Ceftriaxone is administered as a sodium salt by intravenous infusion or as deep intramuscular injections in the treatment of various susceptible infections that include chancroid, gastro-enteritis (invasive salmonellosis, shigellosis) gonorrhea, lyme disease, meningitis, septicaemia, surgical infection (prophylaxis), syphilis, typhoid fever and Whipple's disease among others.
Adults: The usual adult daily dose is 1 to 2 grams given once a day (or in equally divided doses twice a day) depending on the type and severity of infection. The total daily dose should not exceed 4 grams. For preoperative use (surgical prophylaxis), a single dose of 1 gram administered intravenously ½ to 2 hours before surgery is recommended.
A single intramuscular dose of 250 mg is recommended for the treatment of gonorrhea in adults. For surgical infection prophylaxis in adults, a single dose of 1 gm is administered 0.5 to 2 hours prior to surgery. A reduction in dosage may be necessary in patients with severe renal failure and in both with renal and hepatic function; plasma concentrations should be monitored in such patients.
Pediatric Patients: For the treatment of skin and skin structure infections, the recommended total daily dose is 50 to 75 mg/kg given once a day (or in equally divided doses twice a day). The total daily doses should not exceed 2 grams. For the treatment of acute bacterial otitis media, a single intramuscular dose of 50 mg/kg (not to exceed 1 gram) is recommended. For the treatment of serious miscellaneous infections other than meningitis, the recommended total daily dose is 50 to 75 mg/kg, given in divided doses every 12 hours. The total daily dose should not exceed 2 grams.
In the treatment of meningitis, it is recommended that the initial therapeutic dose be 100 mg/kg (not to exceed 4 grams). Thereafter, a total daily dose of 100 mg/kg/day (not to exceed 4 grams daily) is recommended. The daily dose may be administered once a day (or in equally divided doses every 12 hours). The usual duration of therapy is 7 to 14 days.
Generally, Ceftriaxone therapy should be continued for at least 2 days after the signs and symptoms of infection have disappeared. The usual duration of therapy is 4 to 14 days; in complicated infections, longer therapy may be required.
In the elderly the dosage does not require modification provided that renal and hepatic functions are satisfactory. If creatinine clearance is less than 10 mL/min, the daily dose must not exceed 2 gm. In patients with liver damage dose reductions is not required if renal functions are required. In severe renal impairment with hepatic insufficiency the plasma concentration of ceftriaxone should be measured regularly it is in excess of the MIC of the causative organism, and the dosage of ceftriaxone adjusted to prevent accumulation.
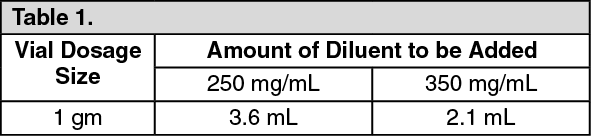
Directions for Use: Intramuscular Administration: Reconstitute Ceftriaxone powder with the appropriate diluent (Sterile water for injection) (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
After reconstitution, each 1 mL of solution contains approximately 250 mg or 350 mg equivalent of ceftriaxone according to the amount of diluent indicated as follows. If required, more dilute solutions could be utilized.
A 350 mg/mL concentration is not recommended for the 250 mg vial since it may not be possible to withdraw the entire contents. As with all intramuscular preparations, Ceftriaxone should be injected well within the body of a relatively large muscle; aspiration helps to avoid unintentional injection into a blood vessel.
Intravenous Administration: Ceftriaxone should be administered intravenously by infusion over a period of 30 minutes. Concentrations between 10 mg/mL and 40 mg/mL are recommended; however, lower concentrations may be used if desired. Reconstitute vials with an appropriate IV diluents. (See Table 2.)
Click on icon to see table/diagram/image
After reconstitution, each 1 mL solution contains approximately 100 mg equivalent of ceftriaxone. Withdraw entire contents and dilute to the desired concentration with the appropriate IV diluent.
Compatibility of Reconstituted Solution: Ceftriaxone sterile powder should be stored at temperatures not exceeding 30°C and protected from light. After reconstitution, protection from normal light is not necessary. The color of solutions ranges from light yellow to amber, depending on the length of storage, concentration and diluents used.
Ceftriaxone solutions remain stable (loss of potency less than 10%) for the following time periods: (See Table 3.)
Click on icon to see table/diagram/image
Frozen solutions should be thawed at room temperature before use. After thawing, unused portions should be discarded. Do not refreeze.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image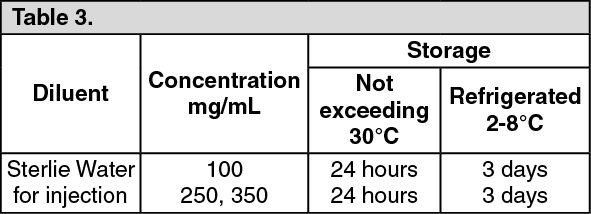 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out