



 Sign Out
Sign Out
 Click on icon to see table/diagram/image
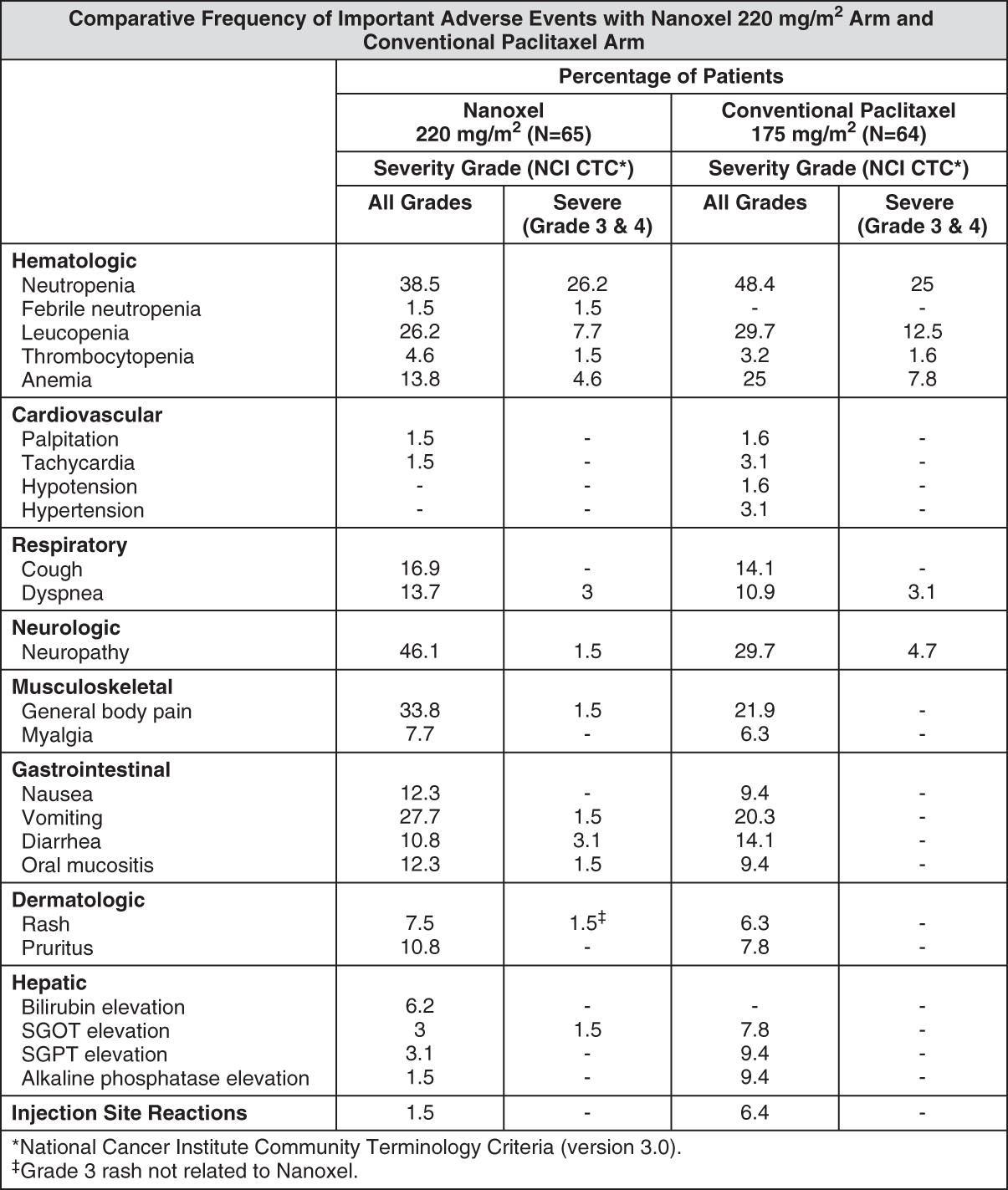
Click on icon to see table/diagram/imageHematologic: Hematological toxicities were modest throughout the duration of therapy. Neutropenia, the most important hematologic toxicity, was dose dependent and reversible. The incidence of neutropenia (all grades) with Nanoxel 220 mg/m2 was 38.5% as compared to conventional paclitaxel (48.4%). Patients receiving Nanoxel 220 mg/m2 had lower incidence of grade 4 neutropenia (12.3%) as compared to conventional paclitaxel (14%). The number of patients requiring G-CSF therapy was found to be comparable ie, 10.9% with conventional paclitaxel and 9.2% with Nanoxel 220 mg/m2. Febrile neutropenia was reported in 1 patient in the Nanoxel 220 mg/m2 arm. The median ANC nadirs were higher in Nanoxel 220 mg/m2 arm as compared to patients treated with conventional paclitaxel (2.2 versus 1.9 cells x 103/mm3).
Grade 3-4 leucopenia was observed in 7.7% of patients treated with Nanoxel (220 mg/m2) as compared to patients treated with conventional paclitaxel (12.5%). The severity of leucopenia was mild (grade 1 & 2) in majority of patients receiving Nanoxel at 220 mg/m2 dose.
Thrombocytopenia was uncommon, which was observed in 4.6% of patients in Nanoxel 220 mg/m2 arm.
Anemia was observed in lesser number of patients in the Nanoxel 220 mg/m2 arm (13.8%) as compared to conventional paclitaxel arm (25%). None of the patient in Nanoxel 220 mg/m2 arm had grade 4 anemia.
Hypersensitivity Reactions (HSRs): In the present study no hypersensitivity reaction was seen in patients who had received Nanoxel despite absence of premedication.
Neurologic: There was no incidence of grade 4 neuropathy in any arm. Sensory neuropathy was the common type of neuropathy observed. In Nanoxel 220 mg/m2 arm, patients who had neuropathy was 46.1%. However, majority of them had grade 1 neuropathy (35.4%). Only 1 patient in this arm suffered from grade 3 neuropathy. In conventional paclitaxel arm, patients who had grade 3 neuropathy was 4.7% compared to 1.5% in the Nanoxel 220 mg/m2 arm.
Musculoskeletal: Myalgia was observed in 7.7% of patients in Nanoxel 220 mg/m2 arm compared to 6.3% in patients receiving conventional paclitaxel. All the events were grade 1/2 in severity, which rsolved without sequelae.
Gastrointestinal: The majority of these GI events were nausea, vomiting, diarrhea and oral mucositis. Nausea/vomiting, diarrhea and mucositis were reported by 40, 10.8 and 12.3% of Nanoxel (220 mg/m2) treated patients. The majority of GI adverse events were of grade 1 & 2 severity and resolved without sequelae.
Dermatologic: The incidence of events related to skin and subcutaneous tissues showed a similar trend in conventional paclitaxel arm and Nanoxel 220 mg/m2 arm (56.4% versus 52.1%, respectively). Most of the events were grade 1-2 in severity.
Hepatic: There was minimal elevation in bilirubin, SGOT and SGPT levels after administration of Nanoxel. All events were of mild to moderate severity. Among patients treated with Nanoxel 220 mg/m2 6.2, 1.5, 3 and 3.1% had elevations in bilirubin, alkaline phosphatase, SGOT and SGPT, respectively.
Accidental Exposure: No reports of accidental exposure to Nanoxel have been received. However, upon inhalation of paclitaxel, dyspnea, chest pain, burning eyes, sore throat and nausea have been reported. Following topical exposure, events have included tingling, burning and redness.
View ADR Reporting Link