The most common adverse reactions associated with etoricoxib are abdominal pain, hypertension, dizziness, headache, ecchymosis, alveolar osteitis, edema, fluid retention, palpitations, arrhythmia, bronchospasm, constipation, flatulence, gastritis, dyspepsia, gastroesophageal reflux disorder, diarrhea, epigastric discomfort, nausea, vomiting, esophagitis, pharyngitis, oral ulcer, asthenia, fatigue, influenza-like illness, and increased ALT and/or AST.
Infections and infestations: Abscess, bacterial infection, bronchitis, cellulitis, fungal infection, herpes simplex, herpes zoster infection, nasopharyngitis, pneumonia, post-operative wound infection, staphylococcal infection, tinea pedis.
Neoplasms benign, malignant and unspecified (including cysts and polyps): Basal cell carcinoma, bladder malignant neoplasm, breast malignant neoplasm, malignant melanoma, non-Hodgkin's lymphoma, uterine leiomyoma.
Blood and lymphatic system disorders: Anemia, leukopenia, thrombocytopenia.
Immune system disorders: Angioedema, anaphylactic/anaphylactoid reaction, anaphylactic/anaphylactoid shock, hypersensitivity, seasonal allergy, urticaria.
Endocrine disorders: Diabetes mellitus.
Metabolism and nutrition disorders: Anorexia, decreased appetite, hyperglycemia, hyperkalemia, increased appetite, peripheral edema, thirst, weight gain.
Psychiatric disorders: Anxiety, confusion, decreased mental acuity, depression, dream abnormality, hallucination, insomnia, somnolence.
Nervous system disorders: Carpal tunnel syndrome, cerebrovascular accident, generalized tonic-clonic seizure, hypoesthesia, hyporeflexia, intracranial hemorrhage, lacunar infarction, lumbar radiculopathy, median nerve neuropathy, memory impairment, paresthesia, restlessness, sciatica, spinal stenosis, syncope, tremor, vertigo.
Eye disorders: Blepharitis, blurred vision, cataract, conjunctivitis, eye pain, Sicca syndrome, visual impairment.
Ear and labyrinth disorders: Ear pain, tinnitus.
Cardiac disorders: Angina pectoris, angina unstable, atrial fibrillation, atrial flutter, cardiac arrest, chest discomfort, chest pain, congestive heart failure, coronary artery disease, dyspnea exertional, mitral valve regurgitation, myocardial infarction, myocardial ischemia, tachycardia.
Vascular disorders: Deep vein thrombosis, diastolic hypertension, flushing, hemorrhoids, hot flush, hypertensive crisis, hypovolemic shock, orthostatic hypotension, transient ischemic attack, vasculitis.
Respiratory, thoracic, and mediastinal disorders: Cough, dyspnea, epistaxis, laryngitis, pulmonary embolism, rales, respiratory failure, sinus congestion, sinusitis, upper respiratory tract infection, wheezing.
Gastrointestinal disorders: Abdominal distention, aphthous ulcer, bowel movement pattern change, dental pain, dry mouth, dysgeusia, esophagitis, frequent bowel movements, gastritis, gastroduodenal ulcers, gastroenteritis, gastrointestinal sounds abnormal, gastrointestinal disorder, gastrointestinal distress, gastrointestinal hemorrhage, gastrointestinal perforation, gingival disorder, glossitis, irritable bowel syndrome, melena, mouth ulceration, oral lesion, oral pain, pancreatitis, peptic ulcer, retching, tongue edema, toothache.
Hepatic and hepatobiliary disorders: Cholelithiasis, cholecystitis, hepatic failure, hepatic steatosis, hepatitis, jaundice.
Skin and subcutaneous tissue disorders: Alopecia, blister, dermal cyst, dermatitis, eczema, erythema, fixed drug eruption, folliculitis, maculopapular rash, non-specific skin disorder, onychomycosis, pruritus, rash, rosacea, skin infection, skin nodule, skin ulcer, Stevens-Johnson syndrome, toxic epidermal necrolysis.
Musculoskeletal and connective tissue disorders: Ankle pain, arthralgia, bursitis, costochondritis, finger pain, foot pain, gout, hip osteoarthritis, hip pain, knee osteoarthritis, muscle spasms, muscular weakness, musculoskeletal pain, musculoskeletal stiffness, neck pain, osteoporosis, periarthritis, rheumatoid arthritis, rotator cuff syndrome, shoulder pain, tendonitis, tenosynovitis, toe deformity.
Renal and urinary disorders: Cystitis, erythrocyturia, glycosuria, hematuria, interstitial nephritis, nephrolithiasis, nephrotic syndrome, nephrotoxicity, nocturia, polyuria, proteinuria, pyelonephritis, renal colic, renal failure, renal insufficiency, urinary calculus, urinary tract infection.
Pregnancy, puerperium and perinatal conditions: Pregnancy.
Reproductive system and breast disorders: Erectile dysfunction, ovarian cyst, vaginal hemorrhage, vaginal infection.
General disorders and administration site conditions: Face edema, feeling hot, fever, hyperhidrosis, pain, prolapse.
Investigations: Decreased bicarbonate, decreased blood sodium, decreased hematocrit, decreased hemoglobin, decreased leukocytes, decreased platelets, fecal occult blood, increased alkaline phosphatase, increased blood pressure, increased blood urea nitrogen, increased creatine phosphokinase, increased erythrocytes, increased gamma-glutamyl transpeptidase, increased monocytes, increased serum creatinine, increased urine nitrite, increased uric acid, non-specific electrocardiogram changes.
Injury, poisoning and procedural complications: Back strain, burn, contusion, corneal abrasion, femoral fracture, hip fracture, humeral fracture, joint sprain, knee sprain, laceration, motor vehicle accident, overdose, strain, subarachnoid hemorrhage, sunburn, tendon rupture, trauma, traumatic arthropathy, wrist fracture.



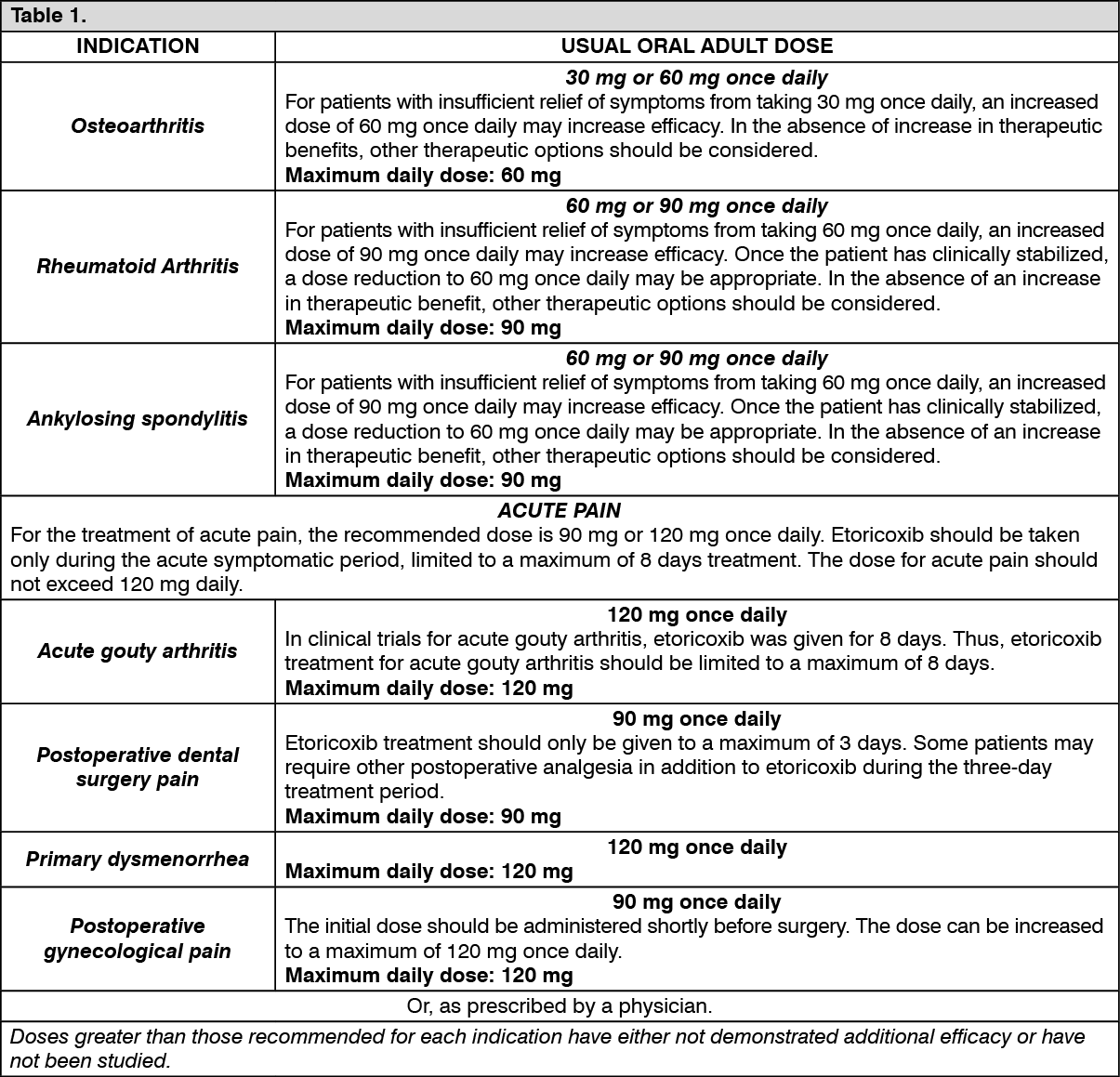 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image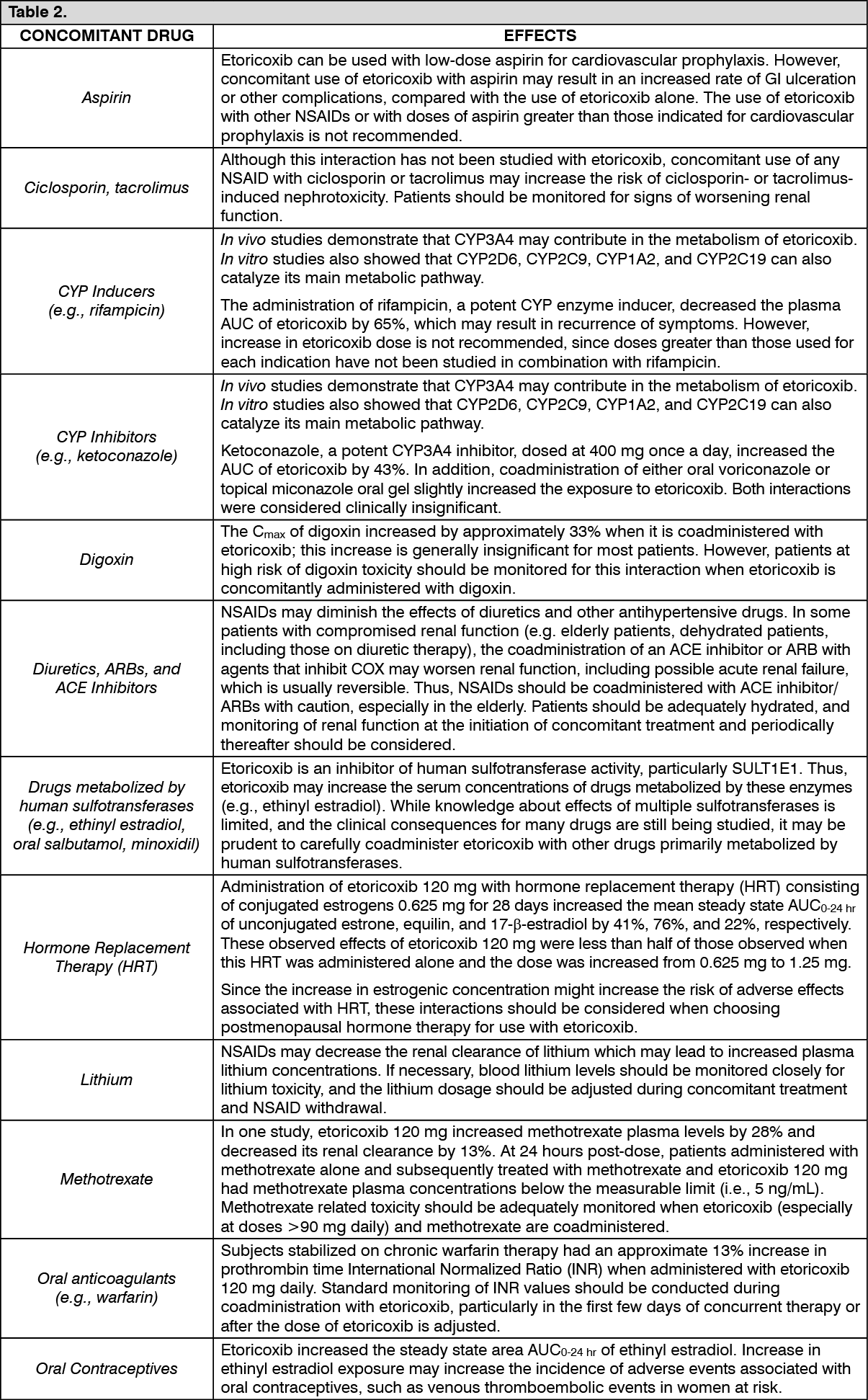 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out