Colorless to pale yellow transparent solution contained in a clear colorless flexible plastic bag.
Each 1 mL contains: Ciprofloxacin 2 mg, 2-hydroxyglutaric acid-γ-lactone 0.864 mg, Sodium chloride 9 mg, Hydrochloric acid q.s., Water for injection q.s.
Pharmacotherapeutic group: Fluoroquinolones.
Pharmacology: Pharmacodynamics: Mechanism of action: As a fluoroquinolone antibacterial agent, the bactericidal action of ciprofloxacin results from the inhibition of both type II topoisomerase (DNA-gyrase) and topoisomerase IV, required for bacterial DNA replication, transcription, repair and recombination.
Pharmacokinetic/pharmacodynamic relationship: Efficacy mainly depends on the relation between the maximum concentration in serum (C
max) and the minimum inhibitory concentration (MIC) of ciprofloxacin for a bacterial pathogen and the relation between the area under the curve (AUC) and the MIC.
Mechanism of resistance: In-vitro resistance to ciprofloxacin can be acquired through a stepwise process by target site mutations in both DNA gyrase and topoisomerase IV. The degree of cross-resistance between ciprofloxacin and other fluoroquinolones that results is variable.
Single mutations may not result in clinical resistance, but multiple mutations generally result in clinical resistance to many or all active substances within the class.
Impermeability and/or active substance efflux pump mechanisms of resistance may have a variable effect on susceptibility to fluoroquinolones, which depends on the physiochemical properties of the various active substances within the class and the affinity of transport systems for each active substance. All in-vitro mechanism of resistance are commonly observed in clinical isolates. Resistance mechanism that inactivate other antibiotics such as permeation barriers (common in
Pseudomonas aeruginosa) and efflux mechanisms may affect susceptibility to ciprofloxacin.
Plasmid-mediated resistance encoded by qnr-genes has been reported.
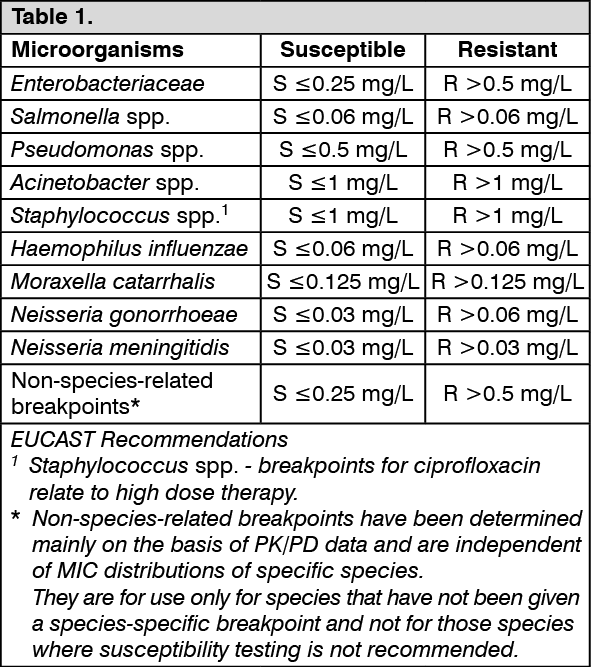
Spectrum of antibacterial activity: Breakpoints separate susceptible strain from strains with intermediate susceptibility and the latter from resistant strains: See table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent in at least some types of infections is questionable.
Groupings of relevant species according to ciprofloxacin susceptibility: See table 2.
Click on icon to see table/diagram/image
Pharmacokinetics: Absorption: Following an intravenous infusion of ciprofloxacin, the mean maximum serum concentrations were achieved at the end of infusion. Pharmacokinetics of ciprofloxacin were linear over the dose range up to 400 mg administered intravenously.
Comparison of the pharmacokinetic parameters for a twice a day and three times a day intravenous dose regimen indicated no evidence of drug accumulation for ciprofloxacin and its metabolites.
A 60-minute intravenous infusion of 200 mg ciprofloxacin given every 12 hours, produced an equivalent area under the serum concentration time curve (AUC).
Distribution: Protein binding of ciprofloxacin is low (20-30%). Ciprofloxacin is present in plasma largely in a non-ionised form and has a large steady state distribution volume of 2-3 L/kg body weight. Ciprofloxacin reaches high concentrations in a variety of tissues such as lung (epithelial fluid, alveolar macrophages, biopsy tissue), sinuses, inflamed lesions (cantharides blister fluid), and the urogenital tract (urine, prostate, endometrium) where total concentrations exceeding those of plasma concentrations are reached.
Biotransformation: Low concentrations of four metabolites have been reported, which were identified as desethyleneciprofloxacin (M 1), sulphociprofloxacin (M 2), oxociprofloxacin (M 3) and formylciprofloxacin (M 4). The metabolites display in-vitro antimicrobial activity but to a lower degree than the parent compound. Ciprofloxacin is known to be a moderate inhibitor of the CYP 450 1A2 iso-enzymes.
Elimination: See table 3.
Click on icon to see table/diagram/image
Ciprofloxacin is largely excreted unchanged both renally and, to a smaller extent, faecally.
Renal clearance is between 180-300 mL/kg/h and the total body clearance is between 480-600 mL/kg/h. Ciprofloxacin undergoes both glomerular filtration and tubular secretion. Severely impaired renal function leads to increased half-lives of ciprofloxacin of up to 12 h.
Non-renal clearance of ciprofloxacin is mainly due to active trans-intestinal secretion and metabolism. 1% of the dose is excreted via the biliary route. Ciprofloxacin is present in the bile in high concentrations.
Pediatric patients: The pharmacokinetic data in pediatric patients are limited.
In a study in children C
max and AUC were not age-dependent (above one year of age). No notable increase in C
max and AUC upon multiple dosing (10 mg/kg three times daily) was observed.
In 10 children with severe sepsis C
max was 6.1 mg/L (range 4.6-8.3 mg/L) after a 1-hour intravenous infusion of 10 mg/kg in children aged less than 1 year compared to 7.2 mg/L (range 4.7-11.8 mg/L) for children between 1 and 5 years of age. The AUC values were 17.4 mg*h/L (range 11.8-32.0 mg*h/L) and 16.5 mg*h/L (range 11.0-23.8 mg*h/L) in the respective age groups. These values are within the range reported for adults at therapeutic doses. Based on population pharmacokinetic analysis of pediatric patients with various infections, the predicted mean half-life in children is approx. 4-5 hours and the bioavailability of the oral suspension ranges from 50 to 80%.
Susceptible microorganisms: E. coli, Shigella, Salmonella, Citrobacter, Klebsiella, Enterobacter, Serratia, Proteus (indole positive and negative), Pseudomonas, Neisseria, Acinetobacter, Streptococcus, Chlamydia, Staphylococcus, Corynebacterium, Bacteroides, Clostridium.
Infectious diseases: Respiratory Tract Infections; Ear, nose, throat infections; Kidney or urinary tract infections; Genital tract infections including gonorrhea; Infections of the gastrointestinal tract; Biliary tract infections; Infections of the skin and soft tissue; Infections of the bones and joints; Gynecological infections; Sepsis and peritonitis.
Because fluoroquinolones, including ciprofloxacin, have been associated with serious adverse reactions, reserve ciprofloxacin for treatment of acute exacerbation of chronic bronchitis, and simple urinary tract infections in patients who have no alternative treatment options.
Dosage: In care of adults, normally 100-400 mg is administered twice a day.
For the treatment of mild to moderate urinary tract infections, 200 mg is administered twice a day.
For severe or complicated urinary tract infections, 400 mg is given twice a day.
For the treatment of mild to moderate lower respiratory tract infections, skin or skin tissue infections, or bone and joint infections, 400 mg is administered twice a day. For the treatment of severe lower respiratory tract infections, skin or skin tissue infections, or bone and joint infections, 400 mg is administered three times a day.
Treatment period (Usual Duration): Usually the duration of therapy of ciprofloxacin is 7-14 days on average. For the bone or joint infection, it should be administered for 4 to 6 weeks or more. In addition, it should be administered for 2 days following after the symptoms of infection are resolved.
The method of administration: Ciprofloxacin injection should be administered by intravenous infusion over a period of 60 minutes. Dosage should be determined in consideration of severity of infection, susceptibility of pathogen, the status and hepatic/renal function of patients. After initial administration intravenously, conversion of intravenous to oral dosing can be applied in accordance with the status of patient.
Administration in patients with impaired renal function: When indicating for patients with renal impairments, some modification of dosage is recommended based upon the following table. If possible, it is recommended to adjust the dosage with monitoring of serum concentration of ciprofloxacin. (See Table 4.)
Click on icon to see table/diagram/image
When only the serum creatinine concentration is known, creatinine clearance may be estimated by the following formula. (See Equation.)
Click on icon to see table/diagram/image
Treatment for overdosage: In the event of acute overdosage, reversible renal toxicity has been reported in some cases. Observe the patient carefully and give supportive treatment, including monitoring of renal function, urinary pH and acidity, if required, to prevent crystalluria. Adequate hydration must be maintained. Calcium or magnesium containing antacids may theoretically reduce the absorption of ciprofloxacin in overdoses. Only a small amount of ciprofloxacin (less than 10%) is removed from the body after hemodialysis or peritoneal dialysis. ECG monitoring should be undertaken, because of the possibility of QT interval prolongation.
It is contraindicated for the patients as following: Patients with known hypersensitivity to ciprofloxacin or any quinolone antibacterial agents.
Pregnant women, women of childbearing potential or nursing mothers.
Children or growing adolescence under 18 years old.
Patients with epilepsy.
Patients with history of tendon ruptures or tendonitis associated with quinolone antibacterial agents or ciprofloxacin.
Patients receiving tizanidine (Concomitant administration of tizanidine and ciprofloxacin may increase the serum concentration of tizanidine, which may induce hypotension and somnolence. When concomitantly used, the increased serum concentration of tizanidine may induce hypotension or somnolence).
Patients receiving ketoprofen (Potential risk of convulsion).
Serious adverse reactions including tendinitis and tendon rupture, peripheral neuropathy, central nervous system effects, and exacerbation of myasthenia gravis: Fluoroquinolones, including ciprofloxacin, have been associated with disabling and potentially irreversible serious adverse reactions. Tendinitis and tendon rupture; Peripheral neuropathy; Central nervous system effects.
Discontinue ciprofloxacin immediately at the first signs or symptoms of any serious adverse reaction. In addition, avoid the use of fluoroquinolones, including ciprofloxacin, in patients who have experienced any of these serious adverse reactions associated with fluoroquinolones. Fluoroquinolones, including ciprofloxacin may exacerbate muscle weakness in patients with myasthenia gravis. Avoid ciprofloxacin in patients with known history of myasthenia gravis.
Because fluoroquinolones, including ciprofloxacin, have been associated with serious adverse reactions, reserve ciprofloxacin for use in patients who have no alternative treatment options for the following indications: Acute bacterial sinusitis, ABS; Acute bacterial exacerbation of chronic bronchitis, (ABECB); Uncomplicated urinary tract infections, UTI.
Ruptures of the shoulder, hand, Achilles tendon or other tendons that are required surgical repair or resulted in prolonged disability have been reported in patients with receiving quinolones. Post-marketing surveillance reports indicate that this risk is increased in patients taking corticosteroids, or in the elderly. Ciprofloxacin should be discontinued if the patients experience pain, inflammation, or rupture of a tendon. Patients should rest and refrain from exercise until the diagnosis of tendonitis or tendon rupture has been excluded. Tendon rupture can occur during or after therapy with quinolones, including ciprofloxacin.
Fluoroquinolones, including ciprofloxacin, have neuromuscular blocking activity and may exacerbate muscle weakness in patients with myasthenia gravis. Post marketing serious adverse reactions, including deaths and requirement for ventilator support, have been associated with fluoroquinolone use in patients with myasthenia gravis.
Healthcare professionals are advised to avoid prescribing fluoroquinolones to patients who have aortic aneurysm or at risk for an aortic aneurysm, such as patients with peripheral atherosclerotic vascular disease, hypertension, certain genetic conditions such as Marfan syndrome and Ehlers-Danlos syndrome, and elderly patients. The benefit of using fluoroquinolones to these patients should be assessed by the prescribers prior to initiation of therapy. It should be prescribed to these patients only when no other treatment options are available.
Ciprofloxacin is administered cautiously to the following patients: Patients with severe renal impairments.
Patients with history of convulsive diseases (Potential risk of convulsion).
Elderly patients.
Patients with known or suspected CNS disorders, e.g., severe cerebral arteriosclerosis (Potential risk of convulsion).
Patients with vein disorders.
Patients with myasthenia gravis (May worsen the symptoms).
Patients receiving theophylline.
Patients with deficiency of glucose-6-phosphate dehydrogenase (G-6-PD) (Hemolysis may occur rarely).
Patients receiving phenylacetate (e.g., fenbufen, flurbiprofen) or propionate non-steroidal anti-inflammatory drugs (Potential risk of convulsion).
General precautions: To reduce the development of drug-resistant bacteria, it is recommended that ciprofloxacin should be used for the minimum period required for the treatment after determining the susceptibility of the bacteria to ciprofloxacin.
As like other quinolones, ciprofloxacin has been known to trigger seizures or lower the seizure threshold. In patients with increased risk of epilepsy and CNS disorders (e.g., decreased seizure threshold, history of convulsion, decreased cerebral blood flow, changes in brain structure or stroke), CNS adverse reactions may occur and therefore they should be informed with the risks. Ciprofloxacin should only be administered if the potential therapeutic benefit justifies the potential risk. In some cases, CNS reactions occurred following the first dose and in rare cases depression or psychotic reactions have progressed to suicidal ideation/thoughts and self-endangering behaviors as of attempted or completed suicide. When these depression, psychotic reactions, suicidal ideation and actions occur, discontinue ciprofloxacin and institute appropriate measures.
Pseudomembranous colitis has been reported with use of nearly all antibacterial agents, including ciprofloxacin, and may range in severity from mild to fatal colitis. Therefore, the patients with diarrhea after the administration of antibacterial agents should be cautious. Toxins produced by Clostridium difficile is reported to be the primary cause of the colitis. Discontinue ciprofloxacin immediately when pseudomembranous colitis is suspected, and appropriate adjunctive ± specific treatment (e.g., administration of oral vancomycin) should be instituted. Under this clinical condition, avoid using any medicines that may disturb the intestinal peristalsis.
Photosensitivity may occur due to ciprofloxacin. Patients should minimize or avoid exposure to excessive natural or artificial UV light in order to prevent any photosensitivity reactions (e.g., sunlight lamps or tanning beds). Discontinue the therapy if any signs for phototoxicity reactions (i.e., rash, eruption, pruritus) occur.
Sensory or sensorimotor polyneuropathy triggering dysesthesia, hypoesthesia, and perception disorder have been reported in patient receiving fluoroquinolones, including ciprofloxacin. If the patient experiences symptoms of peripheral neuropathy including pain, burning, tingling, numbness, and/or weakness, the patients should discuss with physicians before continuing the therapy.
Fluoroquinolones, including ciprofloxacin, have been associated with other central nervous system events, therefore, it could affect to the driving or operating machinery, especially when ciprofloxacin is taken with alcohol.
I.V. Infusion of sodium chloride contained in injection: In patients for whom sodium intake is of medical concern (patients with congestive heart failure, renal failure, nephrotic syndrome, etc.), the additional sodium load should be taken into account.
Ciprofloxacin has been associated with prolongation of the QT interval, caution should be taken in patients with known prolongation of the QT interval, risk factors for QT prolongation or torsade de pointes (for example, congenital long QT syndrome, uncorrected electrolyte imbalance, such as hypokalemia or hypomagnesemia and cardiac disease, such as heart failure, myocardial infarction, or bradycardia), and patients receiving Class IA antiarrhythmic agents (quinidine, procainamide), or Class III antiarrhythmic agents(amiodarone, sotalol), tricyclic antidepressants, macrolides, and antipsychotics. Women tend to have longer baseline QTc interval than men, which may lead them much sensitive to drugs known to delay QT interval.
Ciprofloxacin monotherapy is not suited for treatment of severe infections and infections that might be due to Gram-positive or anaerobic pathogens. In such infections ciprofloxacin must be co-administered with other appropriate antibacterial agents.
Ciprofloxacin is not recommended for the treatment of streptococcal infections due to inadequate efficacy.
Genital tract infections may be caused by fluoroquinolone-resistant Neisseria gonorrhoeae isolates. For genital tract infections, empirical ciprofloxacin should only be considered in combination with another appropriate antibacterial agent unless ciprofloxacin-resistant Neisseria gonorrhoeae can be excluded. If clinical improvement is not achieved after 3 days of treatment, the therapy should be reconsidered.
The in-vitro activity of ciprofloxacin against Mycobacterium tuberculosis might give false negative bacteriological test results in specimens from patients currently taking ciprofloxacin.
Local intravenous site reactions have been reported with the intravenous administration of ciprofloxacin. These reactions are more frequent if the infusion time is 30 minutes or less. These may appear as local skin reactions which resolve rapidly upon completion of the infusion. Subsequent intravenous administration is not contraindicated unless the reactions recur or worsen.
Cases of hepatic necrosis, life-threatening hepatic failure have been reported with ciprofloxacin. In the event of any signs and symptoms of hepatitis (such as anorexia, jaundice, dark urine, pruritus, or tender abdomen), discontinue treatment immediately. There can be a temporary increase in transaminases, alkaline phosphatase, or cholestatic jaundice in patients with previous liver damage, who are treated with ciprofloxacin.
Monitor the patient for rare shock. Discontinue ciprofloxacin when hypotensive, dyspnea, feeling of pressure to the chest occurs, and institute appropriate measures.
Cautions should be taken in patients with ciprofloxacin since rhabdomyolysis accompanied with acute decline in renal function, which features muscle pain, impotent feeling, elevated creatinine kinase (CK), and serum, urine myoglobin, can occur. Muscle weakness can occur, and the symptoms may be worsened especially in patients with myasthenia gravis.
Interstitial pneumonia accompanied with cough, dyspnea, and abnormalities in chest x-rays, eosinophilia, and other symptoms may occur. Discontinue ciprofloxacin when these symptoms occur and give patient appropriate treatment such as administration of adrenocortical steroids.
Use in Children: Quinolones, including ciprofloxacin, cause arthropathy and osteochondrosis in weight bearing joints of juvenile animals. In addition, the safety data showed no evidence of cartilage or joint damage in association with ciprofloxacin when used in juvenile cystic fibrosis patients under 18 years old.
Ciprofloxacin should not be used in pediatric population and growing adolescent under age 18 for the safety and efficacy of ciprofloxacin to these patients have not been established.
Use in the Elderly: Ciprofloxacin is known to be substantially excreted by the kidney. Since some older individuals experience reduced renal function by virtue of their advance age, care should be taken in dose selection for elderly patients.
Use in pregnant women and nursing mothers: Effects on immature cartilage have been observed in the non-clinical studies, thus, it cannot be excluded that the drug could cause damage to articular cartilage in the human immature organism/fetus. Ciprofloxacin should not be used during pregnancy or to women with potentials of childbearing, for its safety in pregnant women has not been established. Animal test did not show potentials of teratogenicity.
Ciprofloxacin is excreted in breast milk. Ciprofloxacin should not be used during breast-feeding or do not breast-feed during the therapy.
See Table 5.
Click on icon to see table/diagram/image
Adverse reactions reported with Ciprofloxacin are summarized in the table. In each frequency category, adverse reactions are presented in the order of severity. Frequencies are defined as Very common (≥1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1000 to <1/100), Rare (≥1/10,000 to <1/1,000), and Very Rare (<1/10,000). If it cannot be estimated from the available data, the frequency is defined as Unknown. MedDRA terminology is used to describe specific reactions, their analogies, and related conditions. ADR terminology is based on MedDRA version 14.0 except for fungal infections and unidentified pains.
Following adverse reactions are added based on analysis and assessment of reported adverse reactions in Korea.
Skin: Maculopapule, Rash, Purpuric eruption.
Injection site: Rash, Pruritus, Urticaria.
Ciprofloxacin is an inhibitor of human cytochrome P450 1A2 (CYP1A2) mediated metabolism. Co-administration of ciprofloxacin with other drugs primarily metabolized by CYP1A2 (e.g. theophylline, clozapine, olanzapine, ropinirole, tizanidine, duloxetine, agomelatine) results in increased plasma concentrations of these drugs and could lead to clinically significant adverse events of the co-administered drug. Concurrent administration of ciprofloxacin and theophylline can cause an undesirable increase in serum theophylline concentration. This can lead to theophylline-induced adverse reactions (e.g., cardiac arrest, seizure, status epilepticus, and respiratory failure) that may rarely be life threatening or fatal. If concomitant use cannot be avoided, monitor serum levels of theophylline and adjust dosage as appropriate.
Co-administration of ketoprofen with ciprofloxacin can rarely cause seizures, therefore it is not concurrently used. Co-administration of phenylacetic acid-derived (e.g. fenbufen, flubiprofen) or propionic acid-derived non-steroidal anti-inflammatory drugs with ciprofloxacin can rarely cause seizures, therefore concurrently use with caution. Non-steroidal anti-inflammatory drugs (but not acetyl salicylic acid) in combination of very high doses of quinolones have been shown to provoke convulsions in pre-clinical studies.
Cmax and AUC of ciprofloxacin are slightly diminished when given concomitantly with omeprazole.
Simultaneous administration of ciprofloxacin with anti-coagulant drugs such as warfarin may augment its anti-coagulant effects. The risk may vary with the underlying infection, age and general status of the patient so that the contribution of ciprofloxacin to the increase in INR (international normalized ratio) is difficult to assess. The INR should be monitored frequently during and shortly after co-administration of ciprofloxacin with anti-coagulant drugs.
As with other quinolones, hypoglycemia sometimes severe has been reported when ciprofloxacin and oral antidiabetic agents, mainly sulfonylureas (for example, glyburide, glimepiride), were co-administered.
Concomitant administration of cyclosporine with ciprofloxacin may increase serum concentration of cyclosporine and elevate serum creatinine. For these patients, it is necessary to monitor serum creatinine more frequently (twice a week).
Probenecid may interfere with renal tubular secretion of ciprofloxacin, decreasing therapeutic effect in treatment of urinary tract infections, and increase the level of ciprofloxacin in serum.
Renal tubular transport of methotrexate may be inhibited by concomitant administration of ciprofloxacin, potentially leading to increased plasma levels of methotrexate and increased risk of methotrexate-associated toxic reactions. Therefore, carefully monitor patients under methotrexate therapy when concomitant ciprofloxacin therapy is indicated.
In a clinical study with healthy subjects, there was an increase in serum tizanidine concentration (Cmax increase: 7-fold, range: 4 to 21-fold; AUC increase: 10-fold, range: 6 to 24-fold) when given concomitantly with ciprofloxacin. Increased serum tizanidine concentration is associated with a potentiated hypotensive and sedative effect. Therefore, tizanidine must not be administered together with ciprofloxacin.
Simultaneous administration of ciprofloxacin and phenytoin may result in increased or reduced serum levels of phenytoin. To avoid the loss of seizure control associated with decreased phenytoin levels and to prevent phenytoin overdose-related adverse reactions upon ciprofloxacin discontinuation in patients receiving both agents, monitor phenytoin therapy, including phenytoin serum concentration during and shortly after co-administration of ciprofloxacin with phenytoin.
On concurrent administration of ciprofloxacin and caffeine or pentoxifylline, reduced clearance resulting in elevated levels and prolongation of serum half-life of caffeine or pentoxifylline.
The serum concentration of ciprofloxacin and metronidazole were not altered when these two drugs were given concomitantly.
Ropinirole: It was shown in a clinical study that concomitant use of ropinirole with ciprofloxacin, a moderate inhibitor of the CYP450 1A2 isozyme, results in an increase of Cmax and AUC of ropinirole by 60% and 84% respectively. Although ropinirole treatment was well tolerated, a possible interaction with ciprofloxacin associated with side effects may occur upon concomitant administration.
Lidocaine: It was demonstrated in healthy subjects that concomitant use of lidocaine containing medicinal products with ciprofloxacin, a moderate of CYP450 1A2 isozyme, reduces clearance of intravenous lidocaine by 22%. Although lidocaine treatment was well tolerated, a possible interaction with ciprofloxacin associated with side effects may occur upon concomitant administration.
Ciprofloxacin may affect QT interval. It should be used with caution when treated with drugs such as Class IA or III anti-arrhythmic. Ciprofloxacin should be used with caution in patients receiving drugs known to prolong QT interval (e.g. Class IA and III anti-arrhythmic).
Following concomitant administration of 250 mg ciprofloxacin with clozapine for 7 days, serum concentrations of clozapine and N-desmethylclozapine were increased by 29% and 31% respectively. Clinical surveillance and appropriate adjustment of clozapine dosage during and shortly after co-administration with ciprofloxacin are advised.
Serum level and AUC of sildenafil twiced when co-administered with 50 mg of sildenafil and 500 mg of ciprofloxacin in healthy subject. Therefore, consider the benefits of treatment and the risks, closely monitor the patient in concomitant use of ciprofloxacin and sildenafil.
Agomelatine: Fluvoxamine, a strong inhibitor of CYP450 1A2 enzyme, remarkably inhibits the metabolism of agomelatine, resulting 60 times increase in exposure of agomelatine in clinical test. There is no clinical data supporting interactions between ciprofloxacin and agomelatine, but co-administration with agomelatine is contraindicated.
Zolpidem: It is not recommended to co-administer ciprofloxacin with zolpidem, for there is risk of increase in serum zolpidem level.
Precautions in use: As the infusion solution is sensitive to light, only remove the infusion bag from the outer foil wrap for use. In daylight, the full efficacy of the solution is guaranteed over a period of 3 days.
The ciprofloxacin infusion solution is compatible with Ringer's solution, Lactated Ringer's solution, 5% and 10% dextrose solutions, 5% Dextrose and 0.225% Sodium Chloride solution, and 5% Dextrose and 0.45% Sodium Chloride solution. When ciprofloxacin infusion solutions are mixed with compatible infusion solutions, for microbial reasons and light sensitivity these solutions must be administered shortly after admixture.
Unless compatibility with other solutions/drugs has been confirmed, the infusion solution must always be administered separately. The visual sign of incompatibility are e.g. precipitation, clouding, and discoloration.
Incompatibility appears with all infusion solutions/drugs that are physically or chemically unstable at the pH of the solutions (e.g. penicillins, heparin solutions), especially in combination with solutions adjusted to an alkaline pH (pH of ciprofloxacin solutions: 3.9-4.5).
Precautions in storage and handling: Do not transfer ciprofloxacin from the original package to one another. It may result in accidents and/or deteriorate the quality of ciprofloxacin.
Ciprofloxacin should be stored under protection from the direct rays of light and UV light.
At cool temperatures precipitation may occur, which will re-dissolve at room temperature (15°C-25°C). Therefore, do not store the injection in the refrigerator.
Others: From comparative studies in animals, both with the pre-existing quinolone antibacterial agents (e.g., nalidixic and pipemidic acid) and more recently developed agents (e.g., norfloxacin and ofloxacin), it is known that this substance class produces a characteristic damage pattern; damage to kidney, eye, and cartilage in weight-bearing joints of immature animals may be encountered.
Crystalluria has been reported by excessive administration (750 mg/more than once).
Store in a dry place at temperatures not exceeding below 30°C, protect from light. Do not refrigerate.
Shelf-life: 24 months.
J01MA02 - ciprofloxacin ; Belongs to the class of fluoroquinolones. Used in the systemic treatment of infections.
Ciclodin IV Infusion Bag soln for IV inj 2 mg/mL (200 mg/100 mL)
100 mL x 30 × 1's
Ciclodin IV Infusion Bag soln for IV inj 2 mg/mL (400 mg/200 mL)
200 mL x 20 × 1's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image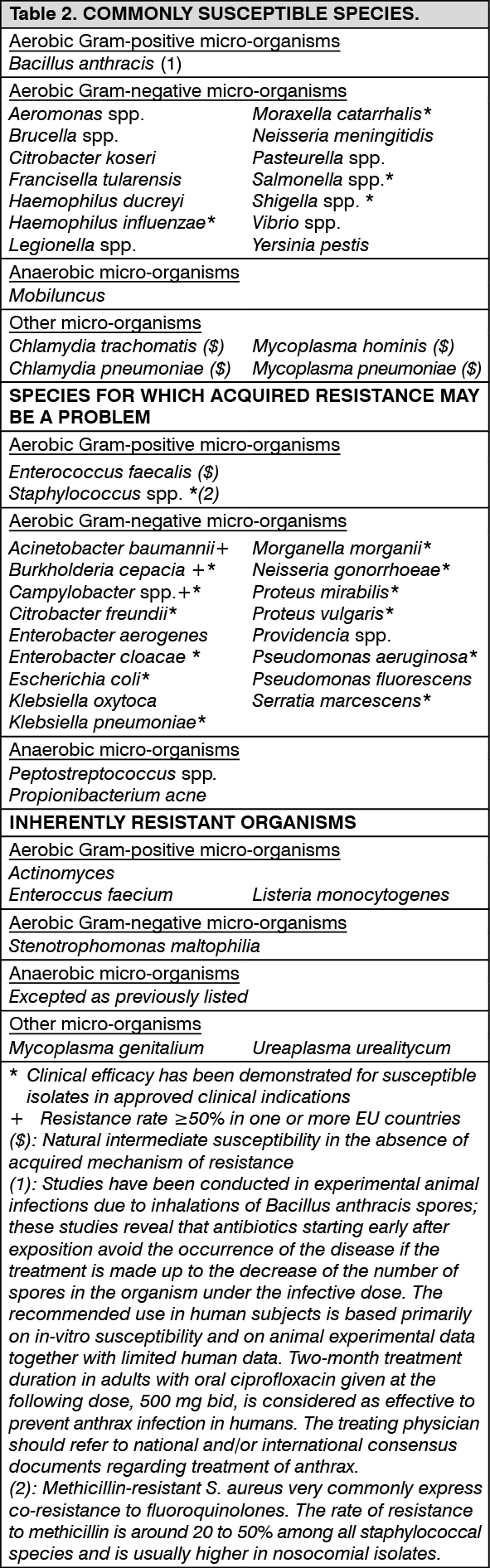 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image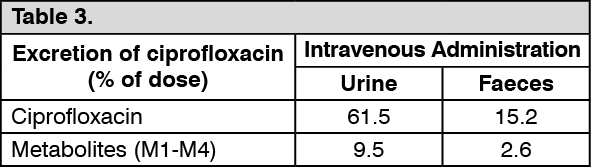 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image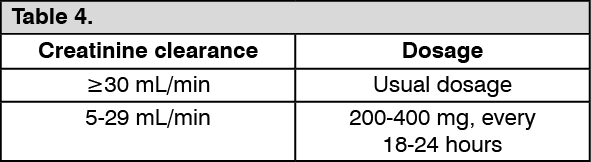 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image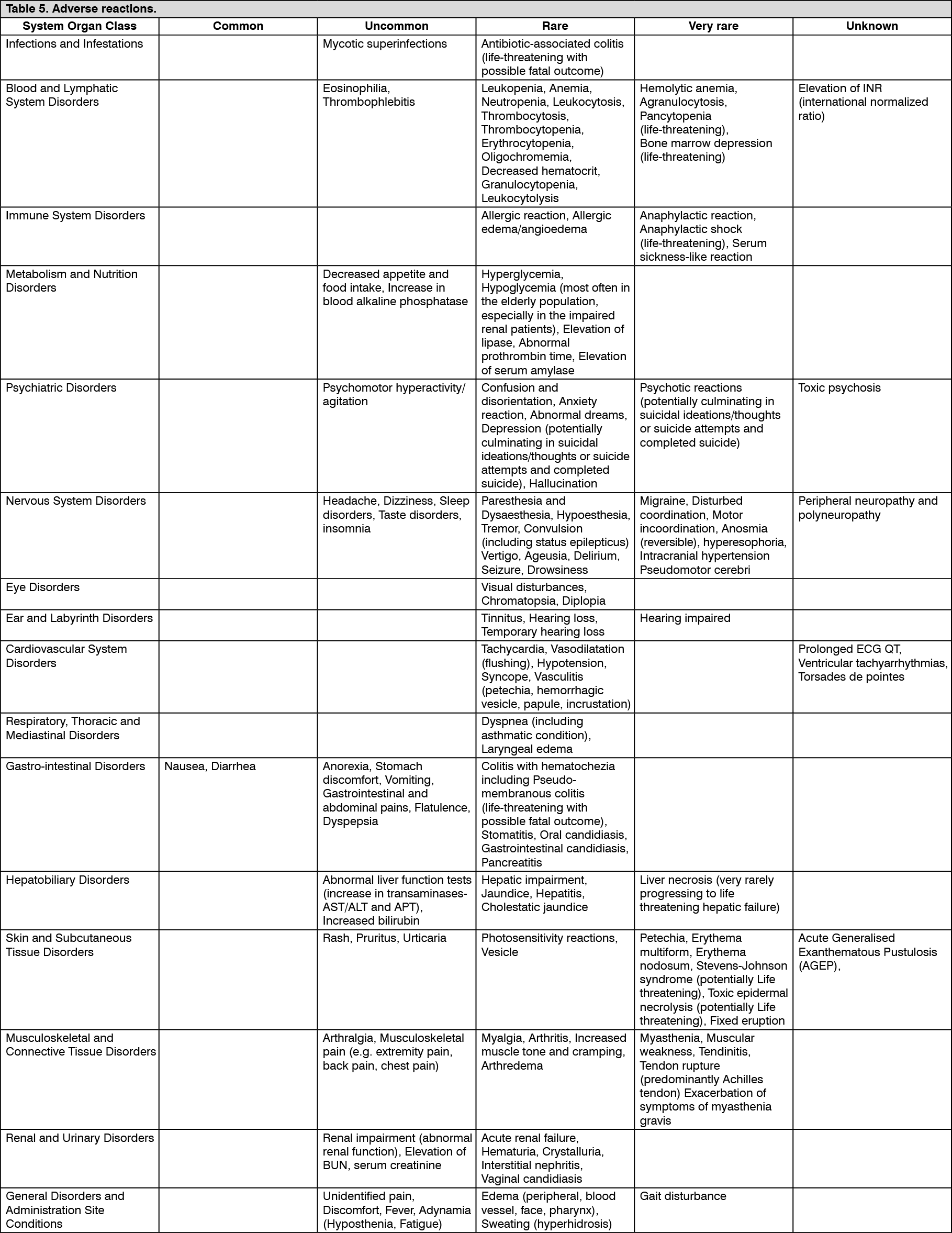 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageab96fa49-1198-4b1f-9c8d-b27a007ef355.GIF)
451b10fc-8c3f-4518-8692-b27a007ef37a.GIF)

 Sign Out
Sign Out