



 Sign Out
Sign Out
Mechanism of Action: Cefepime is a bactericidal agent that acts by inhibition of bacterial cell wall synthesis. Cefepime has a broad spectrum of in vitro activity that encompasses a wide range of Gram-positive and Gram-negative bacteria. Cefepime has a low affinity for chromosomally-encoded beta-lactamases.
Cefepime is highly resistant to hydrolysis by most beta-lactamases and exhibits rapid penetration into Gram-negative bacterial cells. Within bacterial cells, the molecular targets of cefepime are the penicillin binding proteins (PBP).
Cefepime has been shown to be active against most isolates of the following microorganisms, both in vitro and in clinical infections as described in the indications.
Aerobic Gram-Negative Microorganisms: Enterobacter, Escherichia coli, Klebsiella pneumonia, Proteus mirabilis, Pseudomonas aeruginosa.
Aerobic Gram-Positive Microorganisms: Staphylococcus aureus (methicillin-susceptible isolates only), Streptococcus pneumonia, Streptococcus pyogenes (Lancefield's Group A streptococci), Viridans group streptococci.
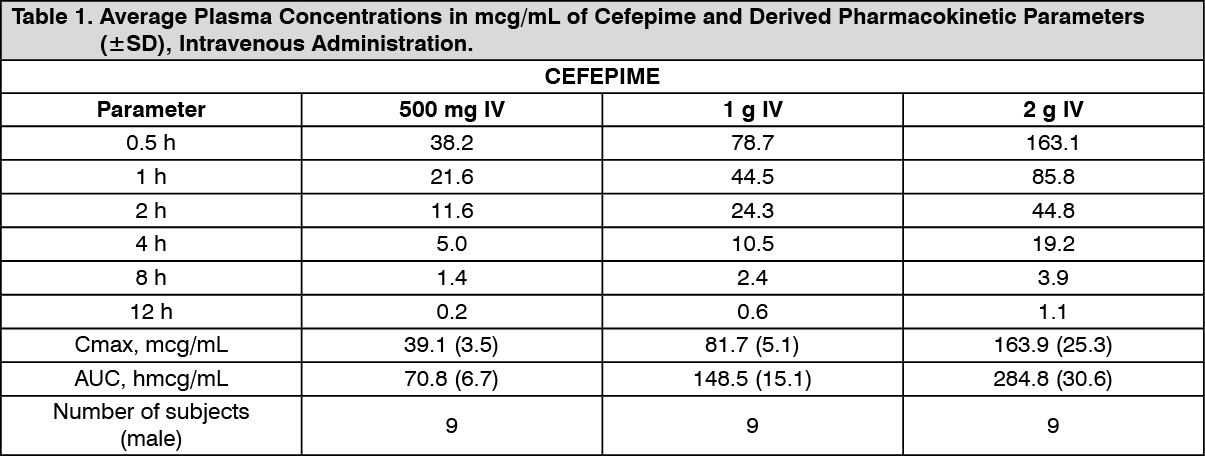
Pharmacokinetics: The average plasma concentrations of cefepime observed in healthy adult male volunteers (n=9) at various times following single 30-minute infusions (IV) of cefepime 500 mg, 1 g, and 2 g are summarized in Table 1. Elimination of cefepime is principally via renal excretion with an average (±SD) half-life of 2.0 (±0.3) hours and total body clearance of 120.0 (±8.0) mL/min in healthy volunteers. Cefepime pharmacokinetics are linear over the range 250 mg to 2 g. There is no evidence of accumulation in healthy adult male volunteers (n=7) receiving clinically relevant doses for a period of 9 days.
Absorption: The average plasma concentrations of cefepime and its derived pharmacokinetic parameters after intravenous (IV) administration are portrayed in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
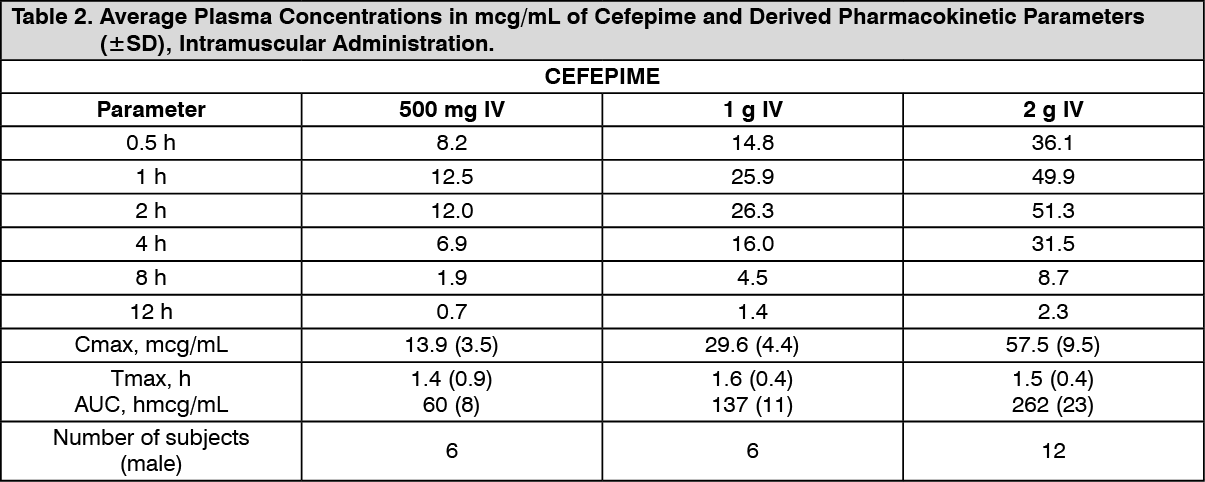
Click on icon to see table/diagram/imageFollowing intramuscular (IM) administration, cefepime is completely absorbed. The average plasma concentrations of cefepime at various times following a single intramuscular injection are summarized in Table 2. The pharmacokinetics of cefepime are linear over the range of 500 mg to 2 g intramuscularly and do not vary with respect to treatment duration. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDistribution: The average steady-state volume of distribution of cefepime is 18.0 (±2.0) L. The serum protein binding of cefepime is approximately 20% and is independent of its concentration in serum.
Cefepime is excreted in human milk. A nursing infant consuming approximately 1000 mL of human milk per day would receive approximately 0.5 mg of cefepime per day.
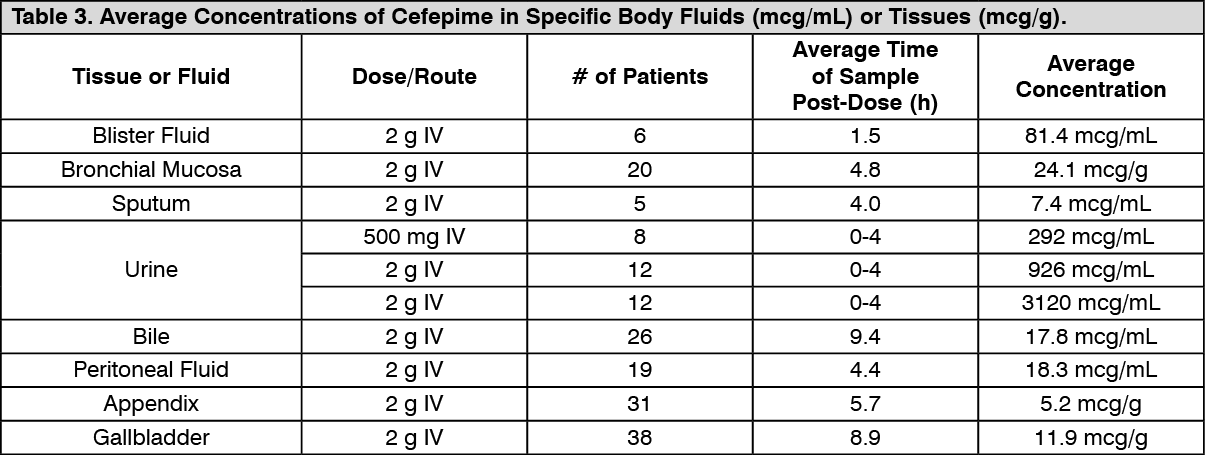
Concentrations of cefepime achieved in specific tissues and body fluids are listed in Table 3. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image