Dosage should be adjusted to the stage, severity, and type of infection, weight of the patient and sensitivity of the pathogen. Duration of therapy should be governed by the response of the patient, and to a less extent by the sensitivity of the organism as determined by periodic in-vitro test. It must be remembered that when antibiotic therapy is interrupted for significant periods, resumption of therapy may be less successful owing to the development in the interim of resistant organisms.
In the presence of impaired renal function the dosage must be adjusted carefully. Since excretion is decreased the drug is retained and concentration in the blood may be abnormally high. Thus lower dosage than usual may be therapeutically effective while the usual dosage may cause serious toxic reactions.
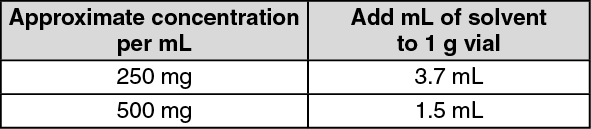
Dissolve contents of vial aseptically by adding Water for Injection U.S.P. according to the following table. Do not mix solutions of streptomycin sulfate with streptomycin calcium chloride complex as an insoluble precipitate will form. Use only clear solutions, free of undissolved particles. A slight discoloration that may develop in solutions on standing does not impair their effectiveness. Refrigeration minimizes discoloration. Sterile solutions may be stored at room temperature for 4 weeks without significant loss of potency. They should not be autoclaved.
In determining the volume of solvent to be added in the vial, it is necessary to take into account that each gram equivalent of the streptomycin powder itself contributes to the volume of the solution made. The dilution table given below has been calculated with a slight excess of solvent to allow for the amount of solution that normally adheres to vial, syringe and needle. See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
For systemic action, streptomycin should be injected intramuscularly. To avoid pain which sometimes follow injection in sensitive persons, care should be taken to make a deep intramuscular injection. The site of choice is the buttock and to assure avoiding the sciatic nerve, the upper outer quadrant should be used. If alternate sites become necessary, the quadriceps femoris, triceps or deltoid muscles may be substituted. When the deltoid is chosen as the site of injection, care must be taken to avoid the bursa. In all instances, care must be taken to avoid intravenous injection.
Tuberculosis: Tuberculosis (other than miliary and meningeal): 1 g intramuscularly 2 or 3 times a week or daily. Daily dosage is advisable in patients with severe or highly acute forms of the disease.
Paraaminosalicylic acid (12 g daily in divided doses) or isoniazid (approximately 300 mg daily in divided doses) should be given concomitantly. This combined chemotherapy inhibits or delays the emergence of tubercle bacilli resistant to streptomycin and allows the duration of administration of streptomycin to be extended effectively often to 1 year or more.
Appropriate forms of collapse therapy may be advisable early in the course of treatment of pulmonary tuberculosis. However, with combined intermittent therapy surgical procedures are frequently postponed until a maximal clinical and X-ray response is achieved and the patient thus becomes a better operative risk. This may require 9 to 12 months or more of combined chemotherapy.
Miliary tuberculosis and when elected, meningeal tuberculosis: 1 g intramuscular daily usually is adequate, although some cases may require 2 to 3 g daily in divided doses. P-aminosalicylic acid or isoniazid should be given concomitantly as outlined above. Treatment of these serious types of the disease must be prolonged usually for 1 year or longer.
Surgical intervention in tuberculous patients: For short term prophylaxis 1 g is given intramuscularly daily for about 2 to 7 days before operation to reduce the sputum volume and make the patient a better surgical risk. The drug is continued after operation for 14 to 28 days or more if a therapeutic objective still remains. Again in this instance, combination with other agents is essential.
Non-Tuberculous Infections: Gonorrhea: when penicillin is allergenic, unavailable, cir not promptly effective (furthermore, coexistent syphilis is not likely to be masked). One intramuscular injection of 0.3 to 0.5 g usually is sufficient. Before treatment dark-field examination should be made of the exudates from any lesions, and after treatment, monthly serologic tests for syphilis should be made for at least 3 months.
Subacute bacterial endocarditis: due to penicillin-resistant, streptomycin-sensitive organisms. At least 2 g intramuscularly daily in divided doses for a minimum of 6 weeks. Treatment is preferably preceded by isolation of the organism and establishment of its sensitivity to streptomycin. About four times the dose necessary to kill the organism
in vitro is required. In endocarditis due to enterococcus a combination of penicillin and streptomycin has been highly effective.
Brucellosis with bacteremia: 1 g intramuscularly every 12 hours for 1 week, then 1 g daily for the second week. This therapy should be augmented by the use of other effective antibiotics.
Urinary tract infections due to susceptible organism (elimination of urinary obstruction is essential): 1 to 2.5 g intramuscularly daily for 5 to 7 days (higher dosage for 14 days in severe infections). Use divided doses when larger daily dosage is employed. Sensitivity tests should be performed where the response is slow or unsatisfactory because of the rapidity with which gram-negative organisms develop resistance to streptomycin.
Perionitis: due to gram-negative bacilli 2 to 2.5 g daily in divided doses for 7 to 14 days. Supplementary treatment with penicillin and sulfonamides is advised. Other antibiotics should be used if sensitivity studies so indicate.
Other nontuberculous infections (due to sensitive organisms): Meningitis, pulmonary infections and laryngotracheitis due to
Hemophilus influenzae, meningitis and bacteremia due to susceptible strains of
Escherichia coli,
Proteus vulgaris,
Aerobacter aerogenes,
Pseudomonas aeruginosa,
Klebsiella pneumoniae, and
Salmonella, pneumonia due to
K. pneumoniae, tularemia, plague, chancroid, when sulfonamides are allergenic, unavailable or not effective; granuloma inguinale, liver abscesses, cholangitis, chronic pulmonary infection and emphysema due to susceptible organisms, enteritis due to susceptible strains of
Salmonella and
Shigella. When used preoperatively for the reduction of intestinal bacteria (Including
Proteus and
Pseudomonas organisms), supplemental therapy with other antibiotics is usually necessary. A daily dosage of 1 to 3 g intramuscularly depending on the severity of the infection, is usually effective. Use divided doses when larger daily dosage is employed. Continue treatment for at least 48 to 72 hours after the temperature returns to normal and all signs of infection have disappeared. In enteritis and gastrointestinal prophylaxis 0.5 to 1 g orally every 6 hours is recommended concomitantly with regular intramuscular injections to combat systemic invasion by susceptible pathogens. Supplemental therapy with other antibiotics is usually necessary.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out