



 Sign Out
Sign Out
Pharmacology: Cefepime is a semi-synthetic, broad spectrum, fourth generation cephalosporin for parenteral administration which is active against a wide range of Gram-positive, Gram-negative aerobic organisms and certain anaerobes. It exerts bactericidal effect by inhibiting the synthesis of the bacterial cell wall. Its activity against Gram-positive cocci is similar to that of cefotaxime and includes staphylococci (but not methicillin-resistant Staphylococcus aureus) and streptococci. It has a broader spectrum of activity against Enterobacteriaceae than other cephalosporins, including organisms that produce chromosomally mediated beta-lactamases such as Enterobacter species and Proteus vulgaris. It has a similar or slightly less activity than ceftazidime against Pseudomonas aeruginosa, although it may be active against some strains resistant to ceftazidime.
Pharmacokinetics: Bioavailability: Cefepime is rapidly and almost completely absorbed after intramuscular (IM) injection. After 1.5 hours of 500 mg and 1 g doses, mean peak plasma concentrations in adults are 14 and 30 mcg/mL, respectively. Peak plasma concentrations of about 40 and 80 mcg/mL are reported within 30 minutes of similar intravenous (IV) doses. In children 2 months to 16 years old who received a single 50 mg/kg IM dose, average plasma concentrations are 76, 75.2, 64, and 4.8 mcg/mL at 0.5, 0.75, 1, and 8 hours, respectively. Intravenous administration of a single 50 mg/kg dose of cefepime in pediatric patients results in cefepime concentrations similar to adults after IV administration of a single 2 g dose of the drug.
Cefepime is widely distributed into tissues and fluids, including blister fluid, bronchial mucosa, sputum, bile, peritoneal fluid, appendix, gall bladder, prostate and cerebrospinal fluid. The average steady state volume of distribution of cefepime is 18 (± 2) L. The serum protein binding of cefepime is approximately 20% and is independent of its concentration in serum.
Cefepime is metabolized to N-methylpyrrolidine (NMP) which is rapidly converted to the N-oxide. Elimination of cefepime is principally via the kidneys with an average (± SD) half-life of 2 (±0.3) hours and total body clearance of 120 (±8) mL/min in healthy volunteers. About 85% of the dose is recovered unchanged in the urine.
Studies in adults with renal impairment indicate that pharmacokinetics (PK) of cefepime are affected by the degree of renal impairment and that total body clearance of the drug decreases in proportion to decreases in creatinine clearance. Patients with renal dysfunction and those undergoing hemodialysis require dosing adjustment. Hepatic impairment does not affect pharmacokinetics of cefepime.
Cefepime is removed by hemodialysis and peritoneal dialysis.
Microbiology: Antimicrobial Spectrum of Activity: Cefepime has been shown to be active against most strains of the following microorganisms both in vitro and in clinical infections: See Table 1.
 Click on icon to see table/diagram/image
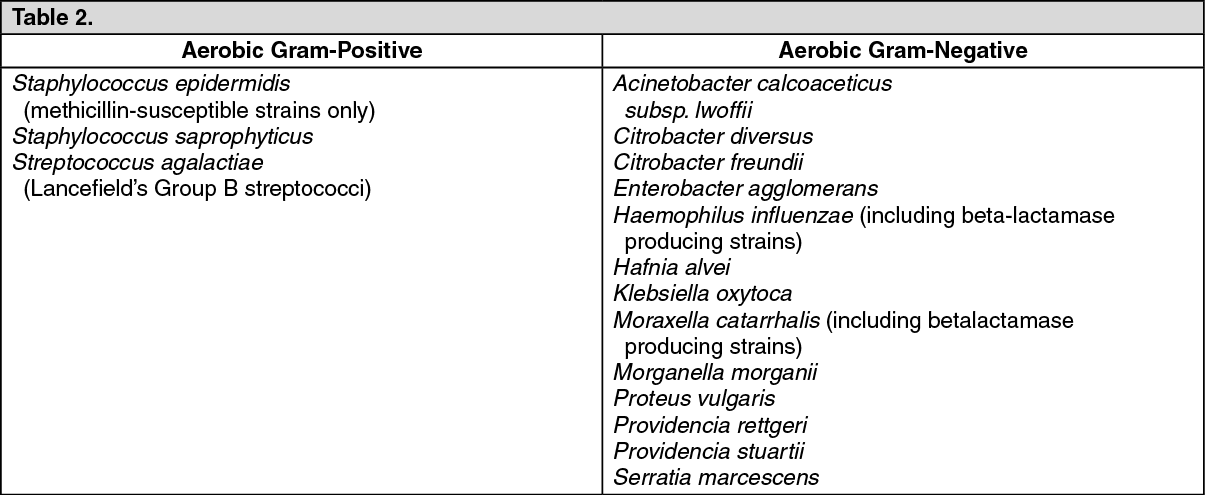
Click on icon to see table/diagram/imageCefepime has been shown to be active in vitro against most strains of the following organisms; however, the clinical significance of these data is unknown: See Table 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMost strains of enterococci, e.g., Enterococcus faecalis, and methicillin-resistant staphylococci are resistant to cefepime.
Cefepime is inactive against many strains of Stenotrophomonas (formerly Xanthomonas maltophilia and Pseudomonas maltophilia).
Cefepime is inactive against most strains of Clostridium difficile.
It is suggested to carry out susceptibility tests.