Each vial contains: Cefepime (as hydrochloride) 1 g.
Pharmacology: Pharmacodynamics: Cefepime hydrochloride, USP is a semi-synthetic, broad spectrum, cephalosporin antibiotic for parenteral administration.
Mechanism of Action: Cefepime is a bactericidal agent that acts by inhibition of bacterial cell wall synthesis. Cefepime has a broad spectrum of in vitro activity that encompasses a wide range of Gram-positive and Gram-negative bacteria. Cefepime has a low affinity for chromosomally-encoded beta-lactamases.
Cefepime is highly resistant to hydrolysis by most beta-lactamases and exhibits rapid penetration into Gram-negative bacterial cells. Within bacterial cells, the molecular targets of cefepime are the penicillin binding proteins (PBP).
Cefepime has been shown to be active against most isolates of the following microorganisms, both in vitro and in clinical infections as described in the indications.
Aerobic Gram-Negative Microorganisms: Enterobacter,
Escherichia coli,
Klebsiella pneumonia,
Proteus mirabilis,
Pseudomonas aeruginosa.
Aerobic Gram-Positive Microorganisms:
Staphylococcus aureus (methicillin-susceptible isolates only),
Streptococcus pneumonia,
Streptococcus pyogenes (Lancefield's Group A streptococci), Viridans group streptococci.
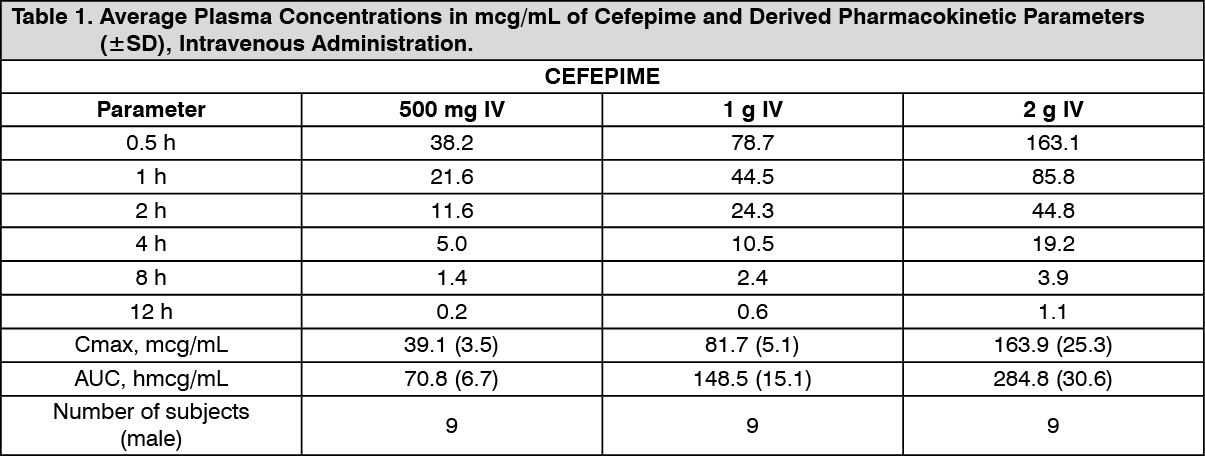
Pharmacokinetics: The average plasma concentrations of cefepime observed in healthy adult male volunteers (n=9) at various times following single 30-minute infusions (IV) of cefepime 500 mg, 1 g, and 2 g are summarized in Table 1. Elimination of cefepime is principally via renal excretion with an average (±SD) half-life of 2.0 (±0.3) hours and total body clearance of 120.0 (±8.0) mL/min in healthy volunteers. Cefepime pharmacokinetics are linear over the range 250 mg to 2 g. There is no evidence of accumulation in healthy adult male volunteers (n=7) receiving clinically relevant doses for a period of 9 days.
Absorption: The average plasma concentrations of cefepime and its derived pharmacokinetic parameters after intravenous (IV) administration are portrayed in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Following intramuscular (IM) administration, cefepime is completely absorbed. The average plasma concentrations of cefepime at various times following a single intramuscular injection are summarized in Table 2. The pharmacokinetics of cefepime are linear over the range of 500 mg to 2 g intramuscularly and do not vary with respect to treatment duration. (See Table 2.)
Click on icon to see table/diagram/image
Distribution: The average steady-state volume of distribution of cefepime is 18.0 (±2.0) L. The serum protein binding of cefepime is approximately 20% and is independent of its concentration in serum.
Cefepime is excreted in human milk. A nursing infant consuming approximately 1000 mL of human milk per day would receive approximately 0.5 mg of cefepime per day.
Concentrations of cefepime achieved in specific tissues and body fluids are listed in Table 3. (See Table 3.)
Click on icon to see table/diagram/image
Used in the treatment of the following infections caused by susceptible strains of the designated microorganisms: 1. Pneumonia (moderate to severe) caused by Streptococcus pneumoniae, including cases associated with concurrent bacteremia, Pseudomonas aeruginosa, Klebsiella pneumoniae, or Enterobacter species.
2. Empiric Therapy for Febrile Neutropenic Patients. Cefepime as monotherapy is indicated for empiric treatment of febrile neutropenic patients. In patients at high risk for severe infection (including patients with a history of recent bone marrow, a transplantation, with hypotension at presentation, with an underlying hematologic malignancy, or with severe or prolonged neutropenia), antimicrobial monotherapy may not be appropriate. Insufficient data exist to support the efficacy of cefepime monotherapy in such patients.
3. Uncomplicated and Complicated Urinary Tract Infections (including pyelonephritis) caused by Escherichia coli or Klebsiella pneumoniae, when the infection is severe, or caused by Escherichia coli, Klebsiella pneumoniae, or Proteus mirabilis, when the infection is mild to moderate, including cases associated with concurrent bacteremia with these microorganisms.
4. Uncomplicated Skin and Skin Structure Infections caused by Staphylococcus aureus (methicillin-susceptible strains only) or Streptococcus pyogenes.
5. Complicated Intra-abdominal Infections (used in combination with metronidazole) caused by Escherichia coli, viridans group streptococci, Pseudomonas aeruginosa, Klebsiella pneumoniae, Enterobacter species, or Bacteroides fragilis.
The recommended adult and pediatric dosages and routes of administration are outlined in the following table. Cefepime should be administered intravenously over approximately 30 minutes. (See Table 4.)
Click on icon to see table/diagram/image
Patients with Hepatic Impairment: No adjustment is necessary for patients with hepatic impairment.
Patients with Renal Impairment: In patients with creatinine clearance less than or equal to 60 mL/min, the dose of Cefepime should be adjusted to compensate for the slower rate of renal elimination. The recommended initial dose of Cefepime should be the same as in patients with normal renal function except in patients undergoing hemodialysis.
The recommended doses of Cefepime in patients with renal impairment are presented in Table 5. When only serum creatinine is available, the following formula (Cockcroft and Gault equation) may be used to estimate creatinine clearance. The serum creatinine should represent a steady state of renal function. (See Table 5.)
Click on icon to see table/diagram/image
In patients undergoing continuous ambulatory peritoneal dialysis, Cefepime may be administered at normally recommended doses at a dosage interval of every 48 hours.
In patients undergoing hemodialysis, approximately 68% of the total amount of cefepime present in the body at the start of dialysis will be removed during a 3-hour dialysis period. The dosage of Cefepime for hemodialysis patients is 1 g on Day 1 followed by 500 mg every 24 hours for the treatment of all infections except febrile neutropenia, which is 1 g every 24 hours.
Cefepime should be administered at the same time each day and following the completion of hemodialysis on hemodialysis days.
Data in pediatric patients with impaired renal function are not available; however, since cefepime pharmacokinetics are similar in adults and pediatric, changes in the dosing regimen proportional to those in adults are recommended for pediatric patients.
Direction for Reconstitution: Dissolve the contents in 10 mL (for intravenous administration) and 2.4 mL (for intramuscular injection) of Sterile Water for Injection or in 0.9% Sodium Chloride or in 5% Dextrose Injection.
Patients who receive an overdose should be carefully observed and given supportive treatment. In the presence of renal insufficiency, hemodialysis, not peritoneal dialysis, is recommended to aid in the removal of cefepime from the body. Accidental overdosing has occurred when large doses were given to patients with impaired renal function. Symptoms of overdose include encephalopathy (disturbance of consciousness including confusion, hallucinations, stupor, and coma), myoclonus, seizures, and neuromuscular excitability.
Contraindicated in patients who have shown immediate hypersensitivity reactions to Cefepime or the cephalosporin class of antibiotics, penicillins or other beta-lactam antibiotics.
Before therapy with Cefepime for injection is instituted, careful inquiry should be made to determine whether the patient has had previous immediate hypersensitivity reactions to cefepime, cephalosporins, penicillins, or other drugs. If this product is to be given to penicillin-sensitive patients, caution should be exercised because cross-hypersensitivity among beta-lactam antibiotics has been clearly documented and may occur in up to 10% of patients with a history of penicillin allergy. If an allergic reaction to cefepime occurs, discontinue the drug. Serious acute hypersensitivity reactions may require treatment with epinephrine and other emergency measures including oxygen, corticosteroids, intravenous fluids, intravenous antihistamines, pressor amines, and airway management, as clinically indicated.
In patients with creatinine clearance less than or equal to 60 mL/min, the dose of Cefepime should be adjusted to compensate for the slower rate of renal elimination. Because high and prolonged serum antibiotic concentrations can occur from usual dosages in patients with renal impairment or other conditions that may compromise renal function, the maintenance dosage should be reduced when cefepime is administered to such patients. Continued dosage should be determined by degree of renal impairment, severity of infection, and susceptibility of the causative organisms. During postmarketing surveillance, serious adverse events have been reported including life-threatening or fatal occurrences of the following: encephalopathy (disturbance of consciousness including confusion, hallucinations, stupor, and coma), myoclonus, and seizures. Most cases occurred in patients with renal impairment who received doses of cefepime that exceeded the recommended dosage schedules. However, some cases of encephalopathy occurred in patients receiving a dosage adjustment for their renal function. In the majority of cases, symptoms of neurotoxicity were reversible and resolved after discontinuation of cefepime and/or after hemodialysis.
Clostridium difficile associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including Cefepime, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
C. difficile produces toxins A and B, which contribute to the development of CDAD. Hypertoxin-producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.
If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.
General: Prescribing Cefepime in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistant bacteria.
As with other antimicrobials, prolonged use of Cefepime may result in overgrowth of nonsusceptible microorganisms. Repeated evaluation of the patient's condition is essential. Should superinfection occur during therapy, appropriate measures should be taken.
Many cephalosporins, including cefepime, have been associated with a fall in prothrombin activity. Those at risk include patients with renal or hepatic impairment, or poor nutritional state, as well as patients receiving a protracted course of antimicrobial therapy. Prothrombin time should be monitored in patients at risk, and exogenous vitamin K administered as indicated.
Positive direct Coombs' tests have been reported during treatment with Cefepime. In hematologic studies or in transfusion cross-matching procedures when antiglobulin tests are performed on the minor side or in Coombs' testing of newborns whose mothers have received cephalosporin antibiotics before parturition, it should be recognized that a positive Coombs' test may be due to the drug.
Cefepime should be prescribed with caution in individuals with a history of gastrointestinal disease, particularly colitis.
Arginine has been shown to alter glucose metabolism and elevate serum potassium transiently when administered at 33 times the amount provided by the maximum recommended human dose of Cefepime. The effect of lower doses is not presently known.
Information for Patients: Patients should be counseled that antibacterial drugs including Cefepime should only be used to treat bacterial infections. They do not treat viral infections (eg, the common cold). When Cefepime is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by Cefepime or other antibacterial drugs in the future.
Diarrhea is a common problem caused by antibiotics, which usually ends when the antibiotic is discontinued. Sometimes after starting treatment with antibiotics, patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as two or more months after having taken the last dose of the antibiotic. If this occurs, patients should contact their physician as soon as possible.
Patients should be advised of neurological adverse events that could occur with Cefepime use. Patients should be instructed to inform their healthcare provider at once of any neurological signs and symptoms, including encephalopathy (disturbance of consciousness including confusion, hallucinations, stupor, and coma), myoclonus, and seizures, for immediate treatment, dosage adjustment, or discontinuation of Cefepime.
Pregnancy: Teratogenic Effects: Pregnancy Category B.
Cefepime was not teratogenic or embryocidal when administered during the period of organogenesis to rats at doses up to 1000 mg/kg/day (1.6 times the recommended maximum human dose calculated on a mg/m2 basis) or to mice at doses up to 1200 mg/kg (approximately equal to the recommended maximum human dose calculated on a mg/m2 basis) or to rabbits at a dose level of 100 mg/kg (0.3 times the recommended maximum human dose calculated on a mg/m2 basis). There are, however, no adequate and well-controlled studies of cefepime use in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
Lactation: Cefepime is excreted in human breast milk in very low concentrations (0.5 mcg/mL). Caution should be exercised when cefepime is administered to a nursing woman.
The following adverse events were thought to be probably related to cefepime during evaluation of the drug in clinical trials conducted in North America (n=3125 cefepime-treated patients). (See Table 6.)
Click on icon to see table/diagram/image
At the higher dose of 2 g every 8 hours, the incidence of probably-related adverse events was higher among the 795 patients who received this dose of cefepime. They consisted of rash (4%), diarrhea (3%), nausea (2%), vomiting (1%), pruritus (1%), fever (1%), and headache (1%).
The following adverse laboratory changes, irrespective of relationship to therapy with cefepime, were seen during clinical trials conducted in North America. (See Table 7.)
Click on icon to see table/diagram/image
A similar safety profile was seen in clinical trials of pediatric patients.
Renal function should be monitored carefully if high doses of aminoglycosides are to be administered with Cefepime because of the increased potential of nephrotoxicity and ototoxicity of aminoglycoside antibiotics. Nephrotoxicity has been reported following concomitant administration of other cephalosporins with potent diuretics such as furosemide.
Store at temperatures not exceeding 30°C.
J01DE01 - cefepime ; Belongs to the class of fourth generation cephalosporins. Used in the systemic treatment of infections.
Megapime Hospi powd for inj 1 g
1's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image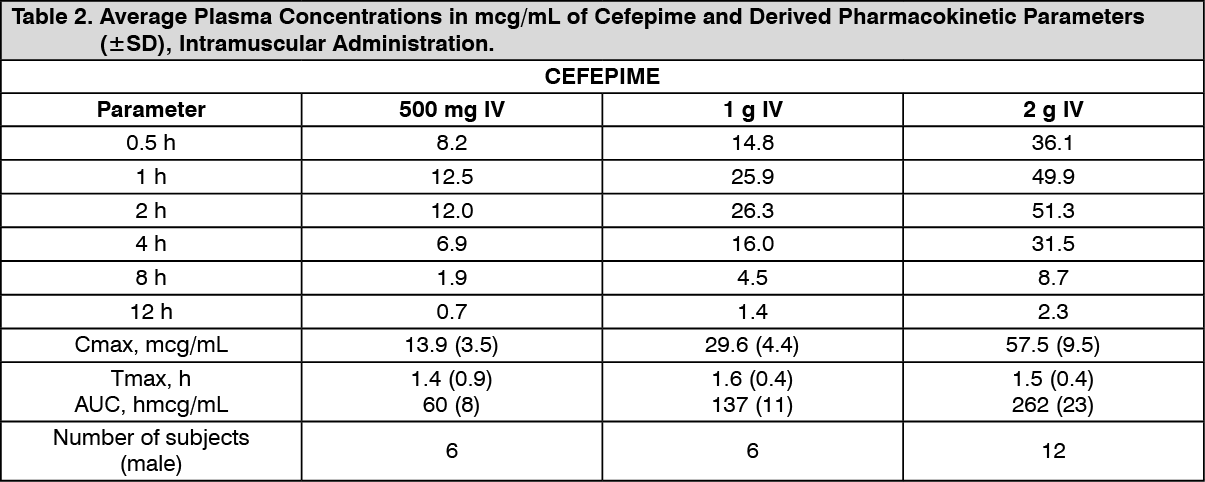 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image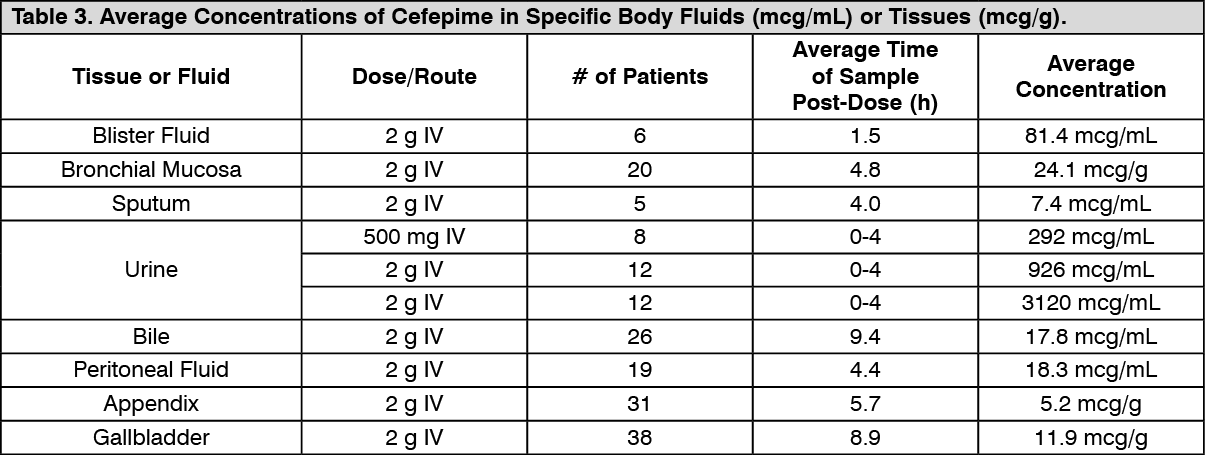 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image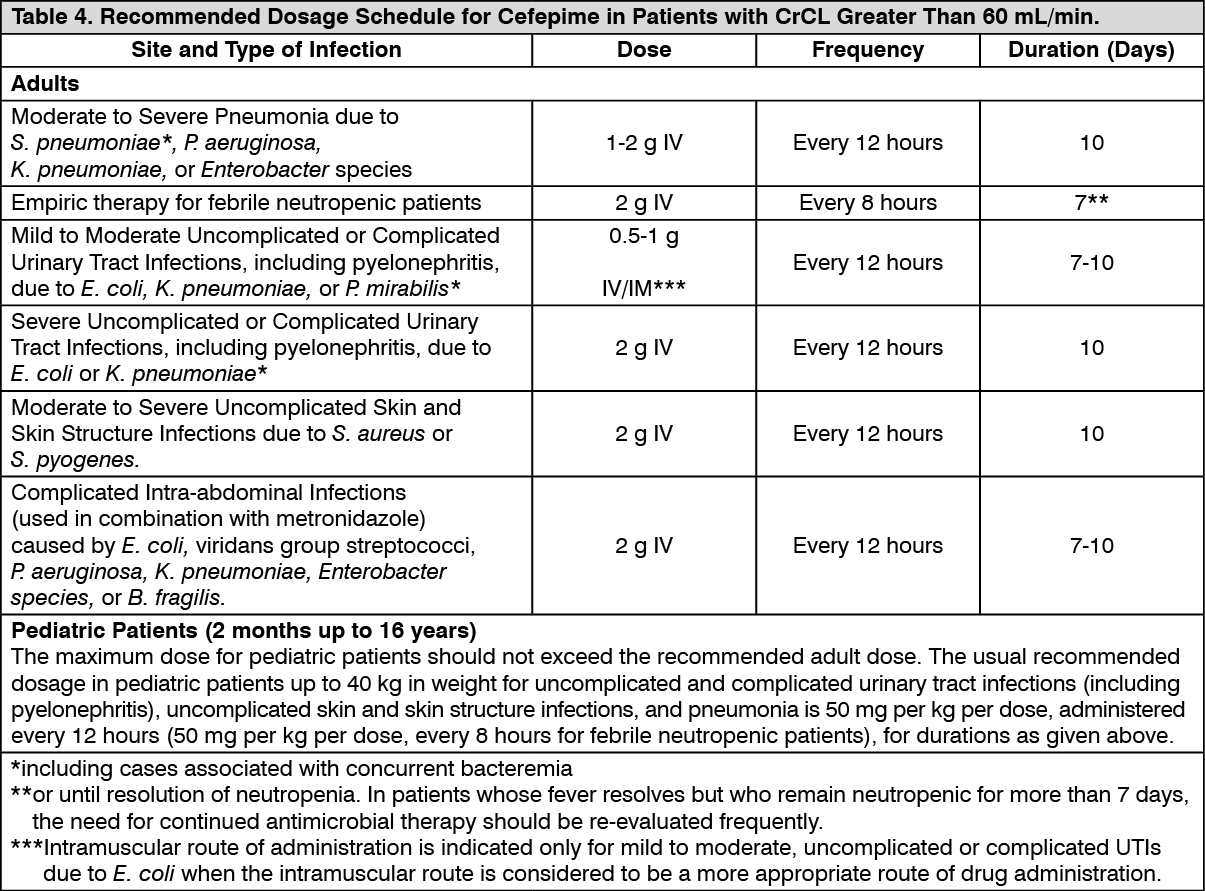 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image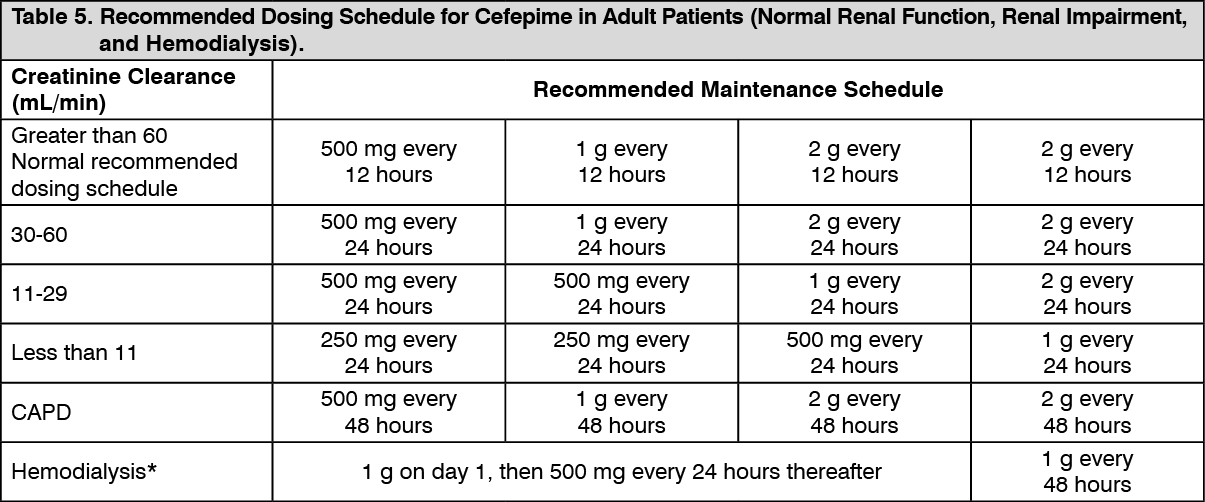 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image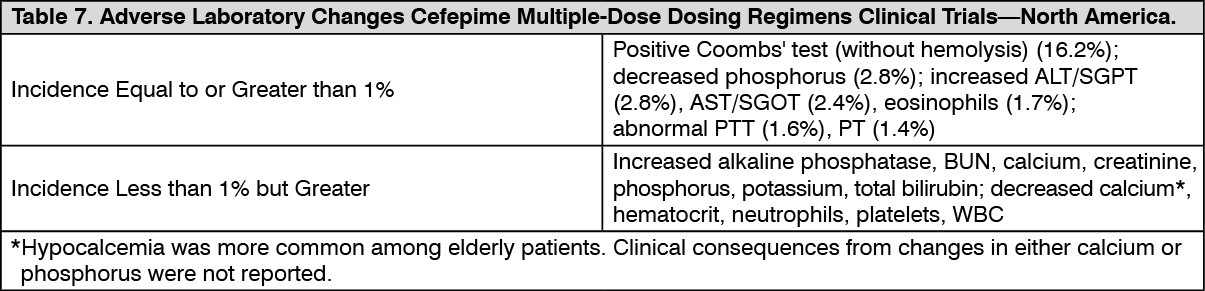 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out