



 Sign Out
Sign Out
Blood glucose monitoring and insulin dose adjustments are recommended to achieve optimal glycemic control. In patients with type 2 diabetes, biphasic insulin aspart 30 can be given as monotherapy. Biphasic insulin aspart 30 can also be given in combination with oral antidiabetic drugs if the patient's blood glucose is inadequately controlled with oral antidiabetic drugs (OADs) alone.
How to Start: Insulin-Naive Patients: For patients with type 2 diabetes, the recommended starting dose of biphasic insulin aspart 30 is 6 U at breakfast and 6 U at dinner (evening meal). However, it can also be initiated once daily with 12 U at dinner (evening meal).
How to Switch: When transferring a patient from biphasic human insulin to biphasic insulin aspart 30, start with the same dose and regimen. Then titrate according to individual needs (see the following titration guideline). As with all insulin products, close glucose monitoring is recommended during the transfer and in the initial weeks thereafter.
How to Intensify: Biphasic insulin aspart 30 can be intensified from once daily to twice daily. When using biphasic insulin aspart 30 once daily, it is generally recommended to move to twice-daily when reaching 30 U by splitting the dose into equal breakfast and dinner doses (50:50).
From biphasic insulin aspart 30 twice daily to thrice daily: The morning dose can be split into morning and lunchtime doses (thrice daily dosing).
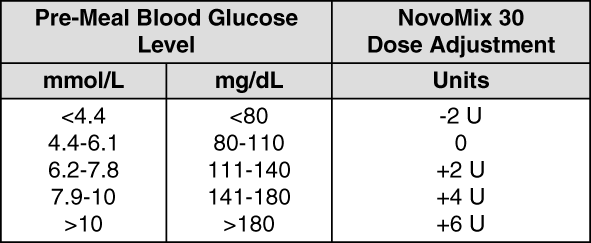
How to Adjust the Dose: Adjust the dose of biphasic insulin aspart 30 on the basis of the lowest pre-meal blood glucose level from the 3 previous days.
Always change the mealtime dose preceding the measurement.
Dose adjustment can be made once a week until target HbA1c is reached.
The dose should not be increased if hypoglycemia occurred within these days.
Adjustment of dosage may be necessary if patients undertake increased physical activity, change their usual diet or during concomitant illness.
The following titration guideline is recommended for dose adjustment (see table).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSpecial Populations: As with all insulin products, in special populations, glucose monitoring should be intensified and the insulin aspart dosage adjusted on an individual basis.
Elderly: Biphasic insulin aspart 30 can be used in elderly patients; however there is limited experience with the use of biphasic insulin aspart 30 in combination with OADs in patients >75 years.
Renal and Hepatic Impairment: Renal or hepatic impairment may reduce the patient's insulin requirements.
Children: Biphasic insulin aspart 30 can be used in children and adolescents ≥10 years when premixed insulin is preferred. Limited clinical data exists for children 6-9 years (see Pharmacology: Pharmacodynamics under Actions). No data are available for biphasic insulin aspart 30 in children below 6 years of age.
Administration: Biphasic insulin aspart 30 is for SC administration only. Biphasic insulin aspart 30 must not be administered IV, as it may result in severe hypoglycemia. Intramuscular administration should be avoided. Biphasic insulin aspart 30 is not to be used in insulin infusion pumps. Biphasic insulin aspart 30 is administered SC by injection in the thigh or in the abdominal wall. If convenient, the gluteal or deltoid region may be used. Injection sites should always be rotated within the same region in order to reduce the risk of lipodystrophy. As with all insulin products, the duration of action will vary according to the dose, injection site, blood flow, temperature and level of physical activity. Biphasic insulin aspart 30 has a faster onset of action than biphasic human insulin and should generally be given immediately before a meal. When necessary, biphasic insulin aspart 30 can be given soon after a meal.