Sufficient mesna must be given to adequately protect the patient from the urotoxic effects of oxazaphosphorine.
The duration of mesna treatment should equal that of the oxazaphosphorine treatment plus the time taken for the urinary concentration of oxazaphosphorine metabolites to fall to non-toxic levels. This usually occurs within 8-12 hours after the end of oxazaphosphorine treatment but may vary depending on the scheduling of oxazaphosphorine. Urinary output should be maintained at 100 mL/hr (as required for oxazaphosphorine treatment) and the urine monitored for hematuria and proteinuria throughout the treatment period.
Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration.
Any solutions which are discolored, hazy, or contain visible particulate matter should not be used.
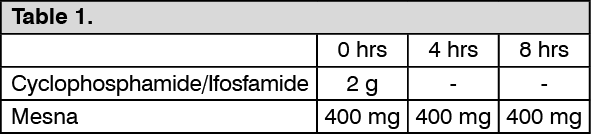
Where ifosfamide or cyclophosphamide is used as an I.V. bolus: Mesna is given by intravenous injection over 15-30 minutes at 20% of the simultaneously administered oxazaphosphorine on a weight per weight basis (w/w). The same dose of mesna is repeated after 4 and 8 hours. The total dose of mesna is 60% (w/w) of the oxazaphosphorine dose. This is repeated on each occasion that the cytotoxic agents are used.
Example of dosage schedule: see Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
If necessary, the dose of mesna can be increased to 40% of the oxazaphosphorine dose given four times at three hourly intervals (0, 3, 6 and 9 hours). (Total dose=160% (w/w) of the oxazaphosphorine dose). This larger dose is recommended in children, in patients whose urothelium may be damaged from previous treatment with oxazaphosphorine or pelvic irradiation, or in patients who are not adequately protected by the standard dose of mesna.
Example of dosage schedule: see Table 2.
Click on icon to see table/diagram/image
Where cyclophosphamide is used orally: The same dose regimen of mesna applies as though cyclophosphamide were used as an I.V. bolus.
Where ifosfamide is used as a 24-hour infusion: Mesna can be used as a concurrent infusion. An initial 20% (w/w) of the total ifosfamide dose is given as an I.V. bolus, then an infusion of 100% (w/w) of the ifosfamide over 24 hours, followed by a further 12-hour infusion of 60% (w/w) of the ifosfamide dose. Total mesna dose=180% of the ifosfamide dose.
Example of dosage schedule: see Table 3.
Click on icon to see table/diagram/image
Where ifosfamide is used as a long-term infusion: An initial 20% (w/w) of the first 24 hours ifosfamide dose is given as an I.V. bolus as the ifosfamide infusion starts. Then each 24-hour infusion of ifosfamide is given with a concurrent 24-hour infusion (100% w/w) of mesna. A 12-hour infusion of mesna (60% (w/w) of the final 24-hour dose of ifosfamide) should be commenced as the ifosfamide-mesna infusion finishes.
Example of dosage schedule: see Table 4.
Click on icon to see table/diagram/image
The final 12-hour infusion of mesna, after long-term or 24-hour infusion of ifosfamide, may be replaced by boluses at 28, 32 and 36 hours, each of 20% (w/w) of the ifosfamide dose, or by oral mesna.
Mesna can be mixed in the same infusion bag as the ifosfamide.
Oral use of mesna ampoules: Mesna has been shown to be effective when taken orally. Compared with intravenous administration, overall availability of mesna in urine after oral administration is approximately 50%; the onset of urinary excretion is delayed by up to 2 hours and is more prolonged than following intravenous dosing.
With the exception of continuous long-term infusions of oxazaphosphorines with mesna, intravenously administered mesna may be replaced by oral administration of mesna. The dosage should be 40% w/w of the dosage of the oxazaphosphorines. The contents of the ampoule should be added to a flavored soft drink (e.g. orange juice, cola). This mixture is stable when refrigerated in a sealed container for 24 hours.
For intermittent oxazaphosphorine therapy following an initial intravenous injection of mesna at a dose of 20% (w/w) of the oxazaphosphorine dose, oral mesna (40% w/w) should be administered at 2 hours and again at 6 hours after the initial intravenous dose. Alternatively, three oral doses of mesna may be administered, replacing the I.V. dose with an oral dose (40% w/w) 2 hours prior to administration of oxazaphosphorines.
Example dosage schedule: see Table 5.
Click on icon to see table/diagram/image
Where ifosfamide is used as a long-term continuous infusion with concomitant mesna, oral mesna may be taken as the infusion of ifosfamide and mesna finishes, then at 2 hours and 6 hours after the time at the finish of the infusion. All oral mesna doses should be 40% (w/w) of the final 24-hour ifosfamide dose.
Example dosage schedule: see Table 6.
Click on icon to see table/diagram/image
Children: Children generally micturate more frequently than adults and therefore it may be necessary to shorten the interval between doses and/or to increase the number of individual doses.
Elderly: No specific information is available.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image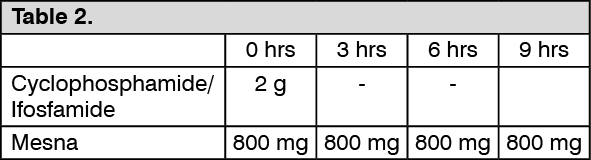 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image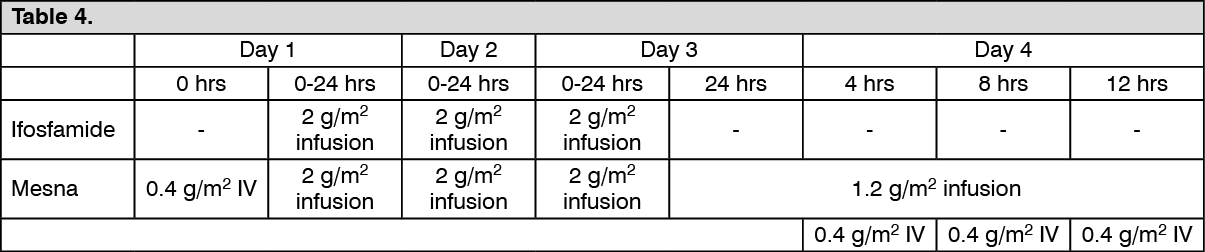 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out