Apixaban Tablets 2.5 mg: Yellow, round shaped, biconvex, film-coated tablet debossed with "IU1" on one side and plain on other side.
Apixaban Tablets 5 mg: Pink, oval shaped, biconvex, film-coated tablet debossed with "IU2" on one side and plain on other side.
Each film-coated tablet contains: Apixaban 2.5 mg or Apixaban 5 mg.
Antithrombotic agent.
Pharmacology: Pharmacodynamics: Apixaban is a selective inhibitor of FXa. It does not require antithrombin III for antithrombotic activity. Apixaban inhibits free and clot-bound FXa, and prothrombinase activity. Apixaban has no direct effect on platelet aggregation, but indirectly inhibits platelet aggregation induced by thrombin. By inhibiting FXa, apixaban decreases thrombin generation and thrombus development. As a result of FXa inhibition, apixaban prolongs clotting tests such as prothrombin time (PT), INR, and activated partial thromboplastin time (aPTT). Changes observed in these clotting tests at the expected therapeutic dose, however, are small, subject to high degree of variability, and not useful in monitoring the anticoagulation effect of apixaban.
Pharmacokinetics: Apixaban demonstrates linear pharmacokinetics with dose-proportional increases in exposure for oral doses up to 10 mg.
Absorption: The absolute bioavailability of apixaban is approximately 50% for doses up to 10 mg of apixaban. Food does not affect the bioavailability of apixaban. Maximum concentrations (Cmax) of apixaban appear 3 to 4 hours after oral administration of apixaban. At doses ≥25 mg, apixaban displays dissolution-limited absorption with decreased bioavailability.
Distribution: Plasma protein binding in humans is approximately 87%. The volume of distribution (Vss) is approximately 21 liters.
Metabolism: Approximately 25% of an orally administered apixaban dose is recovered in urine and feces as metabolites. Apixaban is metabolized mainly via CYP3A4 with minor contributions from CYP1A2, 2C8, 2C9, and 2J2. O-demethylation and hydroxylation at the 3-oxopiperidinyl moiety are the major sites of biotransformation.
Elimination: Apixaban is eliminated in both urine and feces. Renal excretion accounts for about 27% of total clearance. Biliary and direct intestinal excretion contributes to elimination of apixaban in the feces.
Prevention of VTE in adults who have undergone elective hip or knee replacement surgery. Reduced the risk of stroke, systemic embolism, & death in patients with nonvalvular atrial fibrillation (NVAF) with ≥1 risk factors, including patients unsuitable for warfarin. Treatment & prevention (recurrent) of DVT & pulmonary embolism (PE).
Prevention of VTE in elective hip or knee replacement surgery: 2.5 mg bid. Initial dose should be taken 12-24 hours after surgery. Recommended duration of treatment: 32-38 days for hip replacement surgery & 10-14 days for knee replacement surgery.
Prevention of stroke & systemic embolism in Patient with NVAF: 5 mg bid.
Patient with at least 2 of the following characteristics: ≥80 yr, ≤60 kg, or serum creatinine ≥1.5 mg/dL (133 mmol/L): 2.5 mg bid.
DVT & PE: 10 mg bid for 7 days, followed by 5 mg bid.
Prevention of recurrent DVT & PE: 2.5 mg bid after at least 6 month of treatment for DVT or PE.
Surgery & invasive procedures: Patient not previously treated with anticoagulants: At least 5 doses of 5 mg bid (2.5 mg bid in patient who qualify for dose reduction) should be given before cardioversion to ensure adequate anticoagulation. If cardioversion is required before 5 doses of Apixaban: 10 mg loading dose, followed by 5 mg bid. Reduce to 5 mg loading dose, followed by 2.5 mg bid if the patient meets the criteria for dose reduction. Loading dose should be given at least 2 hours before cardioversion.
Method of Administration: May be taken with or without food. For patient with swallowing difficulties, crush tab & suspend in water, 5% dextrose in water (D5W), apple juice or mixed with applesauce. Drink immediately. Solution stable for 4 hours. Alternatively, crush & suspend in 60 mL water or D5W & administer via nasogastric tube.
There is no antidote to apixaban. Overdose of apixaban may result in a higher risk of bleeding. In the event of hemorrhagic complications, treatment must be discontinued and the source of bleeding investigated. The initiation of appropriate treatment, eg., surgical hemostasis or the transfusion of fresh frozen plasma should be considered.
In controlled clinical trials, orally-administered apixaban in healthy subjects at doses up to 50 mg daily for 3 to 7 days (25 mg twice daily (bid) for 7 days or 50 mg once daily (od) for 3 days) had no clinically relevant adverse effects.
Administration of activated charcoal 2 and 6 hours after ingestion of a 20-mg dose of Apixaban reduced mean Apixaban AUC by 50% and 27%, respectively, and had no impact on Cmax. Mean half-life of Apixaban decreased from 13.4 hours when Apixaban was administered alone to 5.3 hours and 4.9 hours, respectively, when activated charcoal was administered 2 and 6 hours after Apixaban. Thus, administration of activated charcoal may be useful in the management of Apixaban overdose or accidental ingestion.
Hypersensitivity to the active substance or to any of the excipients. Clinically significant active bleeding.
Conditions with increased risk of hemorrhage e.g., congenital or acquired bleeding disorders, active ulcerative GI disease, bacterial endocarditis, thrombocytopenia, platelet disorders, history of hemorrhagic stroke, severe uncontrolled HTN, & recent brain, spinal or ophthalmic surgery. Not recommended in patients with hepatic disease associated with coagulopathy & clinically relevant bleeding risk; undergoing hip fracture surgery; prosthetic heart valves with or without atrial fibrillation. Discontinue if severe hemorrhage occurs. Temporarily discontinue for active bleeding, elective surgery, or invasive procedures; avoid lapses in therapy & restart as soon as possible. Risk of developing spinal or epidural hematoma during spinal/epidural anesthesia or puncture which can result in long-term or permanent paralysis. Indwelling epidural or intrathecal catheters must be removed at least 5 hours prior to the 1st dose. Frequently monitor for signs & symptoms of neurological impairment. Not recommended as an alternative to unfractionated heparin for the initial treatment of patients with PE who present with hemodynamic instability or who may receive thrombolysis of pulmonary embolectomy. Not recommended for patients with history of thrombosis who are diagnosed with antiphospholipid syndrome. Carefully assess patients with atrial fibrillation & conditions that warrants mono or dual antiplatelet therapy. Concomitant use with strong CYP3A4 & P-gp inhibitors eg, azole-antimycotics (eg, ketoconazole, itraconazole, voriconazole & posaconazole), HIV PIs (eg, ritonavir); strong CYP3A4 & P-gp inducers (eg, rifampin, phenytoin, carbamazepine, phenobarbital or St. John's wort); antiplatelet agents; NSAIDs including ASA; other platelet aggregation inhibitors or other antithrombotic agents. Not recommended in patients with CrCl <15 mL/min or those undergoing dialysis, or with severe hepatic impairment. Mild or moderate hepatic impairment (Child Pugh A or B). Not recommended during pregnancy. Lactation. Children <18 yr.
Fertility: Studies in animals dosed with apixaban have shown no effect on fertility.
Pregnancy: There are limited data from the use of Apixaban in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity. Apixaban is not recommended during pregnancy.
Lactation: It is unknown whether Apixaban or its metabolites are excreted in human milk. Available data in animals have shown excretion of Apixaban in milk. A risk to newborn and infants cannot be excluded. A decision must be made to either discontinue breast-feeding or to discontinue/abstain from Apixaban therapy.
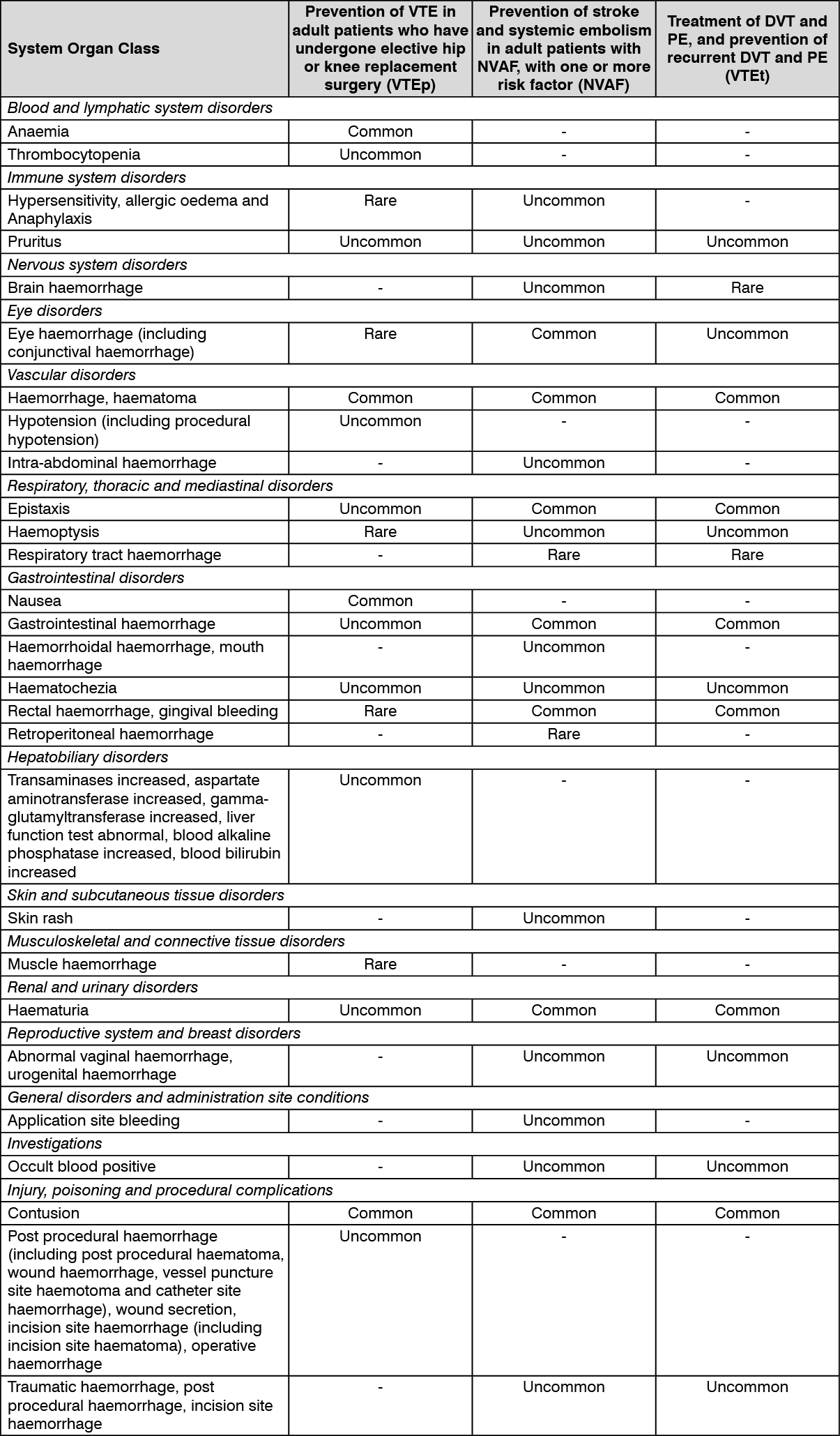
Table as follows shows the adverse reactions ranked under headings of system organ class and frequency using the following convention: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (cannot be estimated from the available data) from VTEp, NVAF, and VTEt respectively. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Increased mean AUC & Cmax with strong CYP3A4 & P-gp inhibitors (eg, ketoconazole). Increased plasma concentration with diltiazem, naproxen, clarithromycin, amiodarone, verapamil, quinidine. Decreased mean AUC & Cmax with strong CYP3A4 & P-gp inducers (eg, rifampin). Reduced plasma concentration with other strong CYP3A4 & P-gp inducers (eg, phenytoin, carbamazepine, phenobarbital or St. John's Wort). Additive effect on anti-FXa activity with enoxaparin. Increased bleeding risk with NSAIDs, ASA or P2Y12 inhibitors. Agents associated with serious bleeding eg, unfractionated heparins & heparin derivatives (including LMWH), FXa inhibiting oligosaccharides (eg, fondaparinux), direct thrombin II inhibitors (eg, desirudin), thrombolytic agents, GPIIb/IIIa receptor antagonists, dipyridamole, dextran, sulfinpyrazone, vit K antagonists, & other oral anticoagulants.
Strong Dual Inhibitors of CYP3A4 and P-gp: For patients receiving apixaban 5 mg or 10 mg twice daily, the dose of apixaban should be decreased by 50% when coadministered with drugs that are strong dual inhibitors of CYP3A4 and P-gp (e.g., ketoconazole, itraconazole, ritonavir, or clarithromycin).
Strong Dual Inducers of CYP3A4 and P-gp: Avoid concomitant use of apixaban with strong dual inducers of CYP3A4 and P-gp (e.g., rifampin, carbamazepine, phenytoin, St. John's wort) because such drugs will decrease exposure to apixaban.
Anticoagulants and Antiplatelet Agents: Coadministration of antiplatelet agents, fibrinolytics, heparin, aspirin, and chronic NSAID use increases the risk of bleeding.
Undesirable effects: The safety of apixaban has been investigated in 7 Phase III clinical studies including more than 21,000 patients: more than 5,000 patients in venous thromboembolic event prevention (VTEp) studies, more than 11,000 patients in non-valvular atrial fibrillation (NVAF) studies and more than 4,000 patients in the venous thromboembolic event treatment (VTEt) studies, for an average total exposure of 20 days, 1.7 years and 221 days respectively.
Special Precautions for Disposal and Other Handling: No special requirement. Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Store at temperatures not exceeding 30°C.
B01AF02 - apixaban ; Belongs to the class of direct factor Xa inhibitors. Used in the treatment of thrombosis.
Xabitor 2.5 FC tab 2.5 mg
30's
Xabitor 5 FC tab 5 mg
30's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out