Body as a Whole: Asthenia, chest pain, edema, facial edema, fatigue, fever, infection, influenza-like disease, orthostatic effects, syncope, trauma.
Cardiovascular: Angina pectoris, arrhythmias including atrial fibrillation, cerebrovascular event/accident, hypotension/orthostatic hypotension, myocardial infarction, second degree AV block, palpitation, sinus bradycardia, sternalgia, tachycardia, ventricular tachycardia, ventricular fibrillation.
Endocrine: Diabetic nephropathy, diabetic vascular disease.
Gastrointestinal: Abdominal pain, anorexia, constipation, dental pain, diarrhea, dry mouth, dyspepsia, flatulence, gastritis, nausea, vomiting.
Hematologics: Hemolysis, anemia, epistaxis, thrombocytopenia (rare).
Liver/Biliary: Liver function abnormalities, hepatitis (rare).
Metabolic and Nutritional and Laboratory Values: Gout, hyperkalemia, hypoglycemia, hyponatremia, weight gain; Elevations of the following: alanine aminotransferase (ALT), BUN, serum creatinine, liver enzymes and/or bilirubin; Reductions of the following: hemoglobin and hematocrit.
Musculoskeletal: Arthralgia, arthritis, fibromyalgia, joint swelling, myalgia, muscle cramps, muscle weakness, pain (back, arm, shoulder, hip, leg, knee, musculoskeletal), stiffness, rhabdomyolysis (rare).
Nervous System/Psychiatric: Dizziness, anxiety, anxiety disorder, ataxia, confusion, depression, dream abnormality, dysgeusia, headache, hypesthesia, insomnia, decreased libido, memory impairment, migraine, nervousness, panic disorder, paresthesia, peripheral neuropathy, sleep disorder, somnolence, tremor, vertigo.
Respiratory: Bronchitis, cough/dry cough, dyspnea, nasal congestion/respiratory congestion, pharyngeal discomfort, pharyngitis, rhinitis, sinusitis/sinus disorder, upper respiratory tract infections.
Skin: Anaphylactic reactions, angioedema (including swelling of the larynx and glossitis, causing airway obstruction and/or swelling of the face, lips, pharynx, and/or tongue), alopecia, cellulitis, dermatitis, dry skin, ecchymosis, erythema, erythroderma, flushing, photosensitivity, pruritus, rash, sweating, superficial peeling of palms, urticaria, vasculitis including Henoch-Schonlein purpura (rare).
Special Senses: Blurred vision, burning/stinging in the eye, cataract, conjunctivitis, taste perversion, tinnitus, decreased visual acuity.
Urogenitals: Impotence, nocturia, urinary frequency, urinary tract infection.



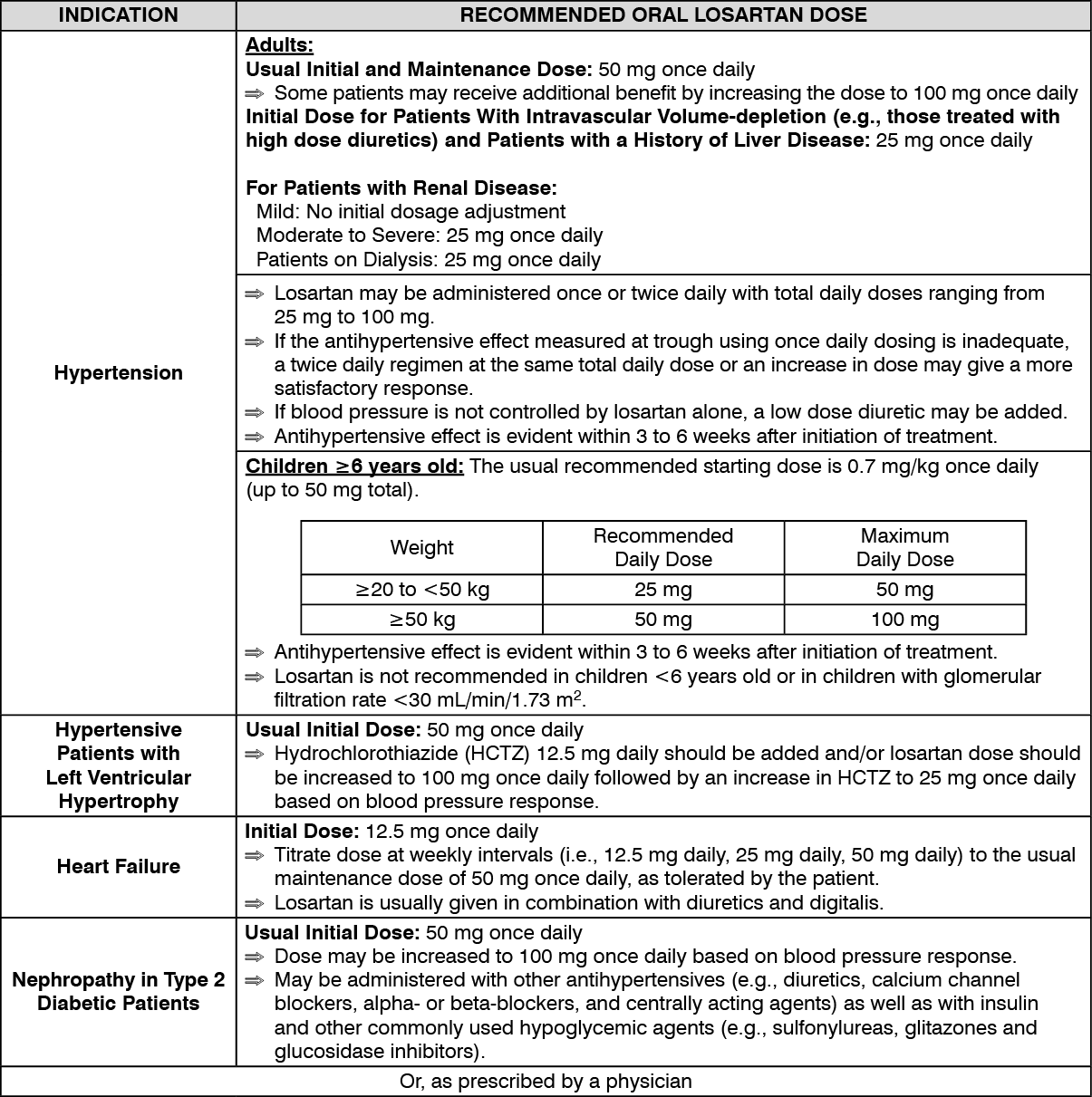 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out