



 Sign Out
Sign Out
Clindamycin appears to inhibit protein synthesis in susceptible organisms by binding to the 50S subunits of the bacterial ribosome which leads to the inhibition of peptide bond formation. This prevents chain prolongation by blocking transpeptidation, halting bacterial multiplication. Clindamycin's site of action appears to be the same as that of erythromycin and chloramphenicol.
Pharmacokinetics: About 90% of an oral clindamycin dose is rapidly absorbed from the gastrointestinal (GI) tract. Prior to absorption, clindamycin hydrochloride is hydrolyzed to free clindamycin in the GI tract. The drug is not inactivated by gastric acidity. Clindamycin's serum concentrations appear to be predictable, increasing linearly with increasing doses. The extent of absorption and peak serum concentrations of clindamycin are not appreciably affected when administered with food, although peak serum concentrations may be delayed.
After oral administration of a single 150 mg dose of clindamycin hydrochloride to healthy, fasting adults, peak serum concentrations of clindamycin average 1.9 to 3.9 mcg/mL and are attained within 45-60 minutes; serum clindamycin concentrations average 1.5 mcg/mL at 3 hours and 0.7 mcg/mL at 6 hours.
Clindamycin is distributed into many body tissues and fluids including saliva, ascites fluid, pleural fluid, synovial fluid, bone, and bile. However, even in the presence of inflamed meninges, only small amounts of the drug diffuse into the cerebrospinal fluid (CSF). The concentration of clindamycin in synovial fluid and bone is reported to be 60-80% of concurrent serum concentrations; the degree of penetration does not appear to be affected by joint inflammation. Clindamycin readily crosses the placenta; cord blood concentrations of the drug have been reported to be 46% of concurrent maternal blood concentrations. Clindamycin is distributed into breast milk.
At a concentration of 1 mcg/mL, about 93% of the drug is bound to serum proteins.
Clindamycin's serum half-life (t1/2) is 2-3 hours in adults and children with normal renal function. The serum t1/2 is increased slightly in patients with markedly reduced renal or hepatic function. Clindamycin's serum concentrations are not appreciably affected by hemodialysis, peritoneal dialysis or prolonged administration in patients with normal renal functions.
Clindamycin is partially metabolized to bioactive and inactive metabolites. The major bioactive metabolites are clindamycin sulfoxide and N-demethyl-clindamycin which are excreted in urine, bile and feces. About 10% of the drug undergoes urinary excretion and about 3.6% via fecal excretion as active drug and metabolites within 24 hours; the remainder is excreted as inactive metabolites. Probenecid has no effect on clindamycin excretion.
Microbiology: Antimicrobial Spectrum of Activity: Clindamycin has demonstrated activity in vitro and in clinical infections against most strains of the following microorganisms: See Table 1.
 Click on icon to see table/diagram/image
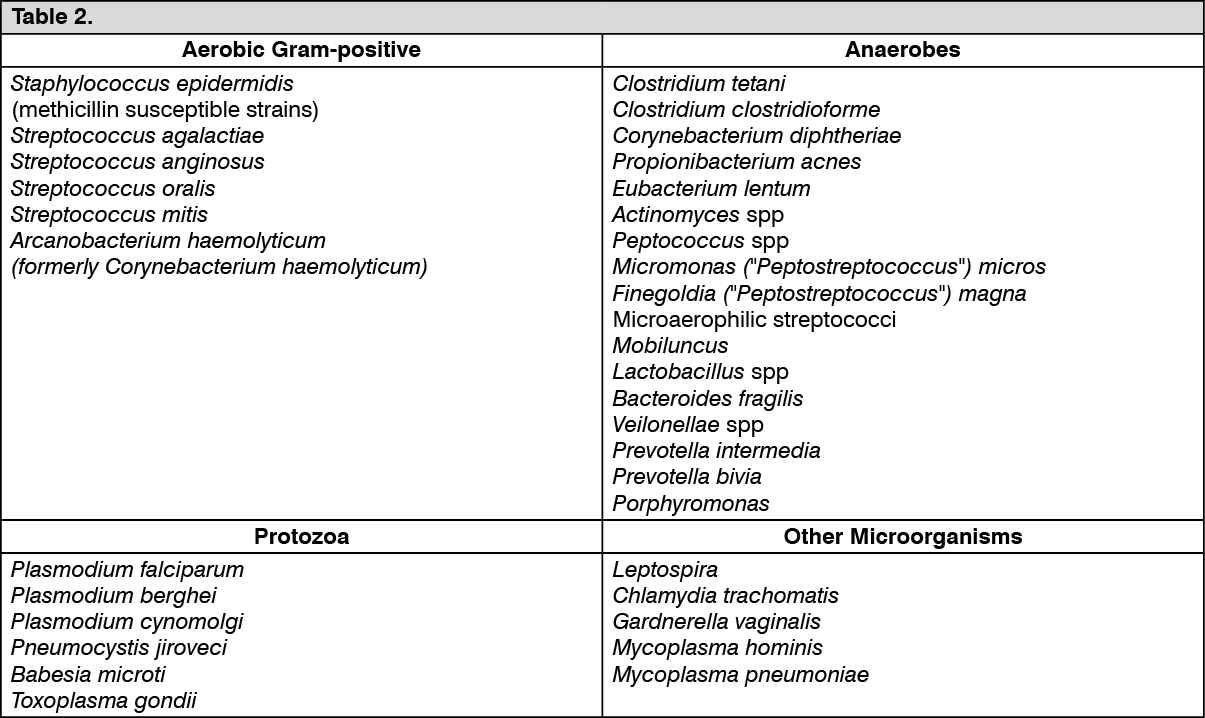
Click on icon to see table/diagram/imageClindamycin has demonstrated in vitro activity against isolates of the following microorganisms; however, clinical significance is unknown: See Table 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageWhen tested by in vitro methods, some staphylococcal strains originally resistant to erythromycin rapidly develop clindamycin resistance.
Cross-resistance has been demonstrated between clindamycin and lincomycin.
It is suggested to carry out susceptibility tests.