



 Sign Out
Sign Out

Early clinical studies of oral anticoagulants, which formed the basis for recommended therapeutic ranges of 1.5-2.5 times control PT, used sensitive human brain thromboplastin. When using the less sensitive rabbit brain thromboplastins commonly employed in PT assays today, adjustments must be made to the targeted PT range that reflect this decrease in sensitivity.
Available clinical evidence indicates that an INR of 2-3 (eg, PT ratio of 1.2-1.5) when measuring with the less sensitive thromboplastin reagents, ISI=2.8 (see table) is sufficient for prophylaxis and treatment of venous thromboembolism and minimizes the risk of hemorrhage associated with higher INRs. Five (5) recent clinical trials evaluated the effects of warfarin in patients with non-valvular atrial fibrillation (AF). Meta-analysis findings of these studies revealed that the effects of warfarin in reducing thromboembolic events including stroke were similar at either moderately high INR (2-4.5) or low INR (1.4-3). There was a significant reduction in minor bleeds at the low INR. Similar data from clinical studies in valvular atrial fibrillation patients are not available. The trials in non-valvular atrial fibrillation support the American College of Chest Physicians (ACCP) recommendation that an INR of 2-3 be used for long-term warfarin therapy in appropriate AF patients. In cases where the risk of thromboembolism is great eg, in patients with recurrent systemic embolism, a higher INR may be required. A PT ratio of >2 appears to provide no additional therapeutic benefit in most patients and is associated with a higher risk of bleeding.
In patients with mechanical heart valve(s), long-term prophylaxis with warfarin to an INR of 2.5-3.5 is recommended. In patients with bioprosthetic heart valve(s), based on limited data, the American College of Chest Physicians recommends warfarin therapy to an INR of 2-3 for 12 weeks after valve insertion. In patients with additional risk factors eg, atrial fibrillation or prior thromboembolism, consideration should be given for longer term therapy.
The proceedings and recommendations of the 1986 National Conference on Antithrombotic Therapy review and evaluate issues related to oral anticoagulant therapy and the sensitivity of thromboplastin reagents and provide additional guidelines for defining the appropriate therapeutic regimen.
The conversion of the INR to PT ratios for the less-intense (INR 2-3) and more intense (INR 2.5-3.5) therapeutic range recommended by the ACCP for thromboplastins over a range of ISI values is shown in the table. (See table.)
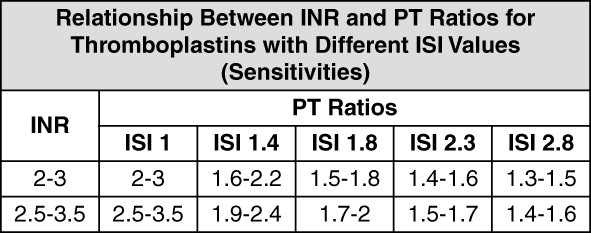 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageInitial Dosage: The dosing of Coumadin must be individualized according to patient's sensitivity to the drug as indicated by the INR and/or PT ratio.
Use of a large loading dose may increase the incidence of hemorrhage and other complications, does not offer more rapid protection against thrombi formation, and is not recommended. Low initiation doses are recommended for elderly and/or debilitated patients and patients with increased sensitivity to Coumadin (see Precautions).
It is recommended that Coumadin therapy be initiated with a dose of 2-5 mg/day with dosage adjustments based on the results of INR and/or PT ratio determinations.
Maintenance: Most patients are satisfactorily maintained at a dose of 2-10 mg daily. Flexibility of dosage is provided by breaking scored-tablets in half. The individual dose and interval should be gauged by the patient's prothrombin response.
Duration of Therapy: The duration of therapy in each patient should be individualized. In general, anticoagulant therapy should be continued until the danger of thrombosis and embolism has passed.
Laboratory Control: The PT reflects the depression of vitamin K-dependent Factors VII, IX, X and II. There are several modifications of the 1-stage PT and the physician should become familiar with the specific method used in his laboratory. The degree of anticoagulation indicated by any range of PTs may be altered by the type of thromboplastin used; the appropriate therapeutic range must be based on the experience of each laboratory. The PT should be determined daily after the administration of the initial dose until PT results stabilize in the therapeutic range. Intervals between subsequent PT determinations should be based upon the physicians' judgment of the patient's reliability and response to Coumadin in order to maintain the individual within the therapeutic range. Acceptable intervals for PT determinations are normally within the range of 1-4 weeks after a stable dosage has been determined. To ensure adequate control, it is recommended that additional PT tests are done when other warfarin products are interchanged with Coumadin and also if other medications are co-administered with it (see Precautions).
Treatment During Dentistry and Surgery: The management of patients who undergo dental and surgical procedures requires close liaison between attending physicians, surgeons and dentists. In patients who must be anticoagulated prior to, during or immediately following dental or surgical procedures, adjusting the dosage of Coumadin to maintain the PT at the low end of the therapeutic range, may safely allow for continued anticoagulation. The operative site should be sufficiently limited and accessible to permit the effective use of local procedures for hemostasis. Under these conditions, dental and surgical procedures may be performed without undue risk of hemorrhage.
Conversion from Heparin Therapy: Since the onset of the Coumadin effect is delayed, heparin is preferred initially for rapid anticoagulation. Conversion to Coumadin may begin concomitantly with heparin therapy or may be delayed 3-6 days. As heparin may affect the PT, patients receiving both heparin and Coumadin should have blood for PT determination, drawn at least: 5 hrs after the last IV bolus dose of heparin; or 4 hrs after cessation of a continuous IV infusion of heparin; or 24 hrs after the last SC heparin injection.
When Coumadin has produced the desired therapeutic range or prothrombin activity, heparin may be discontinued.