Pharmacology: Pharmacodynamics: The pharmacodynamics properties of each drug, irbesartan and amlodipine, provide an addition of antihypertensive effects when administered in combination against the effect observed with both components separately. Both the AT
1 receptor blocker and the calcium channel antagonist decrease blood pressure by reducing the peripheral resistance, but the calcium influx blockade and the vasoconstriction reduction by angiotensin II are complementary mechanisms.
Irbesartan:
Mechanism of action: Irbesartan is a specific antagonist of angiotensin II receptors (AT
1 subtype).
Angiotensin II is an important component of the renin-angiotensin system, it participates in the pathophysiology of hypertension and sodium homeostasis. Irbesartan does not require metabolic activation for its action.
Irbesartan blocks the potent vasoconstriction and aldosterone secreting effects produced by the angiotensin II, by selective antagonism of angiotensin II receptors (AT
1 subtype) localized in vascular smooth muscle cells and in the adrenal cortex. Irbesartan has no agonist activity in the AT
1 receptor and has a much higher affinity (more than 8500-fold) for the AT
1 receptor than for the AT
2 receptor (receptor that has not shown to be associated with cardiovascular homeostasis).
Irbesartan does not inhibit the enzymes in the renin-angiotensin system, i.e., the angiotensin-converting enzyme (ACE), nor affects other hormone receptors or ion channels involved in the cardiovascular regulation of blood pressure and sodium homeostasis. The AT
1 receptors blockade caused by Irbesartan interrupts the feedback loop within the renin-angiotensin system, resulting in increases of plasma levels of renin and angiotensin II. Aldosterone plasma concentrations decline following irbesartan administration, however, serum potassium levels are not significantly affected (mean increase of <0.1 mEq/l) at the recommended doses. Irbesartan has no notable effects on serum triglycerides, cholesterol or glucose concentrations. There is no effect on serum uric acid or urinary uric acid excretion.
Pharmacodynamic Properties: The effect on the decrease in blood pressure by Irbesartan becomes apparent after the first dose and is present in an important way for 1-2 weeks; the maximum effect occurs in 4-6 weeks. In long-term follow-up studies, the effect of irbesartan remained for more than a year.
A single daily dose up to 900 mg produced dose-related drops in blood pressure. The 150-300 mg once a day dose decreases trough blood pressure in supine or sitting position (i.e., 24 hours after taking the dose), at an average of 8-13/5-8 mmHg (systolic/diastolic) higher figures than those observed with placebo. The effects in trough are 60-70% of the corresponding peak diastolic and systolic responses. Optimal effects on blood pressure during the 24 hours are obtained with daily single dose.
Blood pressure decreases approximately to the same degree in both the standing position and the supine position. Orthostatic effects are not frequent, but as with ACE inhibitors, they can be expected in patients who have sodium depletion and/or volume depletion.
Irbesartan blood pressure decreasing effects and the effects of thiazide-type diuretics are added. In patients who are not adequately controlled with irbesartan alone, the addition of a low dose of hydrochlorothiazide (12.5 mg) to irbesartan once a day results in a greater reduction in blood pressure trough compared to 7-10/3-6 mmHg placebo (systolic/diastolic).
Irbesartan effectiveness is not influenced by age or gender. As with other drugs that affect the renin-angiotensin system, black patients have a markedly lower response to monotherapy with Irbesartan. When irbesartan was administered concomitantly with hydrochlorothiazide at low doses (12.5 mg daily), the antihypertensive response in black patients was similar to that of white patients.
After the discontinuation of irbesartan, blood pressure gradually returns to the baseline. Rebound hypertension has not been observed.
Amlodipine:
Mechanism of action: Amlodipine is a calcium dihydropyridine antagonist (calcium ion antagonist or slow-channel blocker) who inhibits the entry of calcium ions and the transmembrane influx of these ions into both the cardiac smooth muscle and the vascular smooth muscle. Amlodipine antihypertensive action mechanism is due to a direct relaxing effect on the vascular smooth muscle. The precise mechanism by which amlodipine alleviates angina symptoms has not been determined, however, amlodipine reduces the total ischemic burden through the following two actions: 1) Amlodipine dilates the peripheral arterioles and, in this way reduces the total peripheral resistance (after load) against which the heart works. Since the heart rate remains stable, this heart discharge reduces myocardial energy consumption and oxygen requirements.
2) Amlodipine mechanism of action probably involves also dilation of the main arteries and coronary arterioles, both in ischemia and normal areas. This dilatation increases the oxygen supply to the myocardium in patients with coronary artery spasm (Prinzmetal's or variant angina).
In patients with hypertension, the administration of a daily dose produces significant reductions in blood pressure, both in standing and supine position for a period of 24 hours. Due to its slow onset of action, acute hypotension is not characteristic of amlodipine administration.
In patients with angina, the administration of amlodipine once a day increases the total time of exercise, the time for the onset of angina, and the time for a depression of 1 mm in the ST segment. In addition, it decreases both the frequency of angina attacks and the consumption of nitroglycerin tablets.
Amlodipine has not been associated with any adverse metabolic effects or changes in plasma lipids and is suitable for use in patients with asthma, diabetes and gout.
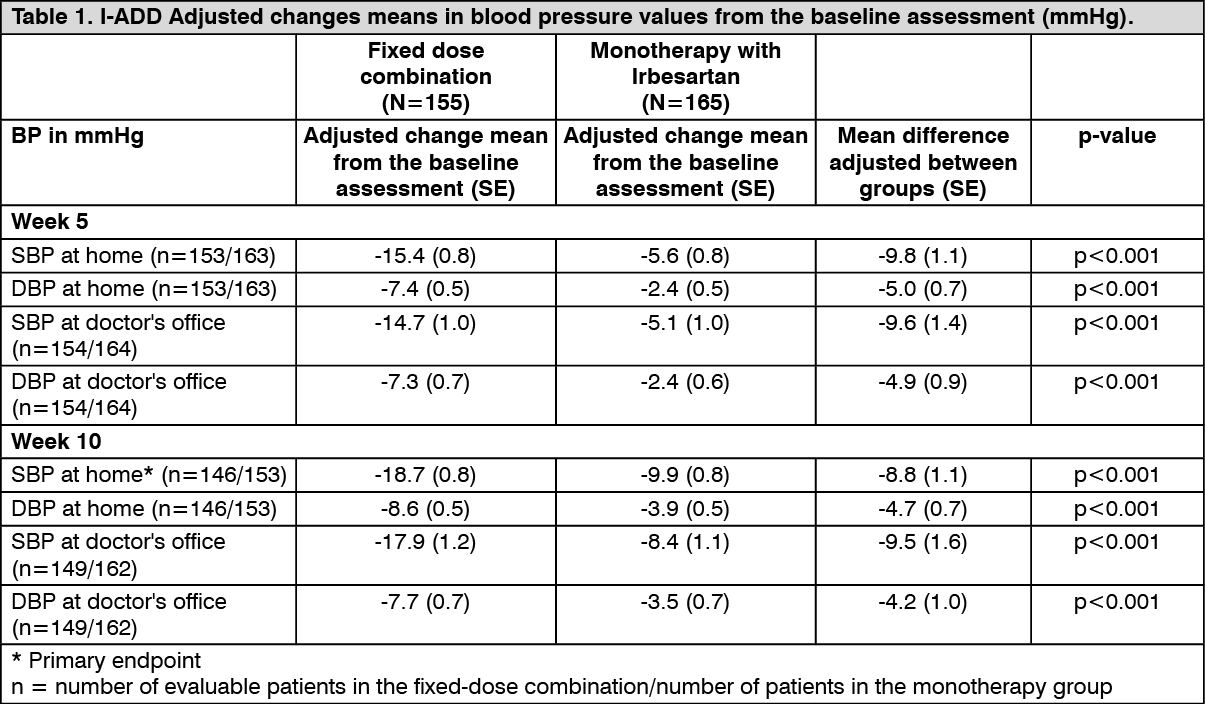
Clinical Efficacy/Clinical Studies: The clinical evidence of efficacy of the irbesartan and amlodipine fixed-dose combination derives from two studies: I-ADD and I-COMBINE. Both were multicenter, prospective, randomized, open, parallel groups, with blind evaluation of the endpoints. The studies were performed in patients with established, uncontrolled essential hypertension [mean systolic blood pressure (SBP) ≥ 145 mmHg] after at least 4 weeks of treatment with irbesartan 150 mg (I-ADD) or amlodipine 5 mg (I-COMBINE)].
Both studies consisted of three treatment periods, A, B and C. During Period A, all patients received 5 mg of amlodipine or 150 mg of Irbesartan, once daily, for 7 to 10 days. At the end of Period A, if the mean SBP of a patient was < 135 mmHg, the patient was withdrawn from the corresponding study.
In the I-ADD study, patients (n = 325) were randomized after Period A to receive 150 mg of Irbesartan or the fixed dose combination of 150 mg/5 mg of irbesartan/amlodipine once daily for 5 weeks (Period B). In Week 5, doses were increased (forced titration) to 300 mg of Irbesartan or 300 mg/5 mg of the fixed dose combination of Irbesartan/amlodipine once daily and continued for 5 weeks.
In the I-COMBINE study, patients (n = 290) were randomized after period A to receive 5 mg of amlodipine or the fixed dose combination of 150 mg/5 mg of Irbesartan/amlodipine once daily for 5 weeks (Period B). At week 5, doses were increased (forced titration) to 10 mg of amlodipine or the fixed dose combination of 150 mg/10 mg Irbesartan/amlodipine once daily and continued for 5 weeks (Period C).
In the I-ADD study, the primary endpoint was the change in the SBP measured at home at Week 10. In the I-COMBINE study, the primary endpoint was the change in the SBP measured at home in Week 5. Secondary endpoints were diastolic blood pressure (DBP), measured at home and office blood pressure measurements (OBPM), as well as the percentage of controlled patients (mean SBP measured at home < 135 mmHg) and patients with a response (mean SBP measured at home < 135 mmHg and average of DBP measured at home < 85 mmHg) at Week 10 for both studies.
The results of both studies demonstrated a significantly greater efficacy of the fixed dose combination with respect to amlodipine or irbesartan alone (see Tables 1 and 2).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: Irbesartan/Amlodipine combination:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: Irbesartan/Amlodipine combination: The concurrent administration of Irbesartan and amlodipine, either in a fixed dose combination tablet or the free dose combination, has no influence on the bioavailability of the individual components.
The three fixed-dose combinations of Irbesartan and amlodipine (150 mg/10 mg, 300 mg/5 mg, and 300 mg/10 mg) are bioequivalent to free-dose combinations (150 mg/10 mg, 300 mg/5 mg, and 300 mg/10 mg) both in terms of speed and of absorption degree.
When administered separately or concomitantly at 300 mg and 10 mg dose levels, the time until the average plasma peak concentrations of Irbesartan and amlodipine remains unchanged, i.e., 0.75-1 hour and 5 hours respectively after administration. Similarly, C
max and AUC are in the same range resulting in a relative bioavailability of 95% for Irbesartan and 98% for amlodipine when administered in combination.
The mean half-life values for Irbesartan and amlodipine, administered alone or in combination, are similar: 17.6 hours against 17.7 hours for Irbesartan and 58.5 hours against 52.1 hours for amlodipine. The elimination of Irbesartan and amlodipine is unchanged when drugs are administered alone or concomitantly.
The pharmacokinetics of both drugs appear to be linear in the range of doses administered together (i.e., between 150 mg and 300 mg for Irbesartan and between 5 mg and 10 mg for amlodipine).
Irbesartan: Irbesartan is an orally active agent and does not require biotransformation for its activity. After oral administration, Irbesartan is rapidly and completely absorbed. Peak plasma concentrations occurs from 1.5 to 2 hours after oral administration. The absolute bioavailability of Irbesartan administered orally is 60-80%. Food does not affect the bioavailability of Irbesartan.
Irbesartan is approximately 96% protein-bound in plasma, and has negligible binding to cellular components of blood. The distribution volume is 53-93 L/Kg.
In plasma, unchanged Irbesartan accounts for 80-85% of the circulating radioactivity after oral or intravenous administration of Irbesartan C
14. Irbesartan is metabolized in the liver via glucuronide conjugation and oxidation. Its main circulating metabolite is Irbesartan glucuronide (approximately 6%). Irbesartan conjugation and oxidation, mainly by the cytochrome P450 isoenzyme CYP2C9; the CYP3A4 isoenzyme has a negligible effect. Irbesartan is not metabolized by most of the isoenzymes commonly involved in drug metabolism, nor induces or inhibits them substantially (i.e., CYP1A1, CYP1A2, CYP2A6, CYP2B6, CYP2D6, or CYP2E1). Irbesartan does not induce or inhibit the CYP3A4 isoenzyme.
Irbesartan and its metabolites are excreted by both biliary and renal routes. About 20% of the radioactivity administered after a dose of Irbesartan C
14, orally or intravenously, is recovered in the urine and the rest in the feces. Less than 2% of the dose is excreted in the urine as Irbesartan without change.
Irbesartan terminal elimination half-life (t
½) is 11-15 hours. The total body clearance of intravenously administered irbesartan is 157-176 mL/min, of which 3.0 to 3.5 mL/min are by renal clearance. Irbesartan exhibits a linear pharmacokinetics over the limits of the therapeutic dose. Steady-state plasma concentrations are reached within three days of the start of the once a day dosing regimen. The limited accumulation (<20%) was observed in plasma when the daily dose was repeated.
In hypertensive individuals, higher concentrations of Irbesartan were observed in plasma (11-44%) in women than in men; however, after multiple doses, no differences were observed in terms of accumulation or elimination half-life between men and women. No gender-specific differences have been observed regarding the clinical effect.
In elderly normotensive subjects (men and women) (65-80 years old) with clinically normal renal and hepatic function, AUC and peak plasma concentrations (C
max) of Irbesartan were approximately 20 to 50% higher than those observed in the younger subjects (18 to 40 years old). Regardless of age, the elimination half-life is similar.
No significant differences have been observed related to age regarding the clinical effect.
In black and white normotensive subjects, Irbesartan AUC in plasma and terminal elimination half-life (t
½) are approximately 20 to 25% higher in blacks than whites; Irbesartan peak plasma concentrations (C
max) were basically equivalent.
In patients with renal impairment (regardless of degree) and in patients on hemodialysis, Irbesartan pharmacokinetics did not change significantly. Irbesartan is not removed by hemodialysis.
In patients with hepatic insufficiency due to mild to moderate cirrhosis, the pharmacokinetics of Irbesartan was not significantly affected.
Amlodipine: After oral administration of therapeutic doses, amlodipine is well absorbed, with maximum blood levels between 6 to 12 hours after dose administration. It has been estimated that the absolute bioavailability is 64 to 90%. The volume of distribution is approximately 21 L/Kg. In vitro studies have shown approximately 97.5% circulating amlodipine is bound to plasma proteins. Absorption of amlodipine is not affected by food intake.
The plasma terminal elimination half-life is around 35 to 50 hours in consistency with the dosage once a day. Amlodipine is extensively metabolized by the liver forming inactive metabolites, 10% of the original compound and 60% as metabolites excreted in the urine.
Special Populations: Irbesartan and Amlodipine combination:
Pediatric patients: No information available for the fixed dose combination.
Amlodipine:
Use in the Elderly: The time to obtain the maximum plasma concentrations of amlodipine is similar between elderly and young patients. Clearance of amlodipine tends to be reduced with resulting increases in the AUC and the elimination half-life in elderly patients. The increased AUC and elimination half-life in patients with congestive heart failure were as hoped for the age group studied.
The increases in the AUC and in the mean route of elimination in patients with congestive heart failure occurred as expected in this age group.
Pediatric patients: A pharmacokinetic study has been conducted in 74 hypertensive children between 12 months to 17 years of age (with 34 patients from 6 to 12 years of age and 28 patients from 13 to 17 years of age) receiving amlodipine doses between 1.25 and 20 mg administered once a day or twice a day.
In children 6 to 12 years of age and adolescents 13-17 years of age, typical oral clearance (CL/F) was 22.5 and 27.4 L/h respectively in male individuals and 16.4 and 21.3 L/h respectively in the female individuals. A great variability in exposure among people was observed. The data reported in children under 6 years of age are limited.
Use in patients with hypertension: A randomised, double-blind study of morbidity and mortality called the Antihypertensive and Lipid-Lowering treatment to prevent Heart Attack Trial (ALLHAT) was conducted to compare the new pharmacological treatments: amlodipine 2.5-10 mg/day (calcium-channel blocker) or lisinopril 10-40 mg/day (ACE inhibitor) as first-line thiadiuretic treatment, chlortalidone 12.5-25 mg/day for mild-to-moderate hypertension.
A total of 33,357 hypertensive patients aged 55 years and above were randomised and monitored for an average of 4.9 years.
Patients had at least one additional risk factor for coronary artery disease, including: previous myocardial infarction or cerebrovascular accident (> 6 months before enrolment) or a record of another CHD with atherosclerosis (51.5% overall), type 2 diabetes (36.1%), C-HDL < 35 mg/dL (11.6%), left ventricular hypertrophy diagnosed by electrocardiogram or echocardiogram (20.9%), current smoker (21.9%).
The primary endpoint was a composite of fatal heart disease or non-fatal myocardial infarction. There was no significant difference in the primary endpoint between amlodipine-based treatment and chlortalidone-based treatment. RR 0.98 CI 95% (0.90 to 1.07) p = 0.65. Of the secondary endpoints, the incidence of heart failure (component of a combined cardiovascular endpoint) was significantly greater in the amlodipine group compared to the chlortalidone group (10.2% vs. 7.7%, RR 1.38, CI 95% [1.25-1.52] p <0.001). However, there were no significant differences in all-cause mortality between the amlodipine-based treatment and the chlortalidone-based treatment. RR 0.96 CI 95% [0.89-1.02] p = 0.20.
Use in patients with heart failure: In hemodynamic studies and controlled clinical studies based on exercise in patients with NYHA class II-IV heart failure, it has been shown that amlodipine does not lead to clinical deterioration determined by tolerance to exercise, left ventricular ejection fraction and clinical symptoms.
A placebo-controlled study (PRAISE) designed to evaluate patients with NYHA class III-IV heart failure receiving digoxin, diuretics and ACE inhibitors, showed that amlodipine does not lead to an increased risk of mortality or combined mortality and morbidity with heart failure. In a large-scale, placebo-controlled follow-up study (PRAISE-2) of amlodipine in patients with NYHA III and IV heart failure without clinical symptoms or objective findings of suggestive or underlying ischemic disease, at stable doses of ACE inhibitors, digitalis and diuretics, amlodipine had no effect on overall cardiovascular mortality. In this same population, amlodipine was associated with more reports of pulmonary oedema.
Pediatric population: In a study involving 268 children aged between 6 and 17 years with predominantly secondary hypertension, the comparison of one dose of 2.5 mg and one dose of 5.0 mg of amlodipine with placebo, showed that both doses reduced systolic artery pressure significantly more than the placebo. The difference between the doses was not statistically significant. The long-term effects of amlodipine on growth, puberty and overall development have not been studied. The long-term efficacy of amlodipine treatment in childhood in reducing cardiovascular morbidity and mortality in adulthood has also not been established.
Patients with liver failure: Very limited clinical data exists on the administration of amlodipine in patients with liver failure. Patients with liver failure have reduced amlodipine clearance, resulting in a longer half-life and an increase in the AUC of approximately 40-60%.
Toxicology: Precautions related to Carcinogenesis, Mutagenesis, Teratogenesis Effects and Fertility: Irbesartan: No evidence of carcinogenicity was observed when Irbesartan was administered at doses up to 500/1,000 mg/Kg/day in rats (males/females, respectively) and 1,000 mg/Kg/day in mice for two years. These doses produced a systemic exposure 4-25 times (rats) and 4-6 times (mice) greater than exposure in humans who received 300 mg daily.
Irbesartan was not mutagenic in a battery of in vitro tests (Ames microbial test, rat hepatocyte DNA repair test, mammalian V79 premature gene mutation test). Irbesartan was negative in several tests for induction of chromosomal aberrations (human lymphocyte assay, in vitro, mouse micronucleus study, in vivo).
Fertility and reproduction were not affected in studies of male and female rats, even with doses that cause some toxicity in the parents (up to 650 mg/Kg/day). No significant effects were observed in the number of corpora lutea, implants or live fetuses. Irbesartan did not affect the survival, development or reproduction of the offspring.
At doses of 50 mg/Kg/day and greater, transient effects (increased renal pelvic cavitation, hydroureter or subcutaneous edema) were observed in the fetuses of rats, which resolved after birth. In rabbits, maternal mortality, abortion, and early fetal resorption were observed, with a dose of 30 mg/Kg/day. No other teratogenic effects were observed in rats or rabbits.
Amlodipine: Carcinogenesis: Rats and mice treated with amlodipine in the diet for two years at concentrations calculated to provide daily dosage levels of 0.5, 1.25 and 2.5 mg/Kg/day showed no evidence of carcinogenicity. The highest dose (for mice, similar to, and for rats, double* the maximum recommended clinical dose of 10 mg on a mg/m
2 basis) was close to the maximum tolerated dose for mice but not for rats.
Mutagenesis: Mutagenicity studies did not reveal any effect related to amlodipine at gene or chromosome level.
Infertility: There was no effect on fertility in rats treated with amlodipine (males for 64 days and females 14 days before mating) at doses up to 10 mg/Kg/day (8 times* the maximum recommended human dose of 10 mg in mg/m
2 base).
In another study in rats in which the male rats were treated with amlodipine besylate for 30 days at a dose comparable to the dose in humans based on mg/kg, a reduction in plasma of follicle-stimulating hormone and testosterone levels was seen, in addition to a reduction in the density spermatozoids and in the number of mature spermatids and Sertoli cells. (*Based on a 50 kg patient.)



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image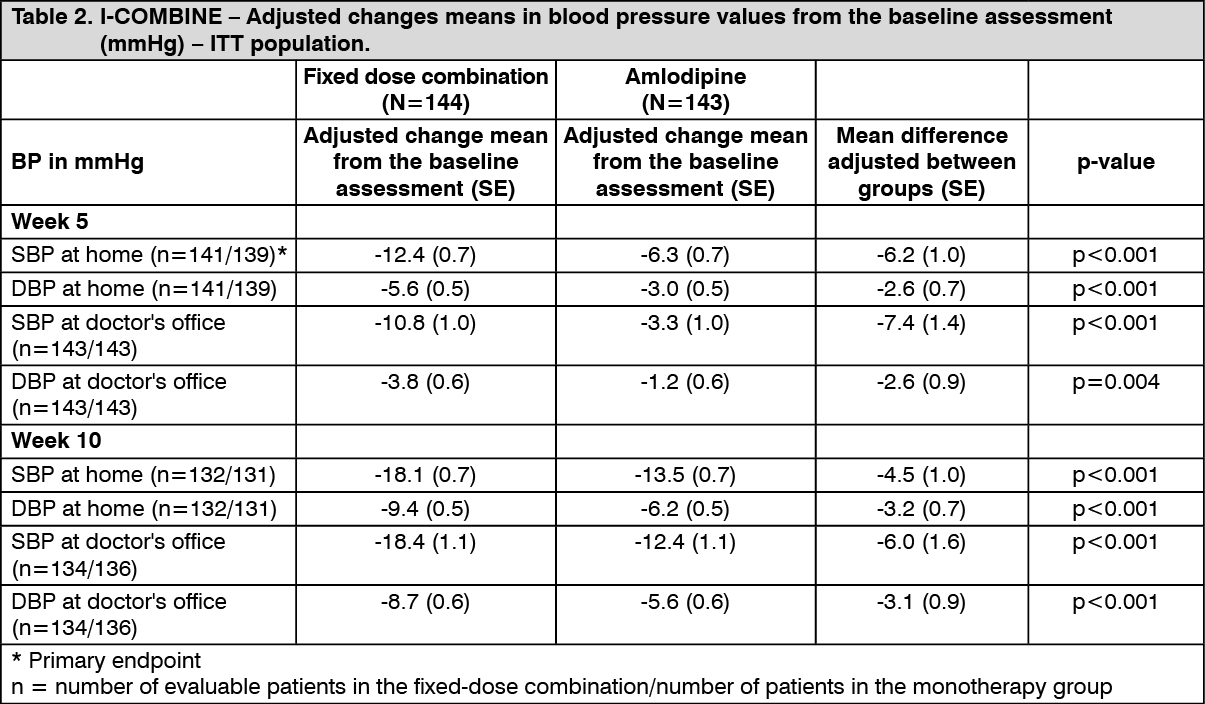 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out