



 Sign Out
Sign Out
This product is for intravenous infusion only.
This product is intended for single use only. Any unused medicinal product or waste material should be disposed of in accordance with local requirements.
Dosing Recommendations: Hypercalcemia of Malignancy (HCM) (albumin-corrected serum calcium > 12 mg/dL [3 mmol/L]): 4 mg given as a single dose intravenous (IV) infusion over not less than 15 minutes following standard rehydration procedures.
Hydration: Patients must be maintained in a well hydrated state prior to and following administration of zoledronic acid. Promptly initiate vigorous saline hydration (an integral part of hypercalcemia therapy) and make an attempt to restore the urine output to about 2 L/day throughout treatment. Mild or asymptomatic hypercalcemia may be treated with conservative measures (e.g., saline hydration, with or without loop diuretics). Patients should be hydrated adequately throughout treatment but overhydration should be avoided especially in patients who have cardiac failure. Do not employ diuretic therapy prior to correction of hypovolemia.
Retreatment: If serum calcium does not return to normal or does not remain normal after initial treatment, retreatment with zoledronic acid 4 mg may be considered. It is recommended that a minimum of 7 days elapse before retreatment to allow for full response to the initial dose. Renal function must be carefully monitored in all patients receiving zoledronic acid, and possible deterioration in renal function must be assessed prior to retreatment with zoledronic acid.
In addition, retreatment should be given only to those patients who can tolerate the standard rehydration procedures (i.e., 3 to 5 liters of fluids per day and more than 400 mEq of sodium chloride per day). Serum BUN and creatinine must be evaluated and possible deterioration in renal function must be assessed prior to each re-administration in any patient requiring repeated administration.
Dosage Adjustment in Patients with Renal Impairment: The risks and benefits of treatment with zoledronic acid should be evaluated in patients with HCM who have severe renal impairment. In clinical trials, patients with serum creatinine < 400 micromoL/L or < 4.5 mg/dL were excluded. Although no dose adjustment is necessary in HCM patients with mild to moderate renal impairment, i.e., serum creatinine < 400 micromoL/L or < 4.5 mg/dL, zoledronic acid should not be used in patients with severe renal impairment.
Bone Metastases of Solid Tumors and Osteolytic Lesions of Multiple Myeloma (for patients with creatinine clearance > 60 mL/min): 4 mg given as a single dose IV infusion over not less than 15 minutes every 3 to 4 weeks.
In patients requiring antineoplastic therapy, zoledronic acid should be administered either before or after this treatment. The optimal duration of therapy is not known.
Patients will be required to take oral supplementation of calcium (500 mg) and vitamin D (at least 400 IU) per day. If a patient has a prior history of hypercalcemia or develops hypercalcemia during therapy, the patient is advised to discontinue taking calcium and Vitamin D.
Dosage Adjustment in Patients with Renal Impairment: In patients with mild to moderate renal impairment (defined as creatinine clearance 30 mL/min to 60 mL/min), the dose of zoledronic acid should be reduced (see table as follows). These doses are based on pharmacokinetic data in order to achieve the same AUC as that achieved in patients with creatinine clearance of 75 mL/min. Creatinine clearance (CLcr) is calculated using the Cockcroft-Gault formula as follows: see formula and table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image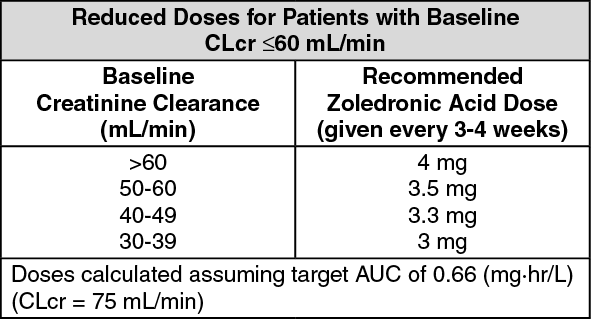 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSerum creatinine should be measured before each zoledronic acid dose and treatment; it should be withheld if renal function has deteriorated. In clinical trials, renal deterioration was defined as follows: For patients with normal baseline serum creatinine (<1.4 mg/dL), an increase of 0.5 mg/dL; For patients with abnormal baseline serum creatinine (>1.4 mg/dL), an increase of 1 mg/dL.