The most frequent adverse reaction associated with Alteplase (Actilyse) is bleeding (≥1:100 to, <1:10: major bleeds; ≥1:10: any haemorrhage) resulting in a fall in haematocrit and/or haemoglobin values. Haemorrhage at any site or body cavity can occur and may result in life-threatening situations, permanent disability or death.
The type of bleeds associated with thrombolytic therapy can be divided into two broad categories: superficial bleeding, normally from punctures or damaged blood vessels; internal bleeding at any site or body cavity.
With intracranial haemorrhage neurological symptoms such as somnolence, aphasia, hemiparesis, convulsion may be associated.
The number of patients treated in clinical trials in the indications acute massive pulmonary embolism and acute ischaemic stroke (within the 0-4.5 hours time window) was very small in comparison to the number in the trial acute for myocardial infarction. Therefore, small numerical differences observed in comparison with the number in acute myocardial infarction were presumably attributable to the small sample size. Except for intracranial haemorrhage as side effect in the indication acute ischaemic stroke as well as for reperfusion arrhythmias in the indication acute myocardial infarction there is no medical reason to assume that the qualitative and quantitative side effect profile of Alteplase (Actilyse) in the indications acute massive pulmonary embolism and acute ischaemic stroke is different from the profile in the indication acute myocardial infarction.
List of adverse reactions: Immune system disorders: anaphylactoid reactions, which are usually mild, but can be life threatening in isolated cases.
They may appear as: rash, urticaria, bronchospasm, angio-oedema, hypotension, shock or any other symptom associated with hypersensitivity.
Nervous system disorders: intracranial haemorrhage such as cerebral haemorrhage, cerebral haematoma, haemorrhagic stroke, haemorrhagic transformation stroke, intracranial haematoma, subarachnoid haemorrhage.
Eye disorders: eye haemorrhage.
Cardiac disorders: pericardial haemorrhage.
Vascular disorders: haemorrhage, such as haematoma; embolism which may lead to corresponding consequences in the organs concerned; bleeding of parenchymatous organs such as hepatic haemorrhage.
Respiratory, thoracic and mediastinal disorders: respiratory tract haemorrhage, such as pharyngeal haemorrhage, haemoptysis, epistaxis, pulmonary haemorrhage.
Gastrointestinal disorders: gastrointestinal haemorrhage such as gastric haemorrhage, gastric ulcer haemorrhage, rectal haemorrhage, haematemesis, melaena, mouth haemorrhage, gingival bleeding; retroperitoneal haemorrhage, such as retroperitoneal haematoma; nausea; vomiting.
Nausea and vomiting can also occur as symptoms of myocardial infarction.
Skin and subcutaneous tissue disorders: ecchymosis.
Renal and urinary disorders: urogenital haemorrhage, such as haematuria, haemorrhage urinary tract.
General disorders and administration site conditions: injection site haemorrhage, puncture site haemorrhage, such as catheter site haematoma, catheter site haemorrhage.
Investigations: blood pressure decreased, body temperature increased.
Injury and poisoning and procedural complications: fat embolism*, which may lead to corresponding consequences in the organs concerned.
Surgical and medical procedures: transfusion.
* Fat embolism, was not observed in the clinical trial population, but was found in spontaneous reporting.
List of additional adverse reactions for the indication acute myocardial infarction:
Cardiac disorders: reperfusion arrhythmia, such as: arrhythmia, extrasystoles, atrial fibrillation, atrioventricular block first degree to atrioventricular block complete, bradycardia, tachycardia, ventricular arrhythmia, ventricular fibrillation, ventricular tachycardia occurs in close temporal relationship to treatment with Alteplase (Actilyse).





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image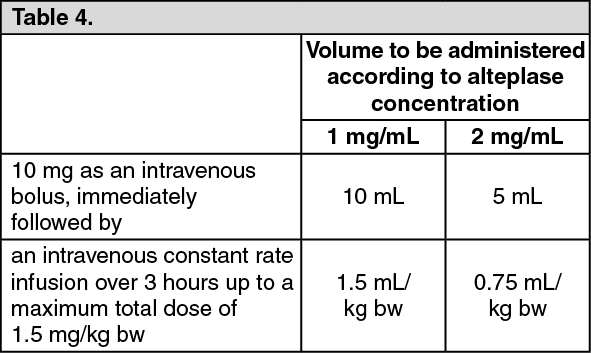 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image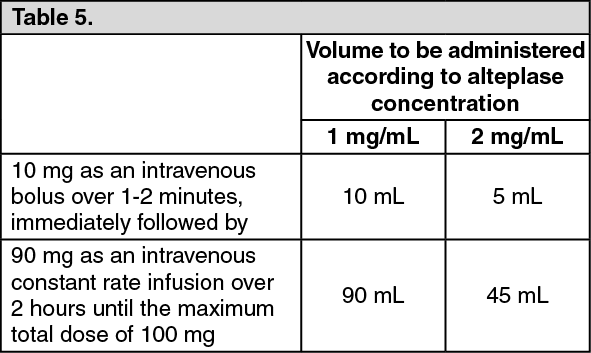 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image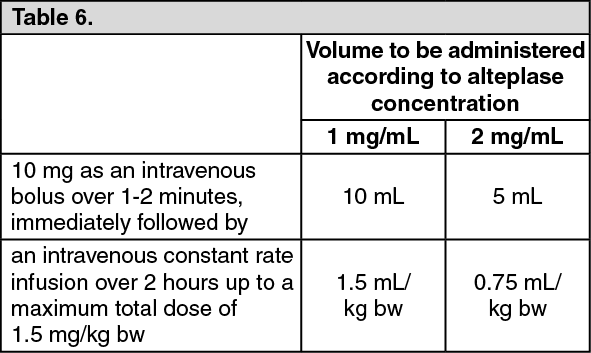 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image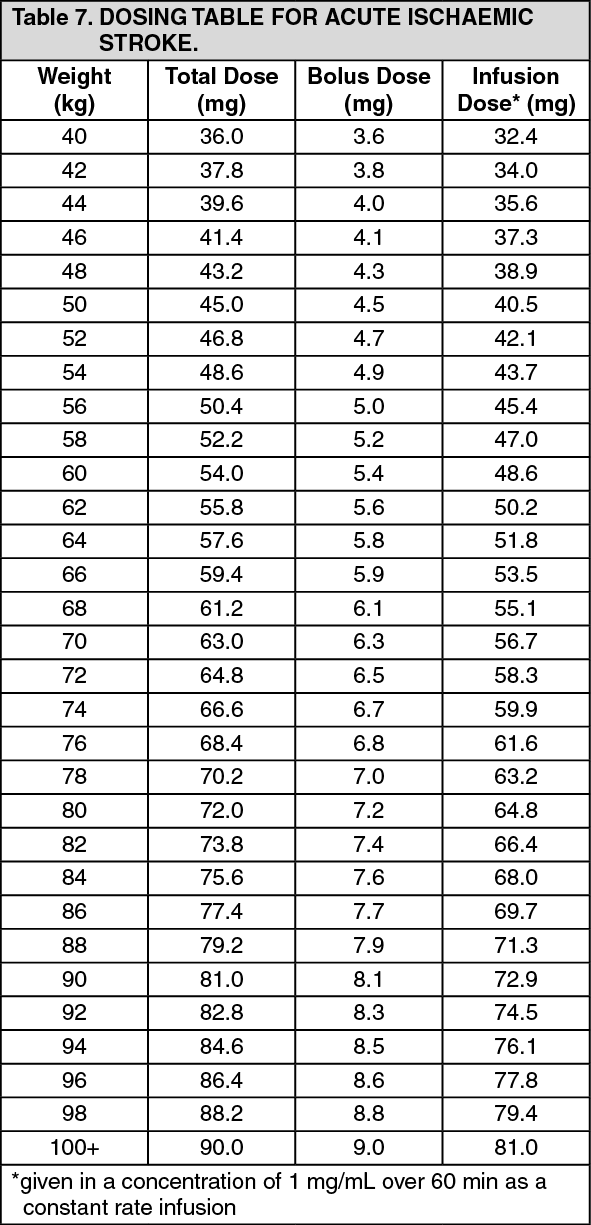 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out