



 Sign Out
Sign Out
 Click on icon to see table/diagram/image
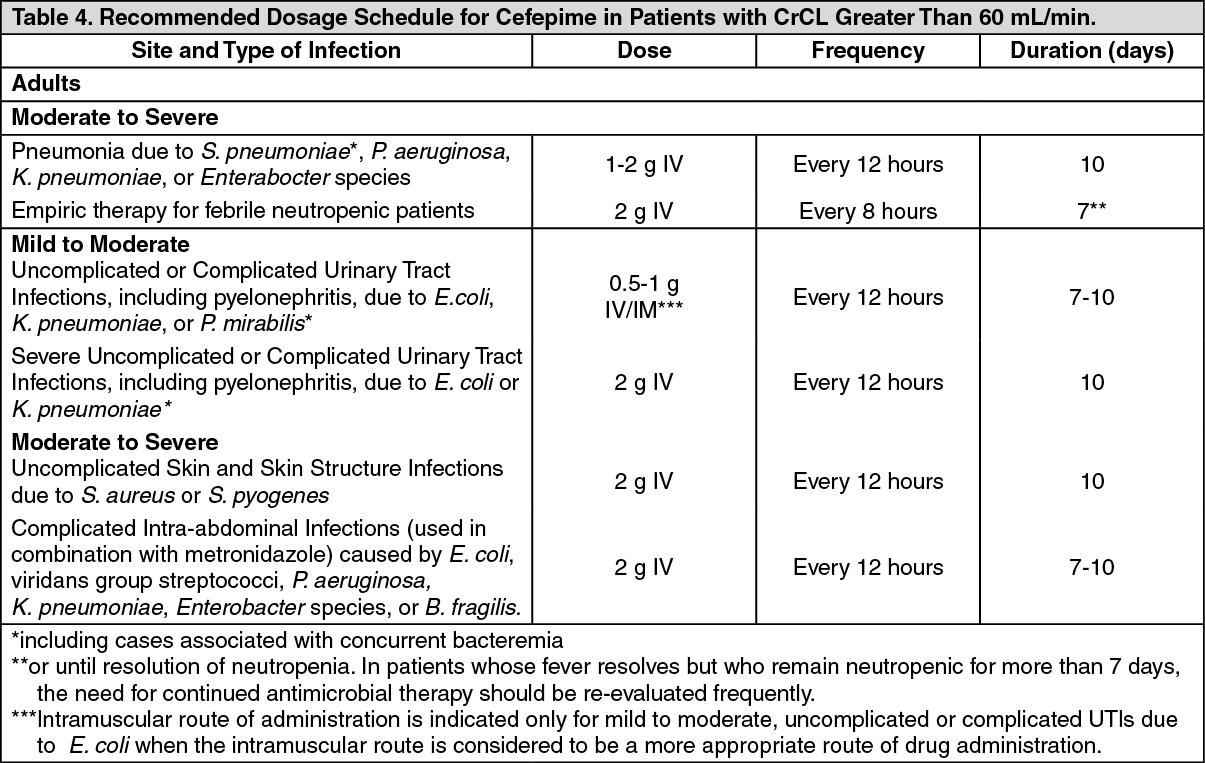
Click on icon to see table/diagram/imagePediatric Patients (2 months up to 16 years): The maximum dose for pediatric patients should not exceed the recommended adult dose. The usual recommended dosage in pediatric patients up to 40 kg in weight for uncomplicated and complicated urinary tract infections (including pyelonephritis), uncomplicated skin and skin structure infections, and pneumonia is 50 mg per kg per dose, administered every 12 hours (50 mg per kg per dose, every 8 hours for febrile neutropenic patients), for durations as given previously.
Patients with Hepatic Impairment: No adjustment is necessary for patients with hepatic impairment.
Patients with Renal Impairment: In patients with creatinine clearance less than or equal to 60 mL/min, the dose of Cefepime should be adjusted to compensate for the slower rate of renal elimination. The recommended initial dose of Cefepime should be the same as in patients with normal renal function except in patients undergoing hemodialysis. The recommended doses of Cefepime in patients with renal impairment are presented in Table 5.
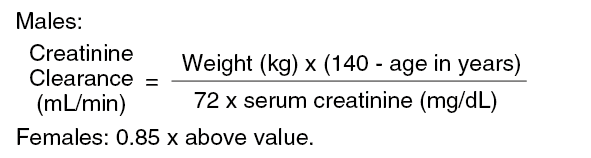
When only serum creatinine is available, the following formula (Cockroft and Gault equation) may be used to estimate creatinine clearance. The serum creatinine should represent a steady state of renal function: (See Formula.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image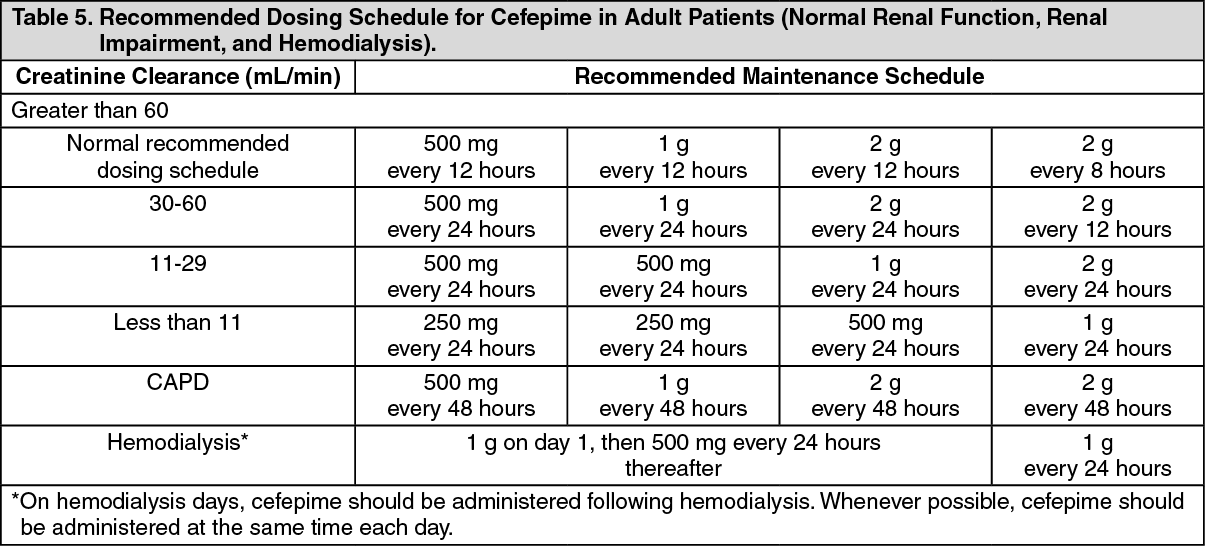 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn patients undergoing continuous ambulatory peritoneal dialysis, Cefepime may be administered at normally recommended doses at a dosage interval of every 48 hours (see Table 5).
In patients undergoing hemodialysis, approximately 68% of the total amount of cefepime present in the body at the start of dialysis will be removed during a 3-hour dialysis period. The dosage of Cefepime for hemodialysis patients is 1 g on Day 1 followed by 500 mg every 24 hours for the treatment of all infections except febrile neutropenia, which is 1 g every 24 hours. Cefepime should be administered at the same time each day and following the completion of hemodialysis on hemodialysis days (see Table 5).
Data in pediatric patients with impaired renal function are not available; however, since cefepime pharmacokinetics are similar in adults and pediatric patients, changes in the dosing regimen proportional to those in adults (see Tables 4 and 5) are recommended for pediatric patients.
Administration: Intravenous Administration: For intravenous infusion, constitute the 500 mg, 1 g, or 2 g vial, and add an appropriate quantity of the resulting solution to an intravenous container with one of the compatible intravenous fluids listed in Cautions for Usage. The resulting solution should be administered over approximately 30 minutes.
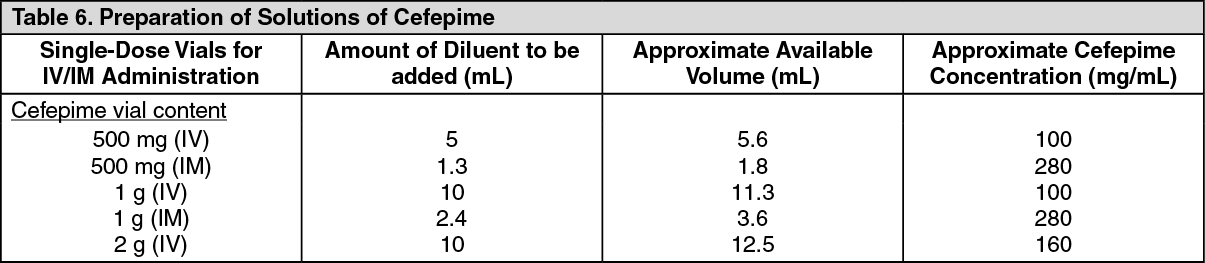
Intramuscular Administration: For intramuscular administration, Cefepime (cefepime hydrochloride) should be constituted with one of the following diluents: Sterile Water for Injection, 0.9% Sodium Chloride, 5% Dextrose Injection, 0.5% or 1.0% Lidocaine Hydrochloride, or Sterile Bacteriostatic Water for Injection with Parabens or Benzyl Alcohol (see Table 6).
Preparation of Cefepime solutions is summarized in Table 6.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image