Generic name: Domperidone (as maleate).
Pharmacologic classification: Gastrokinetic (Prokinetic): Domperidone is a dopamine receptor antagonist used as a peristaltic stimulant and anti-emetic agent for dyspepsia, indigestion, epigastric pain, nausea, and vomiting.
Pharmacology: Pharmacodynamics: Domperidone is a dopamine receptor (D2) antagonist.
Domperidone is a selective peripheral dopamine antagonist at the D2 dopamine receptor in the Chemo-receptor Trigger Zone (CTZ) and stomach. Domperidone does not readily enter the central nervous system (the chemoreceptor trigger zone is considered to lie outside the blood-brain barrier). Domperidone increases spontaneous gastric activity and antagonizes dopamine inhibition of gastric emptying. Domperidone has been shown to increase lower esophageal sphincter pressure and promotes esophageal and antral peristalsis and also increases pyloric dilatation. Domperidone increases the frequency, amplitude, and duration of duodenal contraction and reduces the small bowel transit time. Domperidone has no acetylcholine-like effect.
Pharmacokinetics: Absorption: In fasting subjects, domperidone is rapidly absorbed after oral administration, with peak plasma concentration at 30 to 60 minutes. The low absolute bioavailability of oral domperidone (approximately 15%) is due to extensive first-pass metabolism in the gut wall and liver. Although domperidone's bioavailability is enhanced in normal subjects when taken after a meal, patients with gastro-intestinal complaints should take domperidone 15-30 minutes before a meal. Reduced gastric acidity impairs the absorption of domperidone. Oral bioavailability is decreased prior concomitant administration of cimetidine and sodium bicarbonate. The time of peak absorption is slightly delayed and the AUC somewhat increased when the oral drug is taken after a meal.
Distribution: Oral domperidone does not appear to accumulate or induce on its own metabolism; a peak plasma level after 90 minutes of 21 ng/mL after two weeks of oral administration of 30 mg per day was almost the same as that of 18 ng/mL after the first dose. Domperidone is 91-93% bound to plasma proteins. Distribution studies with radiolabelled drug in animals have shown wide tissue distribution, but low brain concentration. Small amounts of drug cross the placenta in rats.
Metabolism: Domperidone undergoes rapid and extensive hepatic metabolism by hydroxylation and N-dealkylation. In vitro metabolism experiments with diagnostic inhibitors revealed that CYP3A4 is a major form of cytochrome P-450 involved in the N-dealkylation of domperidone, whereas CYP3A4, CYP1A2 and CYP2E1 are involved in domperidone aromatic hydroxylation.
Excretion: Urinary and fecal excretions amount to 31 and 66% of the oral dose respectively. The proportion of the drug excreted unchanged is small (10% of fecal excretion and approximately 1% of urinary excretion). The plasma half-life after a single oral dose is 7-9 hours in healthy subjects but is prolonged in patients with severe renal insufficiency.
Prevention and symptomatic relief of acute nausea and vomiting in adults from any cause but specially: Cytotoxic therapy; Radiotherapy; Nausea and vomiting associated with L-dopa and bromocriptine treatment for parkinsonian patients; Nausea associated with migraine attacks.
Stimulation of gut mobility: Non-ulcer dyspepsia; Esophageal reflux; Reflux esophagitis; Gastritis; Speeding barium transit in "follow-through" radiological studies; Diabetic gastroparesis.
Functional Dyspepsia.
Domperidone should be used at the lowest effective dose for the shortest duration necessary to control nausea and vomiting.
It is recommended to take oral domperidone tablets 15-30 minutes before meals. If taken after meals, absorption of the drug is somewhat delayed.
Patients should try to take each dose at the scheduled time. If a scheduled dose is missed, the missed dose should be omitted and the usual dosing schedule resumed. The dose should not be doubled to make up for a missed dose.
Usually, the maximum treatment duration should not exceed one week.
Adults and adolescents (12 years of age and older and weighing 35 kg or more): One 10 mg tablet up to three times per day with a maximum dose of 30 mg per day.
Domperidone is contraindicated to patients having known hypersensitivity to this drug and in case of neonates. Domperidone should not be used when gastrointestinal stimulation might be dangerous i.e. gastrointestinal haemorrhage, obstruction, perforation or immediately after surgery.
Renal Impairment: The elimination half-life of domperidone is prolonged in severe renal impairment (serum creatinine >6 mg/100 mL, i.e. 0.6 mmol/L). The dosing frequency of domperidone should be reduced to once or twice daily depending on the severity of the impairment. The dose may also need to be reduced.
Cardiovascular effects: Domperidone has been associated with prolongation of the QT interval on the electrocardiogram. During post-marketing surveillance, there have been very rare cases of QT prolongation and torsades de pointes in patients taking domperidone. These reports included patients with confounding risk factors, electrolyte abnormalities and concomitant treatment which may have been contributing factors.
Epidemiological studies showed that domperidone was associated with an increased risk of serious ventricular arrhythmias or sudden cardiac death. A higher risk was observed in patients older than 60 years, patients taking daily doses greater than 30 mg, and patients concurrently taking QT-prolonging drugs or CYP3A4 inhibitors.
Domperidone should be used at the lowest effective dose in adults and adolescents 12 years of age and older.
Domperidone is contraindicated in patients with known existing prolongation of cardiac conduction intervals, particularly QTc, in patients with significant electrolyte disturbances (hypokalaemia, hyperkalaemia, hypomagnesaemia), or bradycardia, or in patients with underlying cardiac diseases such as congestive heart failure due to increased risk of ventricular arrhythmia. Electrolyte disturbances (hypokalaemia, hyperkalaemia, hypomagnesaemia) or bradycardia are known to be conditions increasing the proarrhythmic risk.
Treatment with domperidone should be stopped if signs or symptoms occur that may be associated with cardiac arrhythmia, and the patients should consult their physician.
Patients should be advised to promptly report any cardiac symptoms.
Use with Apomorphine: Domperidone is contra-indicated with QT prolonging drugs including apomorphine, unless the benefit of the co-administration with apomorphine outweighs the risks, and only if the recommended precautions for co-administration mentioned in the apomorphine SmPC are strictly fulfilled. Please refer to the apomorphine SmPC.
Co-administration of levodopa: Although no dosage adjustment of levodopa is deemed necessary, an increase of plasma levodopa concentration (max 30-40%) has been observed when domperidone was taken concomitantly with levodopa.
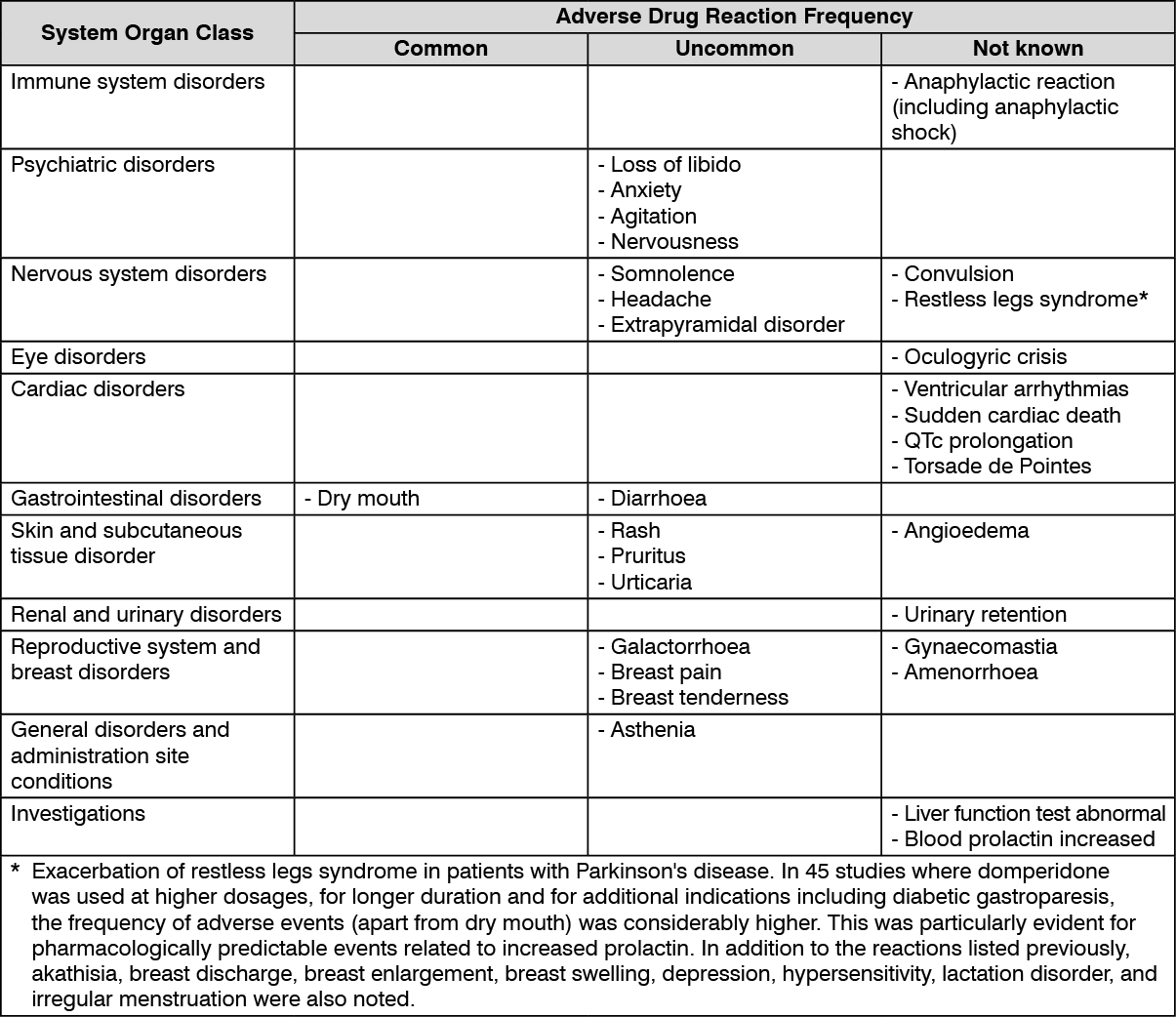
The safety of domperidone was evaluated in clinical trials and in postmarketing experience. The clinical trials included 1275 patients with dyspepsia, gastro-oesophageal reflux disorder (GORD), Irritable Bowel Syndrome (IBS), nausea and vomiting or other related conditions in 31 double-blind, placebo-controlled studies. All patients were at least 15 years old and received at least one dose of domperidone (domperidone base). The median total daily dose was 30 mg (range 10 to 80 mg), and median duration of exposure was 28 days (range 1 to 28 days). Studies in diabetic gastroparesis or symptoms secondary to chemotherapy or parkinsonism were excluded.
The following terms and frequencies are applied: Very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). Where frequency cannot be estimated from clinical trials data, it is recorded as "Not known". (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The main metabolic pathway of domperidone is through CYP3A4. In vitro and human data suggest that the concomitant use of drugs that significantly inhibit this enzyme may result in increased plasma levels of domperidone.
Increased risk of occurrence of QT-interval prolongation, due to pharmacodynamic and/or pharmacokinetic interactions.
Concomitant use of the following substances is contraindicated: QTc-prolonging medicinal products; anti-arrhythmics class IA (e.g., disopyramide, hydroquinidine, quinidine); anti-arrhythmics class III (e.g., amiodarone, dofetilide, dronedarone, ibutilide, sotalol); certain anti-psychotics (e.g., haloperidol, pimozide, sertindole); certain anti-depressants (e.g., citalopram, escitalopram); certain antibiotics (e.g. , erythromycin, levofloxacin, moxifloxacin, spiramycin); certain antifungal agents (e.g., pentamidine); certain antimalarial agents (in particular halofantrine, lumefantrine); certain gastro-intestinal medicines (e.g., cisapride, dolasetron, prucalopride); certain antihistaminics (e.g., mequitazine, mizolastine); certain medicines used in cancer (e.g., toremifene, vandetanib, vincamine); certain other medicines (e.g., bepridil, diphemanil, methadone); apomorphine, unless the benefit of the co-administration outweighs the risks, and only if the recommended precautions for co-administration are strictly fulfilled. Please refer to the apomorphine SmPC.
Potent CYP3A4 inhibitors (regardless of their QT prolonging effects), i.e: Protease inhibitors, systemic azole antifungals; some macrolides (erythromycin, clarithromycin, telithromycin).
Concomitant use of the following substances is not recommended: Moderate CYP3A4 inhibitors i.e. diltiazem, verapamil and some macrolides.
Concomitant use of the following substances requires caution in use: Caution with bradycardia and hypokalaemia-inducing drugs, as well as with the following macrolides involved in QT-interval prolongation: azithromycin and roxithromycin (clarithromycin is contraindicated as it is a potent CYP3A4 inhibitor).
The previously mentioned list of substances is representative and not exhaustive.
Separate in vivo pharmacokinetic/pharmacodynamic interaction studies with oral ketoconazole or oral erythromycin in healthy subjects confirmed a marked inhibition of domperidone's CYP3A4 mediated first pass metabolism by these drugs.
With the combination of oral domperidone 10 mg four times daily and ketoconazole 200 mg twice daily, a mean QTc prolongation of 9.8 msec was seen over the observation period, with changes at individual time points ranging from 1.2 to 17.5 msec. With the combination of domperidone 10 mg four times daily and oral erythromycin 500 mg three times daily, mean QTc over the observation period was prolonged by 9.9 msec, with changes at individual time points ranging from 1.6 to 14.3 msec. Both the Cmax and AUC of domperidone at steady state were increased approximately three-fold in each of these interaction studies. In these studies domperidone monotherapy at 10 mg given orally four times daily resulted in increases in mean QTc of 1.6 msec (ketoconazole study) and 2.5 msec (erythromycin study), while ketoconazole monotherapy (200 mg twice daily) led to increases in QTc of 3.8 and 4.9 msec, respectively, over the observation period.
Levodopa: Increase of plasma levels of levodopa (max 30-40%).
Dilution and compatibility: Not applicable.
Store at temperatures not exceeding 30°C.
A03FA03 - domperidone ; Belongs to the class of propulsives. Used in the treatment of functional gastrointestinal disorders.
Dometab FC tab 10 mg
100's (P11.75/film-coated tab)



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out