Each vial contains: Ifosfamide 1 g.
Ifosfamide is a chemotherapeutic agent chemically related to the nitrogen mustards and a synthetic analog of cyclophosphamide. Ifosfamide is chemically 3-(2-chloroethyl)-2-[(2-chloroethyl)amino]tetrahydro-2H-1,3,2-oxazaphosphorine2-oxide. The molecular formula is C7H15Cl2N2O2P and its molecular weight is 261.1.
Ifosfamide is a white crystalline powder that is soluble in water; has a melting point of 48-51°C. The pH of a 10% solution of Ifosfamide is between 4.5-7.0. Ifosfamide begins to sinter below the melting point and therefore has to be stored at a controlled temperature, that is as low as possible. It is also advisable to control humidity as Ifosfamide highly hygroscopic. Although Ifosfamide dissolves to an extent of about 10% by weight in water, it only has limited stability in aqueous solution. Ifosfamide for injection is presented as single-dose 1, 2 and 3 gram vials for reconstitution and administration as intravenous infusion only.
Pharmacology: Pharmacodynamics: Mechanism of Action: Ifosfamide has been shown to require metabolic activation by microsomal liver enzymes to produce biologically active metabolites. Activation occurs by hydroxylation at the ring carbon atom 4 to form the unstable intermediate 4-hydroxyifosfamide. This metabolite rapidly degrades to the stable urinary metabolite 4-ketoifosfamide. Opening of the ring results in formation of the stable urinary metabolite 4-carboxyifosfamide. These urinary metabolites have not been found to be cytotoxic. N,N-bis(2-chloroethyl)-phosphoric acid diamide (Ifosphoramide) and acrolein are also found. Enzymatic oxidation of the chloroethyl side chains and subsequent dealkylation produces the major urinary metabolites, dechloroethyl Ifosfamide and dechloroethyl cyclophosphamide. The alkylated metabolites of Ifosfamide have been shown to interact with DNA. In vitro incubation of DNA with activated Ifosfamide has produced phosphotriesters. The treatment of intact cell nuclei may also result in the formation of DNA-DNA cross-links. DNA repair most likely occurs in G1 and G2 stage cells.
Pharmacokinetics: Ifosfamide is well absorbed from the gastrointestinal tract. The pharmacokinetics of ifosfamide are reported to exhibit considerable interindividual variation. It is a prodrug that is extensively metabolised, chiefly by cytochrome P450 isoenzymes such as CYP3A4 and CYP2B6 in the liver, to a variety of active and inactive metabolites; there is some evidence that metabolism is saturated at very high doses. Although the manufacturers state that a mean terminal elimination half-life of about 15 hours has been reported after a single high dose intravenous bolus, most studies at lower doses appear to have recorded elimination half-lives of about 4 to 8 hours. After repeated doses (fractionated therapy) there is a decrease in the elimination half-life, apparently due to autoinduction of metabolism. Ifosfamide is distributed into the CSF. It is excreted largely in urine, as unchanged drug and metabolites.
It is used in the treatment of solid tumours including those of the cervix, lung, ovary, testis, and thymus, as well as in sarcoma and in the treatment of lymphomas.
Ifosfamide is given intravenously, either by injection as a solution diluted to less than 4%, or by infusion. Licensed dosage regimens include a total dose of 8 to 12 g/m2 divided over 3 to 5 days, with the course repeated at 2 to 4 week intervals; a total dose of 6 g/m2 divided over 5 days, repeated every 3 weeks; and doses of 5 to 6 g/m2, to a maximum of 10 g, given as a single 24-hour infusion, repeated at 3 to 4 week intervals. The interval between courses also depends on the blood count.
Ifosfamide should be given with mesna and adequate hydration should be maintained, to avoid urological toxicity; fluid intake should not be less than 2 litres daily.
Or as directed by the physician.
No specific antidote is known. Symptoms of overdose include myelosupression, nausea, vomiting, diarrhea and alopecia which are direct extension of the drugs pharmacological effects. Management of overdosage would include general supportive measures to sustain the patient through any period of toxicity that might occur.
It is contraindicated in known hypersensitivity to administration of Ifosfamide, urinary outflow obstruction.
Should be administered under the supervision of a qualified physician experienced in the use of cancer chemotherapeutic agents. Urotoxic side effects, especially hemorrhagic cystitis, as well as CNS toxicities such as confusion and coma have been associated with the use of Ifosfamide for injection and when these occur, cessation of Ifosfamide therapy may be recommended. Severe myelosuppression has been reported in studies.
It is highly recommended that the doctor keeps a check on the progress of treatment and unwanted effects, during regular visits. While on treatment with Ifosfamide and after cessation of treatment, it is strictly recommended to refrain from any immunizations (vaccinations) without the doctor's approval. Ifosfamide may lower the body's resistance and there is a chance of contracting infection the immunization is meant to prevent. In addition, relatives of the patient living in the same house should not take oral polio vaccine since there is a chance of passing the polio virus; hence avoid persons who have taken oral polio vaccine within the past several months, do not get close to them and stay in the same room for very long. If these precautions cannot be taken, one should consider wearing a protective face mask that covers the nose and mouth.
The treating doctor should be informed immediately for unusual bleeding or bruising, black tarry stools, blood in urine or stools and pinpoint red spots on the skin. Care should be taken while using a regular toothbrush, dental floss, or toothpick.
Ifosfamide should be given cautiously to patients with any of the following conditions like Leukopenia/Thrombocytopenia/Tumour cell infiltration of the bone marrow/Prior radiotherapy/Prior treatment with other antineoplastic agents/Brain metastases and advanced cerebral arteriosclerosis/Impaired renal function/Impaired hepatic function/In the presence of known infections and or Abnormal serum creatinine and serum albumin levels. Because Ifosfamide may exert a suppressive action in immune mechanisms, the interruption or modification of dosage should be considered for patients who develop bacterial, fungal or viral infections. This is especially true for patients receiving concomitant steroid therapy, since infections in some of these patients have been fatal. Ifosfamide may cause significant neurologic, renal and hematologic toxicities which may prove fatal despite careful monitoring prior to and during therapy. Prior to initiating treatment, it is necessary to exclude or correct any obstruction of the efferent urinary tract, cystitis, infections, and electrolyte imbalances. Urinary sediment should be examined at regular intervals. Extra care is required in unilaterally nephrectomised patients, in patients with impaired renal function, and in patients pretreated with nephrotoxic drugs (e.g., cisplatin) who obviously tolerate high doses of Ifosfamide less well. Ifosfamide should not be given until three months after the nephrectomy. Additional caution is also advisable in patients treated concomitantly with drugs having nephrotoxic potential (e.g., aminoglycosides and amphotericin B). Careful monitoring is also required for patients with cerebral metastases, as Ifosfamide has been associated with several CNS symptoms. Leukocyte, erythrocyte and platelet counts should be carried out at regular intervals. There is normally a reduction in the leukocyte count beginning approximately by day 5. The nadir, depending on dosage and baseline count is usually reached after 8-10 days. Recovery occurs after 10-14 days and is usually complete after 2-3 weeks. Neurologic manifestations consisting of somnolence, confusion, hallucinations and, in some instances, coma have been reported following Ifosfamide therapy. In the case of Ifosfamide-induced CNS symptoms, drugs acting on the CNS (e.g., antiemetics and narcotics) should be discontinued, if possible, or used with caution. The occurrence of these symptoms requires discontinuing Ifosfamide therapy. These symptoms have usually been reversible and supporting therapy should be maintained until their resolution.
Ifosfamide should be given cautiously to patients with impaired renal function as well as to those with compromised bone marrow reserve, as indicated by: leukopenia, granulocytopenia, extensive bone marrow metastases, prior radiation therapy, or prior therapy with other cytotoxic agents.
During treatment, the patient's hematologic profile (particularly neutrophils and platelets) should be monitored regularly to determine the degree of hematopoietic suppression. Urine should also be examined regularly for red cells which may precede hemorrhagic cystitis.
Wound healing: Ifosfamide may interfere with normal wound healing.
Carcinogenesis, Mutagenesis, Impairment of fertility: Ifosfamide has been shown to be carcinogenic in rats, with female rats showing a significant incidence of leiomyosarcomas and mammary fibroadenomas. The mutagenic potential of Ifosfamide has been documented in bacterial systems in vitro and mammalian cells in vivo. In vivo, Ifosfamide has induced mutagenic effects in mice and Drosophila melanogaster germ cells, and has induced a significant increase in dominant lethal mutations in male mice as well as recessive sex-linked lethal mutations in Drosophila.
Use in Pregnancy: "Category D".
Use in Lactation: Ifosfamide is excreted in breast milk. Because of the potential for serious adverse events and the tumorigenicity shown for Ifosfamide in animal studies, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Use in Children: Safety and effectiveness in pediatric patients have not been established.
Should be administered under the supervision of a qualified physician experienced in the use of anticancer agents and when adequate diagnostic and treatment facilities are readily available for the appropriate management of complications. Urotoxic side effects especially hemorrhagic cystitis has been frequently associated with the use of Ifosfamide and these effects often result in cessation of therapy. Studies report the therapeutic benefit of mesna as a uroprotective agent where the incidence of urinary tract complications reduced from 40 to 3.5%. Thus it is recommended that Ifosfamide be accompanied by uroprotective agent such as mesna. It is recommended that a urinalysis should be obtained prior to each dose of. If microscopic hematuria (greater than 10 RBCs per high power field) is present then subsequent administration should be withheld until complete resolution. Further administration of should be given with vigorous oral or parenteral hydration.
Hematopoietic system: when Ifosfamide is given in combination with other chemotherapeutic agents, severe myelosuppression can be expected and close hematologic monitoring is recommended. White blood cell (WBC) count, platelet count and hemoglobin should be obtained prior to each administration and at appropriate intervals. Unless clinically essential Ifosfamide should not be given to patients with WBC count below 2000/µL and/or platelet count below 50,000/µL.
Central Nervous System: neurologic manifestations such as somnolence, confusion, hallucinations and in some instances coma, have been reported following Ifosfamide therapy. The occurrence of these symptoms requires discontinuation of therapy. The symptoms are usually reversible and supportive therapy should be maintained until complete resolution.
Before using Ifosfamide, the risks of taking the medicine must be weighed against the good it will do. This decision has to be mutually agreed by both the patient and the doctor. For Ifosfamide, the following should be considered: Allergies: inform the doctor of any unusual or allergic reaction to Ifosfamide.
Use in Children: Although there is no specific information comparing use of Ifosfamide in children with use in other age groups, Ifosfamide is not expected to cause different side effects or problems in children than it does in adults.
Use in Elderly: Many medicines have not been studied specifically in older people. Therefore, it may not be known whether they work exactly the same way they do in younger adults or if they cause different side effects or problems in older people. There is no specific information comparing use of Ifosfamide in the elderly with use in other age groups.
Other medicines: Although certain medicines should not be used together at all, in certain unavoidable cases two different medicines may be used together even if an interaction might occur between the two. In such cases, the doctor may want to change the dose, or other precautions may be necessary. When on Ifosfamide therapy, it is especially important that the health care professional knows the concomitant use of Amphotericin B injection/Antithyroid agents (medicine for overactive thyroid)/Azathioprine/Chloramphenicol/Colchicine/Flucytosine/Ganciclovir/Interferon/Plicamycin/Zidovudine and or treatment with x-rays or other cancer medicines as Ifosfamide may increase the effects of these medicines or radiation therapy.
Other medical problems: The presence of other medical problems may affect the use of Ifosfamide. These include Chickenpox (including recent exposure)/Herpes zoster (shingles) which potentiates the risk of disease affecting other parts of the body/Infection as Ifosfamide may decrease the body's ability to fight infection/Kidney disease which may cause effects to be increased because of slower removal of Ifosfamide from the body/Liver disease where the effects may be increased or decreased because the liver works by for the action and removal of Ifosfamide from the body.
Patients receiving Ifosfamide therapy are advise to drink extra fluids to pass more urine and empty bladder frequently, including at least once during the night to prevent kidney and bladder problems. Ifosfamide passes out from the body through the urine. If too much of it appears in the urine or if the urine stays in the bladder too long, it can cause dangerous irritation. Some patients may have to drink up to 7 to 12 cups (3 quarts) of fluid a day.
Ifosfamide may also often cause nausea and vomiting. However, it is very important that patients continue to receive the medicine and ask the health care professional for ways to lessen these effects.
Since the possibility of interference with normal wound healing has been reported with other oxazaphosphorines, Ifosfamide therapy should not be initiated for at least 10-14 days after surgery.
Ifosfamide, like other alkylating agents, has been reported to have oncogenic activity in animals. Thus the possibility that it may have oncogenic potential in humans should be considered.
Use in Pregnancy: Ifosfamide for injection can be teratogenic and cause fetal resorption in experimental animals. It should not be used in pregnancy, particularly in early pregnancy, unless in the judgement of the physician the potential benefits outweigh the possible risks. As is the case with the oxazaphosphorine class of alkylating agents, Ifosfamide is excreted in breast milk and breastfeeding should be terminated prior to institution of Ifosfamide therapy. Inform the doctor if the patient is pregnant or if the patient intend to have children. There is a chance that this medicine may cause birth defects if either the male or female is taking it at the time of conception or if it is taken during pregnancy. Animal studies indicate that the drug is capable of causing gene mutations and chromosomal damage in vivo. Embryotoxic and teratogenic effects have been observed in mice, rats and rabbits at doses 0.05-0.075 times the human dose. In addition, many cancer medicines may cause sterility that could be permanent. Although sterility has not been reported with this medicine, the possibility should be kept in mind. Be sure that the patient have discussed this with the doctor before taking this medicine. It is best to use some kind of birth control while receiving Ifosfamide. The patient should tell doctor right away on becoming pregnant while receiving Ifosfamide.
Pregnancy: "Category D".
Ifosfamide for injection can be teratogenic and cause fetal resorption in experimental animals. It should not be used in pregnancy, particularly in early pregnancy, unless in the judgement of the physician the potential benefits outweigh the possible risks. As is the case with the oxazaphosphorine class of alkylating agents, Ifosfamide is excreted in breast milk and breastfeeding should be terminated prior to institution of Ifosfamide therapy. Inform the doctor if the patient is pregnant or if the patient intend to have children. There is a chance that this medicine may cause birth defects if either the male or female is taking it at the time of conception or if it is taken during pregnancy. Animal studies indicate that the drug is capable of causing gene mutations and chromosomal damage in vivo. Embryotoxic and teratogenic effects have been observed in mice, rats and rabbits at doses 0.05-0.075 times the human dose. In addition, many cancer medicines may cause sterility that could be permanent. Although sterility has not been reported with this medicine, the possibility should be kept in mind. Be sure that the patient have discussed this with the doctor before taking this medicine. It is best to use some kind of birth control while receiving Ifosfamide. The patient should tell doctor right away on becoming pregnant while receiving Ifosfamide.
Lactation: Ifosfamide is excreted in breast milk. Because of the potential for serious adverse events and the tumorigenicity shown for Ifosfamide in animal studies, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Adverse effects involves confusion, drowsiness, depressive psychosis, hallucinations, and rarely, seizures.
Effects on the heart: Severe myocardial depression, with heart failure and ventricular arrhythmias, has been reported in patients given high-dose ifosfamide. Symptoms were reversible with appropriate treatment in most cases.
Effects on the kidneys: In addition to its effects on the bladder ifosfamide may be associated with serious nephrotoxicity. Both proximal and distal tubular damage and to a lesser extent glomerular effects are seen.
Effects on the nervous system: Use of ifosfamide (with mesna for urothelial protection) may be associated with the development of severe encephalopathy, with EEG abnormalities, disorientation, hallucinations, catatonia, and coma; occasionally CNS depression has led to circulatory collapse and death.
Ifosfamide is a substrate for both CYP3A4 and CYP2B6.
Inducers of CYP3A4: CYP3A4 inducers (e.g., carbamazepine, phenytoin, fosphenytoin, phenobarbital, rifampin, St. John's Wort) may increase the metabolism of ifosfamide to its active alkylating metabolites. CYP3A4 inducers may increase the formation of the neurotoxic/nephrotoxic ifosfamide metabolite, chloroacetaldehyde. Closely monitor patients taking ifosfamide with CYP3A4 inducers for toxicities and consider dose adjustment.
Inhibitors of CYP3A4: CYP3A4 inhibitors (e.g., ketoconazole, fluconazole, itraconazole, sorafenib, aprepitant, fosaprepitant, grapefruit, grapefruit juice) may decrease the metabolism of ifosfamide to its active alkylating metabolites, perhaps decreasing the effectiveness of ifosfamide treatment.
Handling and Disposal: Preparation of Ifosfamide for Injection, USP should be done in a vertical laminar flow hood (Biological Safety Cabinet-Class II). Personnel preparing Ifosfamide should wear PVC gloves, safety glasses, disposable gowns and masks. All needles, syringes, vials and other materials which have come in contact with Ifosfamide should be segregated and incinerated at 1000°C or more. Proper precautions should be taken in packaging these materials for transport. Personnel regularly involved in the preparation and handling of Ifosfamide should have bi-annual blood examinations. Procedures for proper handling and disposal of anticancer drugs should be considered. Skin reactions associated with accidental exposure to may occur. If solution contacts the skin or mucosa, immediately wash the skin thoroughly with soap and water or rinse the mucosa with copious amounts of water. Several guidelines on this subject have been published; however there is no general agreement that all of the procedures recommended in the guidelines are necessary or appropriate.
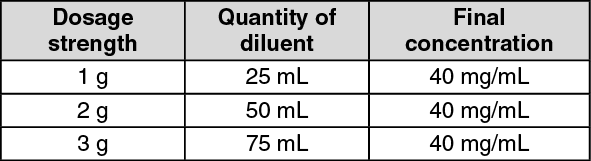
Direction for Reconstitution: Injections are prepared for parenteral use by adding Sterile Water for Injection USP or Sterile Bacteriostatic Water for Injection USP (benzyl alcohol or paraben preservative) to the vial and shaking to dissolve. If dissolution does not take place immediately, allow to stand for few minutes and shake again. It is advisable to use the preparation
immediately after reconstitution. Use the quantity of diluent shown as follows to constitute the product: (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Solutions of Ifosfamide may be diluted further to achieve concentrations of 0.6 to 20 mg/mL in either 5% Dextrose Injection USP, 0.9% Sodium Chloride Injection USP, Lactated Ringer's Injection USP and Sterile Water for Injection USP. For intravenous infusions lasting approximately 30 minutes, dilution with 250 mL Ringer's solution or 5% dextrose solution or 0.9% sodium chloride solution is appropriate; however for intravenous infusions lasting from 1-2 hours, dilution with 500 mL Ringer's solution or 5% dextrose solution or 0.9% sodium chloride solution has been found to be appropriate. The use of large volume parenteral glass bottles for infusion is also acceptable. Reconstituted or constituted and further diluted solutions of should be refrigerated and used within 24 hours. Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration. "Single dose. Discard any remaining portion."
Store at temperatures not exceeding 25°C. Protect from light. Do not freeze.
Reconstituted solutions should be used within 24 hours if stored at room temperature, or within 72 hours if refrigerated. Use further diluted solutions immediately.
Note: As with all parenteral drug products, intravenous admixtures should be inspected visually for clarity, particulate matter, precipitate, discolouration and leakage prior to administration, whenever solution and container permit. Solution showing haziness, particulate matter, precipitate, discolouration or leakage should not be used. Discard unused portion.
L01AA06 - ifosfamide ; Belongs to the class of alkylating agents, nitrogen mustard analogues. Used in the treatment of cancer.
Fosfa powd for inj 1 g
1's
Fosfa powd for inj 2 g
1's





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out