



 Sign Out
Sign Out



Pre/perimenopausal women and men treated with the combination of Abemaciclib (Yulareb) plus an aromatase inhibitor should be treated with a gonadotropin-releasing hormone agonist according to current clinical practice standards.
Pre/perimenopausal women treated with the combination of Abemaciclib (Yulareb) plus fulvestrant should be treated with a gonadotropin-releasing hormone agonist according to current clinical practice standards.
When used as monotherapy, the recommended dose of Abemaciclib (Yulareb) is 200 mg taken orally twice daily.
For early breast cancer, Abemaciclib (Yulareb) should be taken continuously for two years, or until disease recurrence or unacceptable toxicity occurs.
For advanced or metastatic breast cancer, continue treatment until disease progression or unacceptable toxicity.
Abemaciclib (Yulareb) may be taken with or without food [see Pharmacology under Actions].
Instruct patients to take their doses of Abemaciclib (Yulareb) at approximately the same times every day.
If the patient vomits or misses a dose of Abemaciclib (Yulareb), instruct the patient to take the next dose at its scheduled time. Instruct patients to swallow Abemaciclib (Yulareb) tablets whole and not to chew, crush, or split tablets before swallowing. Instruct patients not to ingest Abemaciclib (Yulareb) tablets if broken, cracked, or otherwise not intact.
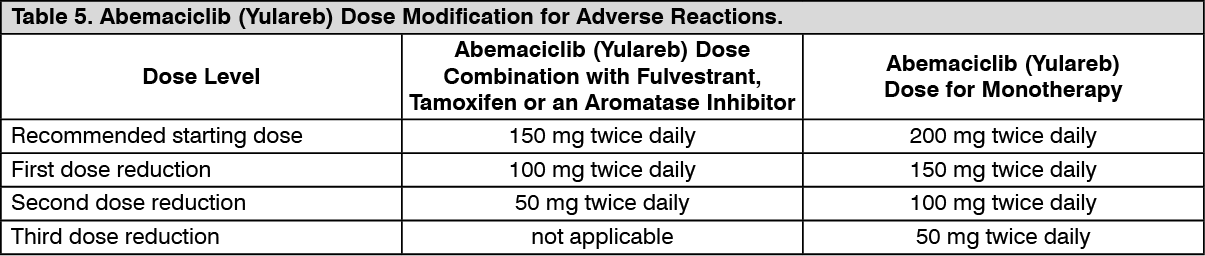
Dose Modification: Dose Modifications for Adverse Reactions: The recommended Abemaciclib (Yulareb) dose modifications for adverse reactions are provided in Tables 5-11. Discontinue Abemaciclib (Yulareb) for patients unable to tolerate 50 mg twice daily. (See Tables 5, 6, 7, 8, 9, 10 and 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image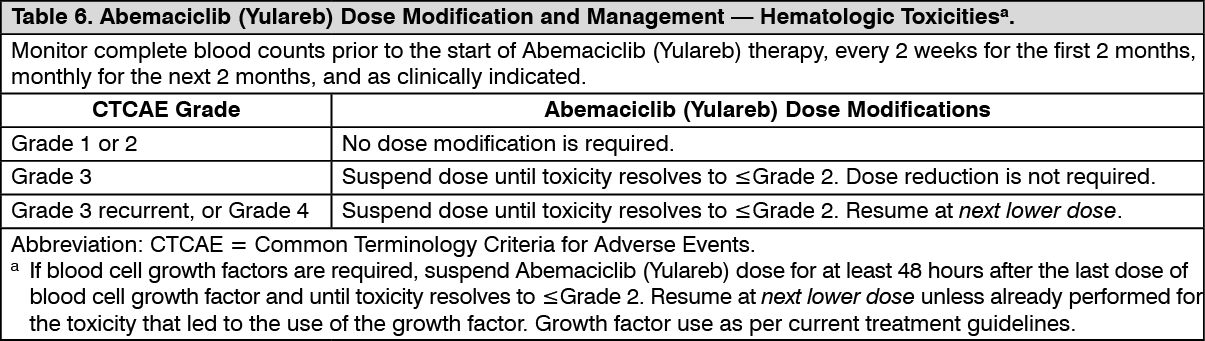 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image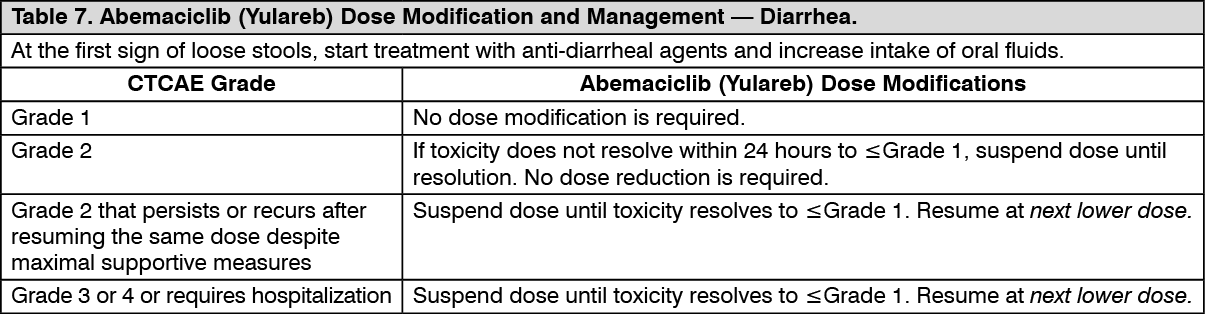 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image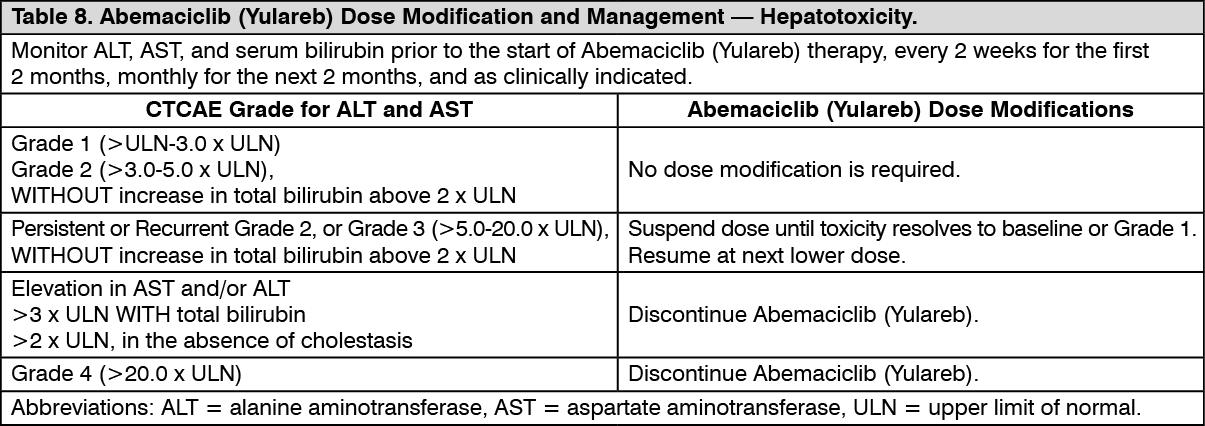 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image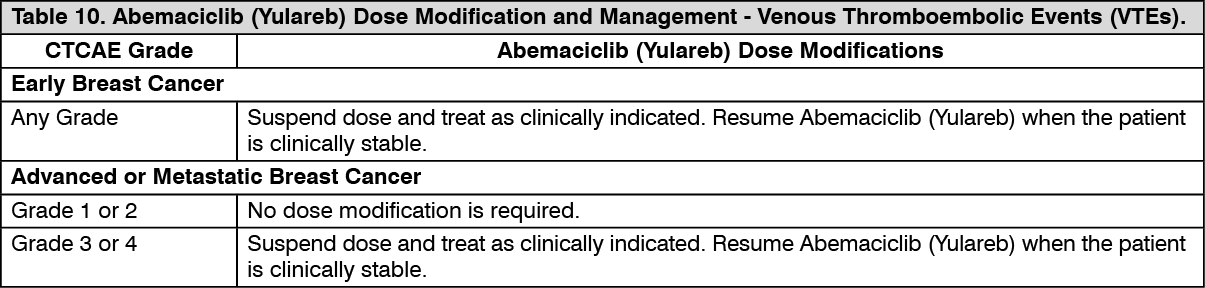 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image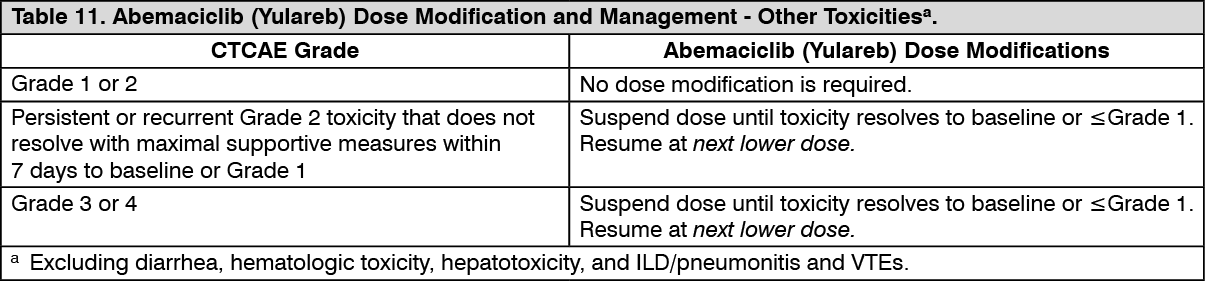 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRefer to the Full Prescribing Information for coadministered fulvestrant, tamoxifen, or an aromatase inhibitor for dose modifications and other relevant safety information.
Dose Modification for Use with Strong and Moderate CYP3A Inhibitors: Avoid concomitant use of the strong CYP3A inhibitor ketoconazole.
With concomitant use of strong CYP3A inhibitors other than ketoconazole, in patients with recommended starting doses of 200 mg twice daily or 150 mg twice daily, reduce the Abemaciclib (Yulareb) dose to 100 mg twice daily. In patients who have had a dose reduction to 100 mg twice daily due to adverse reactions, further reduce the Abemaciclib (Yulareb) dose to 50 mg twice daily. If a patient taking Abemaciclib (Yulareb) discontinues a CYP3A inhibitor, increase the Abemaciclib (Yulareb) dose (after 3-5 half-lives of the inhibitor) to the dose that was used before starting the strong inhibitor [see Interactions and Pharmacology under Actions].
With concomitant use of moderate CYP3A inhibitors, monitor for adverse reactions and consider reducing the Abemaciclib (Yulareb) dose in 50 mg decrements as demonstrated in Table 5, if necessary.
Dose Modification for Patients with Severe Hepatic Impairment: For patients with severe hepatic impairment (Child Pugh-C), reduce the Abemaciclib (Yulareb) dosing frequency to once daily [see Hepatic Impairment under Precautions and Pharmacology under Actions].
Refer to the Full Prescribing Information for coadministered fulvestrant, tamoxifen, or aromatase inhibitor for dose modification requirements for severe hepatic impairment.