White to off-white granular powder encapsulated in slightly soft and slightly brittle empty gelatin capsule size #0 with Scarlet cap and yellow body.
Each capsule contains: Clindamycin (as hydrochloride monohydrate) 300 mg.
Pharmacology: Pharmacodynamics: Clindamycin is a lincosamide antibiotic that inhibits bacterial protein synthesis. It binds to the 50S ribosomal subunit and affects both ribosome assembly and the translation process.
Pharmacodynamic effects: Efficacy is related to the time period over which the agent level is above the minimum inhibitory concentration (MIC) of the pathogen (%T/MIC).
Resistance: Resistance to clindamycin is most often due to mutations at the rRNA antibiotic binding site or methylation of specific nucleotides in the 23S RNA of the 50S ribosomal unit. These alterations can determine in vitro cross resistance to macrolides and streptogramins B (MLS phenotype). Resistance is occasionally due to alterations in ribosomal proteins. Resistance to clindamycin may be inducible by macrolides in macrolide-resistant bacterial isolates. Inducible resistance can be demonstrated with a disk test (D-zone test) or in broth. Less frequently encountered resistance mechanisms involve modification of the antibiotic and active efflux. There is complete cross resistance between clindamycin and lincomycin. As with many antibiotics, the incidence of resistance varies with the bacterial species and the geographical area. The incidence of resistance to clindamycin is higher among methicillin-resistant staphylococcal isolates and penicillin-resistant pneumococcal isolates than among organisms susceptible to these agents.
Antimicrobial activity: Clindamycin has been shown to have in vitro activity against most isolates of the following organisms.
Aerobic bacteria: Gram-positive bacteria: Staphylococcus aureus (methicillin-susceptible isolates); Coagulase-negative staphylococci (methicillin-susceptible isolates); Streptococcus pneumoniae (penicillin-susceptible isolates); Beta-hemolytic streptococci groups A, B, C, and G; Viridans group streptococci; Corynebacterium spp.
Gram-negative bacteria: Chlamydia trachomatis.
Anaerobic bacteria: Gram-positive bacteria: Actinomyces spp; Clostridium spp. (except Clostridium difficile); Eggerthella (Eubacterium) spp.; Peptococcus spp.; Peptostreptococcus spp. (Finegoldia magna, Micromonas micros); Propionibacterium acnes.
Gram-negative bacteria: Bacteriodes spp.; Fusobacterium spp.; Gardnerella vaginalis, Prevotella spp.
Fungi: Pneumocystis jirovecii.
Protozoans: Toxoplasma gondii; Plasmodium falciparum.
Pharmacokinetics: Some level studies with a 150 mg oral dose of clindamycin hydrochloride in 24 normal adult volunteers showed that clindamycin was rapidly absorbed after oral administration. An average peak serum level of 2.50 mcg/mL was reached in 45 minutes; serum levels averaged 1.51 mcg/mL, at 3 hours and 0.70 mcg/mL at 6 hours. Absorption of an oral dose is virtually complete (90%) and the concomitant administration of food does not appreciably modify the serum concentrations; serum levels have been uniformed and predictable from person to person and dose to dose. Serum level studies following multiple doses of clindamycin hydrochloride for up to 14 days show no evidence of accumulation or altered metabolism of drug. Serum half-life of clindamycin is increased slightly in patients with markedly reduced renal function. Hemodialysis and peritoneal dialysis are not effective in removing clindamycin from the serum, Concentrations of clindamycin in the serum increased linearly with increased dose. Serum levels exceed the MIC (minimum inhibitory concentration) for most indicated organisms for at least six hours following administration of the usually recommended doses. Clindamycin is widely distributed in body fluids and tissues (including bones). In vitro studies in human liver and intestinal microsomes indicated that clindamycin is predominantly oxidized by CYP3A4, with minor contribution from CYP3A5, to form clindamycin sulfoxide and a minor metabolite, N-desmethylclindamycin. The average biological half-life is 2.4 hours. Approximately 10% of the bioactivity is excreted in the urine and 3.6% in the feces; the remainder is excreted as bioinactive metabolites. Doses of up to 2 grams of clindamycin per day for 14 days have been well tolerated by healthy volunteers, except that the incidence of gastrointestinal side effects is greater with the higher doses. No significant levels of clindamycin are attained in the cerebrospinal fluid, even in the presence of inflamed meninges.
Pharmacokinetic studies in elderly volunteers (61-79 years) and younger adults (18-39 years) indicate that age alone does not alter clindamycin pharmacokinetics (clearance, elimination, half-life, volume of distribution, and area under the serum concentration time curve) after oral administration of clindamycin hydrochloride, elimination half-life is increased to approximately 4.0 hours (range 3.4-5.1 h) in the elderly compared to 3.2 hours (range 2.1-4.2 h) in younger adults. The extent of absorption, however, is not different between age groups and no dosage alteration is necessary for the elderly with normal hepatic function and normal (age-adjusted) renal function.
Toxicology: Preclinical safety data: Carcinogenesis: Long term studies in animals have not been performed with clindamycin to evaluate carcinogenic potential.
Mutagenesis: Genotoxicity tests performed included a rat micronucleus test and an Ames Salmonella reversion test. Both tests were negative.
Impairment of Fertility: Fertility studies in rats treated orally with up to 300 mg/kg/day (approximately 11 times the highest recommended adult human dose based on mg/m2) revealed no effects on fertility or mating ability.
In oral embryo fetal development studies in rats and subcutaneous embryo fetal development studies in rats and rabbits, no developmental toxicity was observed except at doses that produced maternal toxicity.
Clindamycin has been shown to be effective in the treatment of the following infections when caused by susceptible anaerobic bacteria; susceptible strains of gram-positive aerobic bacteria such as streptococci, staphylococci and pneumococci; and susceptible strains of Chlamydia trachomatis.
A. Upper respiratory infections including tonsillitis, pharyngitis, sinusitis, otitis media and scarlet fever.
B. Lower respiratory infections including bronchitis, pneumonia, emphysema and lung abscess.
C. Skin and soft tissue infections including acne, furuncles, cellulitis, impetigo, abscesses and wound infections. For specific skin and soft tissue infections like erysipelas and paronychia (panaritium) it would seem logical that these conditions would respond very well to clindamycin therapy.
D. Bone and joint infections including osteomyelitis and septic arthritis.
E. Gynecological infections including endometritis, cellulitis, vaginal cuff infection and tubo-ovarian abscess, salpingitis and pelvic inflammatory disease when given in conjunction with an antibiotic of appropriate gram-negative aerobic spectrum. In cases of cervicitis due to Chlamydia trachomatis, single drug therapy with clindamycin has been shown to be effective in eradication the organism.
F. Intra-abdominal infections including peritonitis and abdominal abscesses when given in conjunction with an antibiotic of appropriate gram-negative aerobic spectrum.
G.Septicemia and endocarditis - The effectiveness of clindamycin in the treatment of selected cases of endocarditis has been documented when clindamycin is determined to be bactericidal to the infecting organism, by in vitro testing of appropriate achievable serum concentrations.
H. Dental infections such as periodontal abscess and periodontitis.
J. Toxoplasmic encephalitis in patients with AIDS. In patients who are intolerant to conventional treatment, clindamycin in combination with pyrimethamine has been shown to be efficacious.
J. Pneumocystis jirovecii (previously classified as Pneumocystis carinii) pneumonia in patients with AIDS. In patients who are intolerant to, or do not respond adequately to conventional treatment, clindamycin may be used in combination with primaquine.
In-vitro susceptibility to clindamycin has been shown for the following organisms: B. melaninogenicus, B. disiens, B. bivius, Peptostreptococcus spp., G. vaginalis, M. mulieris, M. curtisii, and Mycoplasma hominis.
Dosage in Adults: 600-1800 mg/day divided in 2, 3 or 4 equal doses. To avoid the possibility of esophageal irritation, clindamycin HCl capsules should be taken with a full glass of water.
Dosage in Children (over 1 month of age): Clindamycin hydrochloride capsules (for children who are able to swallow capsules): To avoid the possibility of esophageal irritation, clindamycin HCl capsules should be taken with a full glass of water.
Doses of 8-25 mg/kg/day in 3 or 4 equal doses.
Clindamycin capsules are not suitable for children who are unable to swallow them whole.
Dosage in Elderly: Pharmacokinetic studies with clindamycin have shown no clinically important differences between young and elderly subjects with normal hepatic function and normal (age-adjusted) renal function after oral administration. Therefore, dosage adjustments are not necessary in the elderly with normal hepatic function and normal (age-adjusted) renal function.
Dosage in Renal Impairment: Clindamycin dosage modification is not necessary in patients with renal insufficiency.
Dosage in Hepatic Impairment: Clindamycin dosage modification is not necessary in patients with hepatic insufficiency.
Dosage in Specific Indications: Treatment of Beta-Hemolytic Streptococcal Infections: Refer to the dosage recommendations previously mentioned under Dosage in Adults and Dosage in Children. Treatment should be continued for at least 10 days.
Treatment of Chlamydia trachomatis Cervicitis: Clindamycin hydrochloride capsules orally 450-600 mg 4 times daily for 10-14 days.
Treatment of Toxoplasmic Encephalitis in Patients with AIDS: Clindamycin hydrochloride orally 600-1200 mg every 6 hours for 2 weeks followed by 300-600 mg orally every 6 hours. The usual total duration of therapy is 8 to 10 weeks.
Treatment of Pneumocystis carinii Pneumonia in Patients with AIDS: Clindamycin hydrochloride 300 to 450 mg orally every 6 hours for 21 days.
Treatment of Acute Streptococcal Tonsillitis/Pharyngitis: Clindamycin hydrochloride capsules 300 mg orally twice daily for 10 days.
Hemodialysis and peritoneal dialysis are not effective in removing clindamycin from the serum.
Clindamycin is contraindicated in patients previously found to be sensitive to clindamycin or lincomycin or to any of its component.
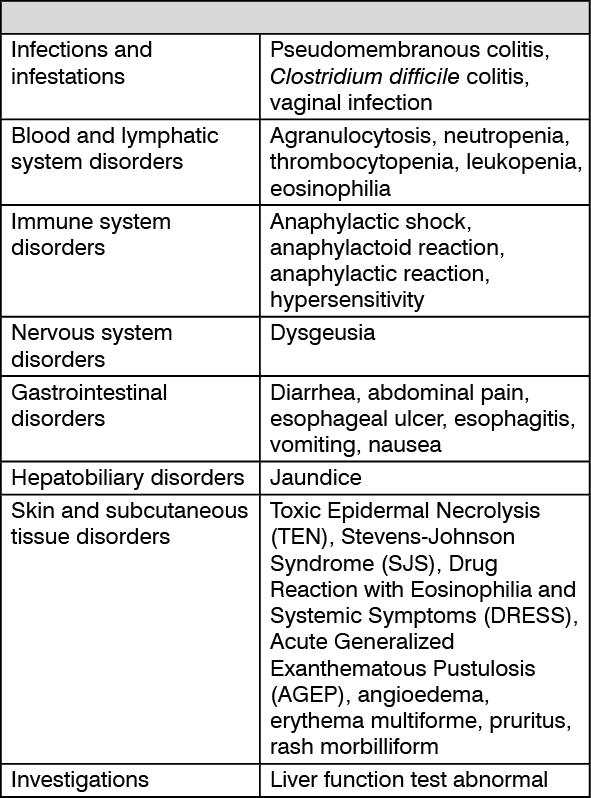
Severe hypersensitivity reactions, including severe skin reactions such as Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS), Stevens-Johnson Syndrome (SJS), Toxic Epidermal Necrolysis (TEN), and Acute Generalized Exanthematous Pustulosis (AGEP) have been reported in patients receiving clindamycin therapy. If a hypersensitivity or severe skin reaction occurs, clindamycin should be discontinued and appropriate therapy should be initiated.
Pseudomembranous colitis has been reported with nearly all antibacterial agents, including clindamycin and may range in severity from mild to life-threatening. Therefore, it is important to consider the diagnosis in patients who present with diarrhea subsequent to the administration of antibacterial agents.
Treatment with antibacterial agents alters the normal flora of the colon and may permit overgrowth of clostridia. Studies indicate that a toxin produced by Clostridium difficile is a primary cause of "antibiotic-associated colitis". After the primary diagnosis of pseudomembranous colitis has been established, therapeutic measures should be initiated. Mild cases of pseudomembranous colitis usually respond to drug discontinuation alone. In moderate-to-severe cases, consideration should be given to management with fluids and electrolytes, protein supplementation, and treatment with an antibacterial drug clinically effective against Clostridium difficile colitis.
Clostridium difficile-associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including clindamycin and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.
If therapy is prolonged, liver and kidney function tests should be performed.
Effects on Ability to Drive and Use Machines: The effect of clindamycin on the ability to drive or operate machinery has not been systematically evaluated.
Pregnancy: Oral and subcutaneous reproductive toxicity studies in rats and rabbits revealed no evidence of impaired fertility or harm to the fetus due to clindamycin, except at doses that caused maternal toxicity. Animal reproduction studies are not always predictive of human response.
Clindamycin crosses the placenta in humans. After multiple doses, amniotic fluid concentrations were approximately 30% of maternal blood concentrations.
In clinical trials with pregnant women, the systemic administration of clindamycin during the second and third trimesters, has not been associated with an increased frequency of congenital abnormalities. There are no adequate and well-controlled studies in pregnant women during the first trimester of pregnancy.
Clindamycin should be used in pregnancy only if clearly needed.
Use in Nursing Mothers: Clindamycin has been reported to appear in human breast milk in ranges from <0.5 to 3.8 μg/mL. Clindamycin has the potential to cause adverse effects on the breastfed infant's gastrointestinal flora such as diarrhea or blood in the stool, or rash. If clindamycin is required by a nursing mother, it is not a reason to discontinue breastfeeding, but an alternate drug may be preferred. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for clindamycin and any potential adverse effects on the breastfed child from clindamycin or from the underlying maternal condition.
See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Clindamycin has been shown to have neuromuscular blocking properties that may enhance the action of other neuromuscular blocking agents. Therefore, it should be used with caution in patients receiving such agents.
Clindamycin is metabolized predominantly by CYP3A4, and to a lesser extent by CYP3A5, to the major metabolite clindamycin sulfoxide and minor metabolite N-desmethylclindamycin. Therefore, inhibitors of CYP3A4 and CYP3A5 may reduce clindamycin clearance and inducers of these isoenzymes may increase clindamycin increase. In the presence of strong CYP3A4 inducers such as rifampicin, monitor for loss of effectiveness.
In vitro studies indicate that clindamycin does not inhibit CYP1A2, CYP2C9, CYP2C19, CYP2E1 or CYP2D6 and only moderately inhibits CYP3A4. Therefore, clinically important interactions between clindamycin and co-administered drugs metabolized by these CYP enzymes are unlikely.
Store at temperatures not exceeding 30°C. Protect from moisture.
G01AA10 - clindamycin ; Belongs to the class of antibiotics. Used in the treatment of gynecological infections.
J01FF01 - clindamycin ; Belongs to the class of lincosamides. Used in the systemic treatment of infections.
Medyclin cap 300 mg
100's




 Sign Out
Sign Out