



 Sign Out
Sign Out
Studies on drug interactions with rosuvastatin/ezetimibe combination with other drugs have not been performed, but studies on rosuvastatin and ezetimibe individual drugs were performed as follows.
Rosuvastatin: Effect of co-administered medicinal products on rosuvastatin: Results from in vitro and in vivo studies, show that rosuvastatin does not interact clinically with cytochrome P450 (does not act as a substrate, inhibitor or inducing agent).
Rosuvastatin is a substrate for certain transporter proteins including the hepatic uptake transporter OATP1B1 and efflux transporter BCRP. Concomitant administration of Crestor with inhibitors of these transporter proteins may result in increased rosuvastatin plasma concentrations and an increased risk of myopathy. (See Table 5.)
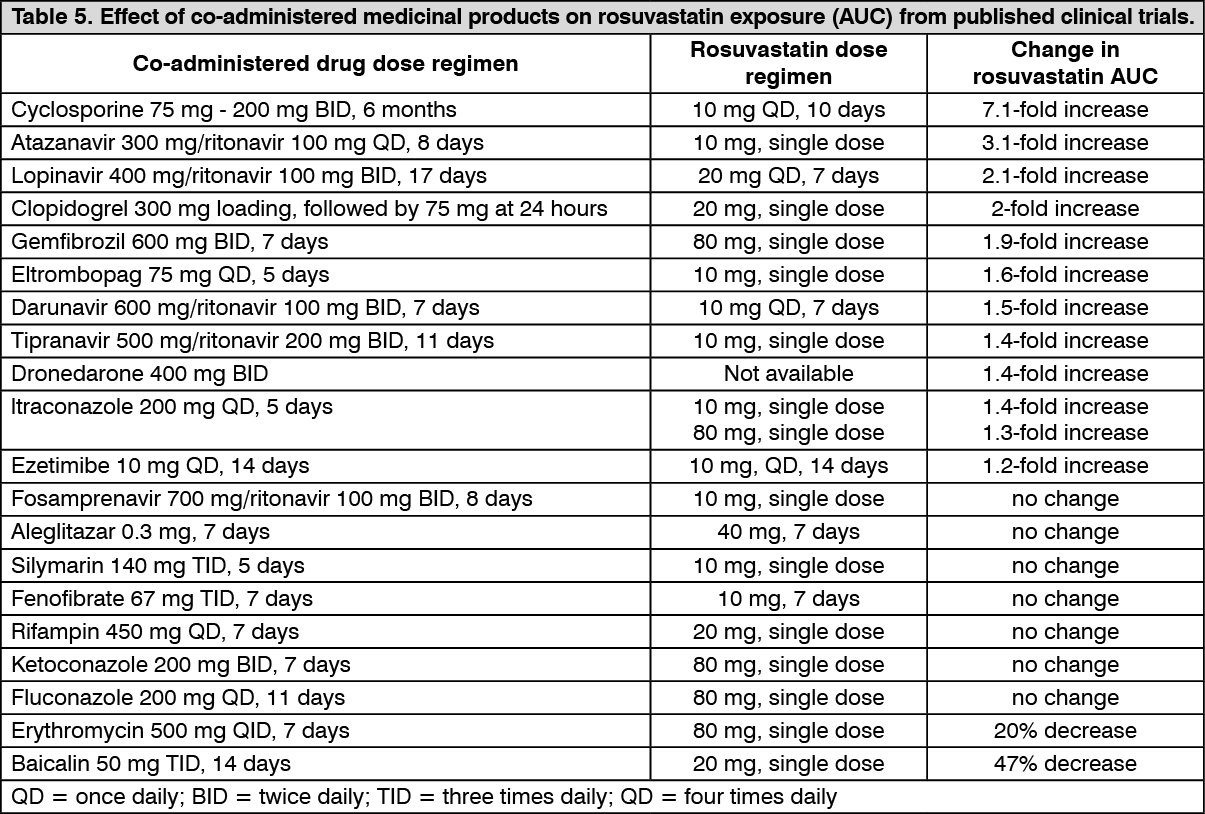 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageEffect of other medicinal products: Antacid: The simultaneous dosing of rosuvastatin with an antacid suspension containing aluminium and magnesium hydroxide resulted in a decrease in rosuvastatin plasma concentration of approximately 50%. This effect was mitigated when the antacid was dosed 2 hours after rosuvastatin. The clinical relevance of this interaction has not been studied.
Fusidic acid: Interaction studies with rosuvastatin and fusidic acid has not been studied.
From post-marketing experience, myopathy including rhabdomyolysis has been reported in the concomitant administration of fusidic acid with rosuvastatin as with other statins. Therefore, the combination of rosuvastatin and fusidic acid is not recommended. If possible, temporary discontinuation of rosuvastatin is recommended throughout the duration of the fusidic acid treatment, should be closely monitored if the treatment is unavoidable.
Effect of rosuvastatin on co-administered medicinal products: Warfarin: When used in combination with rosuvastatin, Warfarin is not significantly affected by pharmacokinetics. As with other statins, the combination use with rosuvastatin and warfarin may increase INR. In the initiation of treatment, discontinuation or dosage-titration of rosuvastatin in patients treated concomitantly with vitamin K antagonists (e.g. warfarin), monitoring of INR is recommended.
Cyclosporine: Co-administration of rosuvastatin and cyclosporine did not affect plasma concentrations of cyclosporine.
Fenofibrate/Fibric acid derivatives: Pharmacokinetic relevant interaction with fenofibrate and rosuvastatin was not observed, however a pharmacodynamic interaction may occur.
Gemfibrozil, fenofibrate, other fibrates and lipid lowering doses (≥1 g/day) of nicotinic acid increase the risk of myopathy when given concomitantly with a statin, probably because they can produce myopathy when given alone.
The 40 mg dose is contraindicated with concomitant use of a fibrate. These patients should also start with the 5 mg dose.
Oral contraceptives: Concomitant use of rosuvastatin and an oral contraceptive resulted in an increase in ethinyl oestradiol and norgestrel AUC of 26% and 34%, respectively. These increased plasma levels should be considered when selecting oral contraceptive doses. There are no pharmacokinetic data available in subjects taking concomitant rosuvastatin and HRT and therefore a similar effect cannot be excluded. However, the combination has been extensively used in women in clinical trials and was well tolerated.
Others: No clinically relevant interaction with digoxin or ezetimibe has been shown.
Ezetimibe: Cholestyramine: Concomitant cholestyramine administration decreased the mean AUC of total ezetimibe (ezetimibe + ezetimibe glucuronide) approximately 55%. The incremental low-density lipoprotein cholesterol (LDL-C) reduction due to adding ezetimibe to cholestyramine may be lessened by this interaction.
Fibrates: Safety and have been evaluated in clinical trial evaluated the safety and efficacy of concomitant fenofibrate administration. Co-administration of ezetimibe with other fibrates has not been studied. Fibrates may increase cholesterol excretion into the bile, leading to cholelithiasis. In pre-clinical studies in dogs, ezetimibe increased cholesterol in the gallbladder bile. Although the preclinical results and their relevance to humans are not known, concomitant fibrates administration (except fenofibrate) is not recommended until results of the study in patients come out.
Gemfibrozil: Concomitant gemfibrozil administration increased the total ezetimibe concentration approximately 1.7-fold, but was not clinically significant. No clinical data are available yet.
Fenofibrate: If cholelithiasis is suspected in a patient receiving ezetimibe and fenofibrate, gallbladder investigations are indicated and other lipid-lowering treatments should be considered. Concomitant fenofibrate administration increased total ezetimibe concentrations approximately 1.5-fold in a pharmacokinetic study.
Statins: No clinically significant pharmacokinetic interactions are seen when ezetimibe was co-administered with atorvastatin, simvastatin, pravastatin, lovastatin, fluvastatin, or rosuvastatin.
Cyclosporine: Caution should be exercised when using ezetimibe and cyclosporine concomitantly and cyclosporine concentrations should be monitored in patients receiving ezetimibe and cyclosporine. In the study of eight post-renal transplant patients with mild renal impairment or normal renal function (creatinine clearance of > 50 mL/min) on a stable dose of cyclosporine, the concomitant use with ezetimibe resulted in a 3.4-fold (range 2.3- to 7.9-fold) increase in the mean AUC and 3.9-fold (range 3.0- to 4.4-fold) increase in the mean Cmax respectively for total ezetimibe compared to a healthy control group (n=17). In a different study, a renal transplant patient with severe renal impairment (creatinine clearance of 13.2 mL/min/1.73 m2) who was receiving cyclosporine and multiple other medications demonstrated a 12-fold greater exposure to total ezetimibe compared to concurrent controls receiving ezetimibe alone. In a two-period crossover study in twelve healthy subjects, daily administration of 20 mg ezetimibe for 8 days with a single 100-mg dose of cyclosporine on Day 7 resulted in a mean 15% increase in cyclosporine AUC (range 10% decrease to 51% increase) compared to a single 100-mg dose of cyclosporine alone.
Anticoagulants: If ezetimibe is added to warfarin, another coumarin anticoagulant, or fluindione, Prothrombin time (INR) should be appropriately monitored. Concomitant administration of ezetimibe (10 mg once daily) had no significant effect on bioavailability of warfarin and prothrombin time in a study of twelve healthy adults. However, there have been post-marketing reports of increased International Normalised Ratio (INR) in patients who had ezetimibe added to warfarin or fluindione. Most of these patients were taking other drug together.