Adverse reactions, including abnormal laboratory tests, were reported in 436 (8.92%) of a total of 4,890 patients receiving RHEA cilostazol. (Figures are total cases reported from the time of initial approval up to the completion of reexamination and approval of the additional indication of RHEA cilostazol Tablets 50 and 100 mg.) The following adverse reactions include those reported without information concerning frequency of occurrence after the drug was placed on the market.
Clinically significant adverse reactions: Congestive heart failure, myocardial infarction, angina pectorisNote:, and ventricular tachycardia (frequency unknown*): Congestive heart failure, myocardial infarction, angina pectoris, and ventricular tachycardia may occur. If any signs of these adverse reactions are observed, the drug should be discontinued and appropriate corrective measures should be taken.
Bleeding tendency: Intracranial hemorrhage, such as cerebral hemorrhage (frequency unknown*): Intracranial hemorrhage, such as cerebral hemorrhage, (Early symptoms of intracranial hemorrhage include headache, nausea, vomiting, consciousness disturbance, and hemiplegia) may occur. If any such symptoms occur, the drug should be discontinued and appropriate corrective measures should be taken.
Pulmonary hemorrhage (frequency unknown*), hemorrhage in the digestive tract, epistaxis, and bleeding in the ocular fundus (less than 0.1%): Pulmonary hemorrhage, hemorrhage in the digestive tract, epistaxis, and bleeding in the ocular fundus may occur. If any such symptoms occur, the drug should be discontinued and appropriate corrective measures should be taken.
Pancytopenia, agranulocytosis (frequency unknown*), and thrombocytopenia (less than 0.1%): Pancytopenia, agranulocytosis, and thrombocytopenia may occur. Patients should be closely monitored. If any signs of these adverse reactions are observed, the drug should be discontinued and appropriate corrective measures should be taken.
Interstitial pneumonia (frequency unknown*): Interstitial pneumonia accompanied by fever, cough, dyspnoea, abnormal chest X-rays, and eosinophilia may occur. If any signs of interstitial pneumonia are noted, the drug should be discontinued and appropriate corrective measures, including adrenocorticotropic hormone administration, should be taken.
Hepatic dysfunction (0.1% to less than 5%), and jaundice (frequency unknown*): Hepatic dysfunction, as indicated by elevated AST (GOT), ALT (GPT), Al-P, or LDH, and jaundice may occur. Patients should be closely monitored. If signs of hepatic dysfunction are observed, the drug should be discontinued and appropriate corrective measures should be taken.
Note: In a clinical study to evaluate RHEA cilostazol efficacy in the prevention of recurrence of cerebral infarction, angina pectoris (regardless of drug relationship) was reported in 6 of 516 (1.16%) patients.
*Information concerning frequency of occurrence was not obtained because adverse reactions were either voluntarily reported or occurred outside Japan.
Other adverse reactions: See Table 3.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image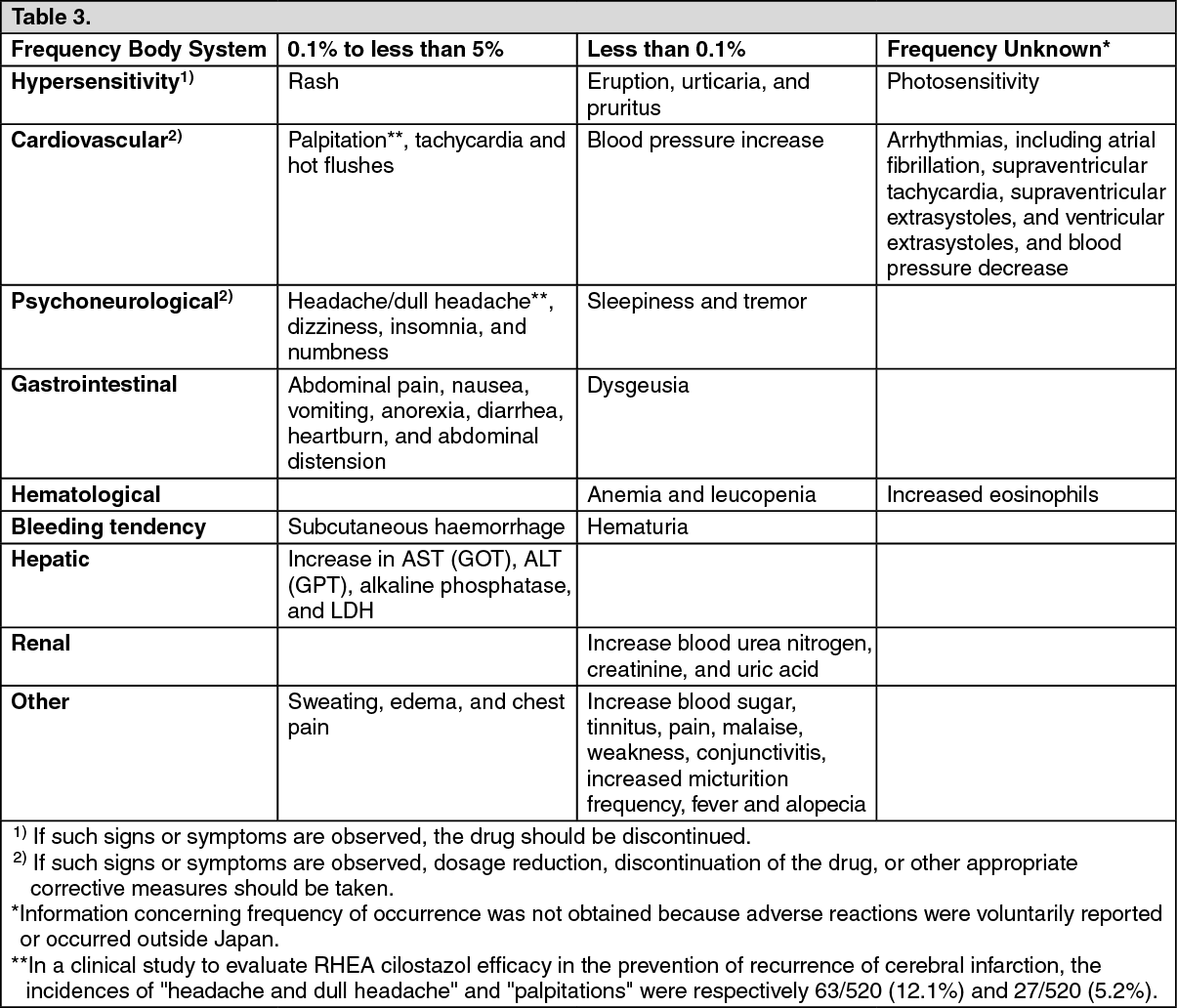 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out