Ticagrelor (Gretor 90) 90 mg is a yellow colored, round, biconvex, film-coated tablet debossed with "G1" on one side arid plain on the other side.
Each film-coated tablet contains: Ticagrelor 90 mg.
Antithrombotic Agent (Platelet Aggregation Inhibitor Excl. Heparin).
Pharmacology: Pharmacodynamics: Mechanism of Action: Ticagrelor is a direct-acting, selective and reversibly binding P2Y12 receptor antagonist that prevents adenosine diphosphate (ADP)-mediated P2Y12 dependent platelet activation and aggregation. Since platelets participate in the initiation of thrombotic complications of atherosclerotic disease, inhibition of platelet function has been shown to reduce risk of cardiovascular events such as CV death, Ml, or stroke. Ticagrelor also increases the local endogenous adenosine levels by inhibiting equilibrative nucleoside transporter-1 (ENT-1) prolonging the half-life of adenosine and thereby increases its local extracellular concentration by providing enhanced local adenosine responses (vasodilation, cardioprotection, platelet inhibition, modulation of inflammation, and induction of dyspnea).
Pharmacodynamic Effects: The benefits associated with Ticagrelor were independent of the use of other cardiovascular therapies including lipid-lowering drugs, beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, Angiotensin II receptor antagonists (AIIRAs), calcium-channel blockers, nitrates, and proton pump inhibitors.
Pharmacokinetics: Ticagrelor demonstrates a linear pharmacokinetics and is approximately dose proportional with its active metabolite (AR-C124910XX).
Absorption: Absorption of ticagrelor occurs with a median tmax of 1.5 h (range 1.0 to 4.0). The formation of the major circulating metabolite AR-C124910XX (active) from ticagrelor occurs with a median tmax of 2.5 h (range 1.5 to 5.0). The mean absolute bioavailability of ticagrelor is about 36% (range 25.4% to 64%). Ingestion of a high-fat meal had no effect on ticagrelor Cmax but resulted in a 21% increase in AUC. The Cmax of its major metabolite was decreased by 22% with no change in AUC. Ticagrelor tablets as crushed tablets mixed in water, given orally or administered through a nasogastric tube into the stomach, is bioequivalent to whole tablets (AUC and Cmax within 80 to 125% for ticagrelor and AR-C124910XX) with a median tmax of 1.0 hour (range 1.0 to 4.0) for ticagrelor and 2.0 hours (range 1.0 to 8.0) for AR-C124910XX.
Distribution: The steady state volume of distribution of ticagrelor is 87.5 L. Ticagrelor and the active metabolite are extensively bound to human plasma proteins (>99%).
Metabolism: CYP3A4 is the major enzyme responsible for ticagrelor metabolism and the formation of its major active metabolite. Ticagrelor and its major active metabolite are weak P-glycoprotein substrates and inhibitors. The systemic exposure to the active metabolite is approximately 30% to 40% of the exposure of ticagrelor.
Excretion: The primary route of ticagrelor elimination is hepatic metabolism. When radiolabeled ticagrelor is administered, the mean recovery of radioactivity is approximately 84% (57.8% in feces, 26.5% in urine). Recoveries of ticagrelor and the active metabolite in urine were both less than 1% of the dose. The primary route of elimination for the major metabolite of ticagrelor is most likely to be biliary secretion. The mean t1/2 is approximately 6.9 hours for ticagrelor and 8.6 hours for the active metabolite.
Specific Populations: Elderly: Higher exposures of Ticagrelor (approximately 60%) and its active metabolite (approximately 50%) were observed in patients ≥65 years of age as compared with younger subjects. These differences are not considered clinically significant.
Pediatric Population: Ticagrelor has not been evaluated in pediatric population.
Gender: Higher exposures to Ticagrelor (approximately 52% for Cmax and 37% for AUC) and its active metabolite (approximately 50%) were observed in women compared to men.
Renal Impairment: Exposure to Ticagrelor was 20% lower and exposure to active metabolite was 17% higher in patients with severe renal impairment compared to subjects with normal renal function. In patients with end-stage renal disease on hemodialysis, Ticagrelor exposure were 38% AUC and 51% Cmax higher on a day without dialysis. A similar increase in exposure was observed immediately prior to dialysis showing that Ticagrelor is not dialysable. No dosing adjustment is required for patients with renal impairment.
Hepatic Impairment: Patient with mild hepatic impairment shows 12% Cmax and 23% AUC exposure to Ticagrelor. Ticagrelor has not been studied in patients with severe hepatic impairment and there is no pharmacokinetic information in patients with moderate hepatic impairment.
Ethnicity: Patients of Asian descent have a 39% higher mean bioavailability compared to Caucasian patients. Black had an 18% lower bioavailability of Ticagrelor. Hispanic and Latino were similar to that in Caucasians.
Ticagrelor 90 mg is indicated for the prevention of thrombotic events (cardiovascular death, myocardial infarction, and stroke) in patients with Acute Coronary syndrome (ACS) - unstable angina, non-ST elevation Myocardial Infarction (NSTEMI) or ST elevation Myocardial Infarction (STEMI), including patients managed medically, and those who are managed with percutaneous coronary intervention (PCI) or coronary artery by-pass graft (CABG).
Ticagrelor tablets can be taken with or without food.
Ticagrelor 90 mg: In the management of ACS, initiate ticagrelor tablets treatment with a 180 mg loading dose (two tablets of 90 mg). Administer 90 mg twice daily during the first year after an ACS event. After one year, administer 60 mg twice daily. Use ticagrelor tablets with a daily maintenance dose of aspirin of 75 to 100.
Do not administer ticagrelor tablets with another oral P2Y12 platelet inhibitor. For patients who are unable to swallow tablets whole, ticagrelor tablets can be crushed, mixed with water and drunk. The mixture can also be administered via a nasogastric tube (CH8 or greater). A patient who misses a dose of ticagrelor tablets should take one tablet (their next dose) at its scheduled time. Premature discontinuation with antiplatelet therapy could result in an increased risk of cardiovascular (CV) death, myocardial infarction (MI), or stroke due to the patient's underlying disease. Physicians who desire to switch patients, with prior ACS event, to Ticagrelor should administer the first dose of Ticagrelor 24 hours following the last dose of the other anti-platelet medication.
Ticagrelor is tolerated in single doses up to 900 mg. There is currently no known treatment to reverse the effects of Ticagrelor, and ticagrelor is not expected to be dialysable. Treatment of overdose should follow local standard medical practice. Bleeding is the expected pharmacologic effect of overdosing. If bleeding occurs, appropriate supportive measures should be taken. Other effects of overdose may include gastrointestinal effects (nausea, vomiting, diarrhea) or ventricular pauses. Monitor the ECG.
Ticagrelor tablets are contraindicated in patients with hypersensitivity (e.g., angioedema) to ticagrelor or any component of the product; in patients with a history of intracranial hemorrhage (ICH) because of a high risk of recurrent ICH in this population; in patients with active pathological bleeding such as peptic ulcer or intracranial hemorrhage; and in patients with severe hepatic impairment.
Risk of Bleeding: Drugs that inhibit platelet function including ticagrelor increase the risk of bleeding. Patient with a propensity to bleed (e.g., due to recent trauma, recent surgery, active or recent GI bleeding, or moderate hepatic impairment) should use Ticagrelor with caution. If possible, manage bleeding without discontinuing ticagrelor. Stopping ticagrelor increases the risk of subsequent cardiovascular events. Consideration should be given to patients with concomitant administration of medicinal products that may increase the risk of bleeding (e.g. non-steroidal anti-inflammatory drugs (NSAIDs), oral anticoagulants, and/or fibrinolytics within 24 hours of ticagrelor dosing. Platelet infusion do not reverse the antiplatelet effect of Ticagrelor in patients with bleeding. Co-administration of Ticagrelor with Desmopressin did not decrease template bleeding time, desmopressin is unlikely to be effective in managing clinical bleeding events. Aminocaproic acid and Tranexamic acid and/or recombinant factor VIIa may augment homeostasis.
Surgery: Because of the reversible binding, restoration of platelet aggregation occurs faster with Ticagrelor. The more rapid offset of effect may predict a reduced risk of bleeding complications (in settings where antiplatelet therapy must be temporarily discontinued due to surgery or trauma). If a patient has to undergo elective surgery and antiplatelet effect is desired, Ticagrelor should be discontinued 5 days prior to surgery.
Patients with Prior Ischemic Stroke: ACS patients with prior ischemic stroke may be treated with Ticagrelor for 12 months only. Caution is advised for treatment beyond one year.
Patients with Moderate Hepatic Impairment: Ticagrelor is contraindicated in patients with severe hepatic impairment. Caution is advised in these patients since there is limited experience with the use of Ticagrelor in this population.
Patients At Risk for Bradyarrhythmia: Increased frequency of mostly asymptomatic ventricular pauses during treatment with Ticagrelor has been reported. Patients with an increased risk of bradycardic events (e.g., patients with sick sinus syndrome w/o pacemaker, 2nd or 3rd degree AV block, or bradycardic-related syncope) must use Ticagrelor with caution due to limited clinical experience.
Dyspnea: Dyspnea usually mild to moderate in intensity and often resolved during continued treatment. There was no indication of an adverse effect on pulmonary function assessed after one month or after at least 6 months of chronic treatment. If a patient develops new, prolonged, or worsened dyspnea that is determined to be related to ticagrelor, no specific treatment is required; continue ticagrelor without interruption if possible. In the case of intolerable dyspnea requiring discontinuation of ticagrelor, consider prescribing another antiplatelet agent.
Thrombotic Thrombocytopenic Purpura: Cases of developing thrombotic thrombocytopenic purpura has been reported very rarely. It is a very serious condition and requires treatment immediately. Use Ticagrelor with caution.
Interference with Laboratory Tests: Use of Ticagrelor may give a false negative result in platelet function test for Heparin-induced thrombocytopenia (HIT). This is related to inhibition of P2Y12-receptor on the healthy donor platelets in the patient's sera/plasma.
Discontinuation of Ticagrelor Tablets: Discontinuation of ticagrelor tablets will increase the risk of myocardial infarction, stroke, and death. If ticagrelor tablets must be temporarily discontinued (e.g., to treat bleeding or for significant surgery), restart it as soon as possible. Resume Ticagrelor tablets as soon as hemostasis is achieved.
Effects on the Ability to Drive and Use Machines: Ticagrelor has no influence on the ability to drive and use machines. During treatment with Ticagrelor, dizziness and confusion have been reported. Therefore, patients who experience these symptoms must exercise caution while driving or using machines.
Pregnancy Category: C
No clinical study has been conducted in pregnant or lactating women. Animal studies do not indicate harmful effects to embryonal/fetal development, parturition, or postnatal development. Ticagrelor should be used during pregnancy only if the potential benefit to the mother justifies any potential risks to the fetus.
It is not known whether Ticagrelor can be secreted into the human milk. Animal studies have shown that ticagrelor and active metabolites are excreted in the milk. The use of Ticagrelor to lactating women is not recommended.
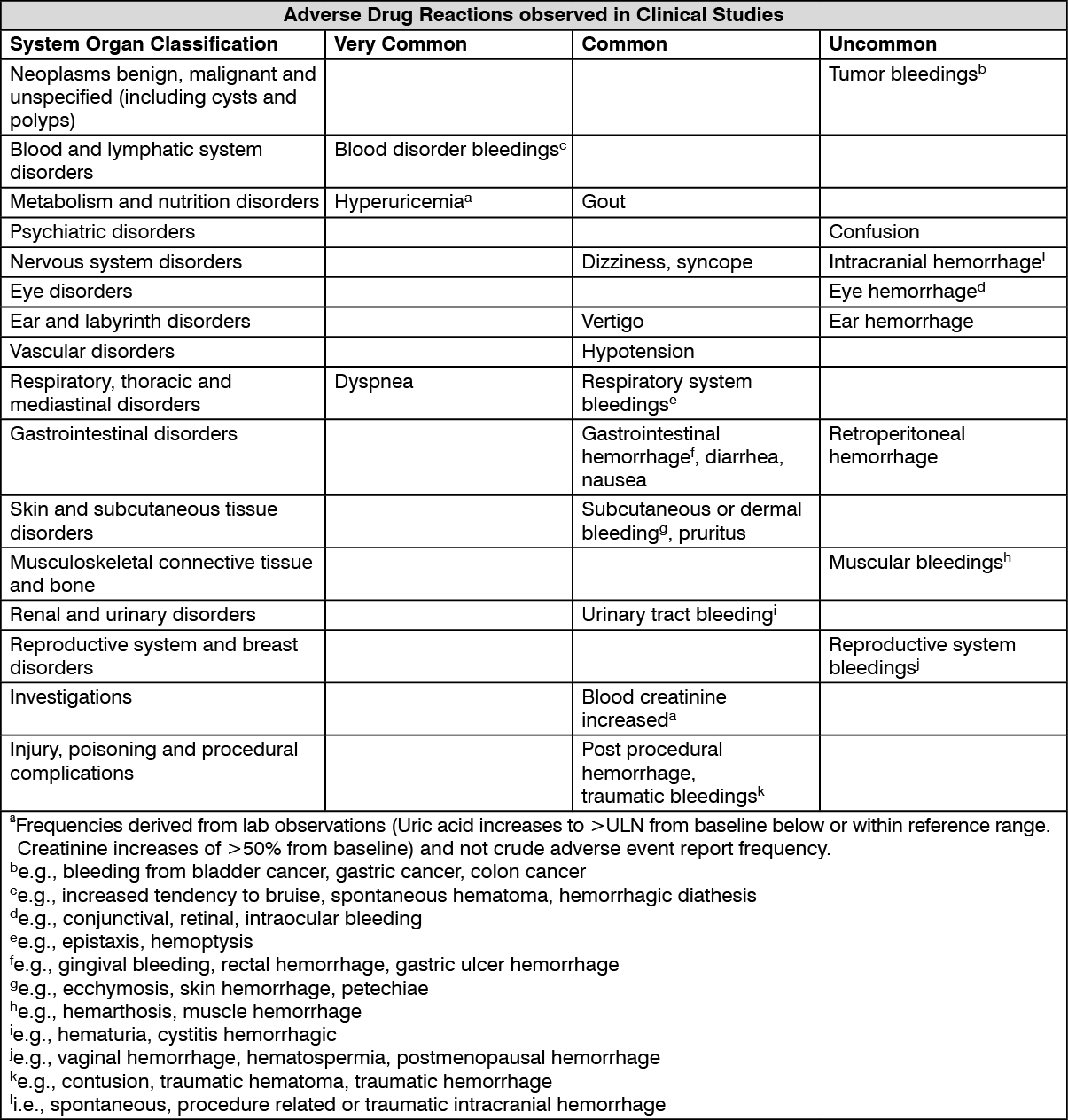
Adverse drug reactions from clinical studies with Ticagrelor are listed by MedDRA System Organ Class (SOC) and frequency category. Within each SOC and frequency category, adverse drug reactions are presented in order of decreasing seriousness. Frequency categories are defined according to the following conventions: Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1000 to <1/100), Rare (≥1/10,000 to <1/1000), Very rare (<1/10,000), Not known (cannot be estimated from the available data). (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
CYP3A Inhibitors: Strong CYP3A inhibitors substantially increase ticagrelor exposure and so increase the risk of dyspnea, bleeding, and other adverse events. Avoid use of strong inhibitors of CYP3A (e.g. ketoconazole, itraconazole, voriconazole, clarithromycin, nefazodone, ritonavir, saquinavir, nelfinavir, indinavir, atazanavir and telithromycin) with Ticagrelor. Moderate CYP3A inhibitors such as amprenavir, aprepitant, diltiazem, erythromycin, fluconazole, and verapamil can be co-administered with Ticagrelor. Cyclosporine (PgP and CYP3A Inhibitor) increases exposure to Ticagrelor while not affecting cyclosporine blood levels.
Strong CYP3A Inducers: Strong CYP3A inducers substantially reduce ticagrelor exposure and so decrease the efficacy of ticagrelor. Avoid use with strong inducers of CYP3A (e.g., rifampin, phenytoin, carbamazepine and phenobarbital).
Aspirin, Enoxaparin and Heparin: Co-administration of Ticagrelor with heparin, enoxaparin, and aspirin do not have any effect on Ticagrelor or the active metabolite plasma levels. Ticagrelor had no effect on heparin based on activated partial thromboplastin time (aPTT) and activated coagulation time (ACT) assays. Ticagrelor had no effect on enoxaparin based on factor Xa assay. Also, co-administration of Ticagrelor and high maintenance dose ASA (>300 mg) is not recommended.
Tolbutamide and Warfarin: Since Ticagrelor is not a CYP2C9 inhibitor, it is unlikely to alter the CYP2C9-mediated metabolism of drugs such as tolbutamide and warfarin.
Opioids: As with other oral P2Y12 inhibitors, co-administration of opioid agonists delays and reduce the absorption of ticagrelor and its active metabolite presumably because of slowed gastric emptying. Consider the use of a parenteral anti-platelet agent in acute coronary syndrome patients requiring co-administration of morphine or other opioid agonists.
Simvastatin, Lovastatin, and Atorvastatin: Ticagrelor increases serum concentrations of simvastatin, lovastatin, and atorvastatin because these drugs are metabolized by CYP3A4. Avoid simvastatin and lovastatin doses greater than 40.
Digoxin: Ticagrelor inhibits the P-glycoprotein transporter; monitor digoxin levels with initiation of or change in ticagrelor therapy.
Oral Contraceptives: Co-administration of Ticagrelor with oral contraceptives (levonorgestrel and ethinyl estradiol) increases exposure of ethinyl estradiol exposure but do not alter the PK of levonorgestrel. No clinically significant effect on oral contraceptives is expected when administered with Ticagrelor.
Store at temperatures not exceeding 30°C.
B01AC24 - ticagrelor ; Belongs to the class of platelet aggregation inhibitors excluding heparin. Used in the treatment of thrombosis.
Gretor 90 FC tab 90 mg
30's (P1,350/box)



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out