Film-coated tablet: Moxifloxacin is usually well tolerated. Most adverse reactions are mild to moderate. The most common adverse reactions are nausea and diarrhea.
Infection and infestations: Common: Myotic superinfections.
Blood and Lymphatic system disorders: Uncommon: Anemia, Leukopenia, Neutropenia, Thrombocytopenia, Thrombocytothemia, Prothrombin time prolonged/INR increased.
Rare: Thromboplastin level abnormal.
Very rare: Prothrombin level increased/INR decreased, Prothrombin level/INR abnormal.
Immune system disorders: Uncommon: Allergic reaction, Pruritus, Rash, Urticaria, Blood eosinophilia.
Rare: Anaphylactic/anaphylactoid reaction, Allergic edema/angioedema.
Very rare: Anaphylactic/anaphylactoid shock.
Metabolism and nutrition disorders: Uncommon: Hyperlipidemia.
Rare: Hyperglycemia, Hyperuricemia.
Very rare: Hypoglycemia.
Psychiatric disorders: Uncommon: Anxiety reactions, Psychomotor hyperactivity/agitation.
Rare: Emotional liability, Depression, Hallucinations.
Very rare: Depersonalization, Psychotic reactions.
Nervous system disorders: Common: Headache, Dizziness.
Uncommon: Paresthesia and dysesthesia taste disorders (including ageusia in very rare cases), Confusion and disorientation, Sleep disorders, Tremor, Vertigo, Somnolence.
Rare: Hypoesthesia, Smell disorders (including anosmia), Abnormal dreams, Disturbed coordination (including gait disturbances, especially due to dizziness or vertigo; in very rare cases leading to fall with injuries, especially in elderly), Seizures of various clinical manifestations (including grand malconvulsions), Disturbed attention, Speech disorders, Amnesia, Peripheral neuropathy and polyneuropathy.
Very rare: Hyperesthesia.
Eye disorders: Uncommon: Visual disturbances (especially in the course of CNS reactions).
Very rare: Transient loss of vision (especially in the course of CNS reactions).
Ear and Labyrinth disorders: Rare: Tinnitus, Hearing impairment including deafness (usually reversible).
Cardiovascular system disorders: Common: QT prolongation in patients with hypokalaemia.
Uncommon: QT prolongation, Palpitations, Tachycardia, Vasodilation.
Rare: Ventricular tachyarrythmias, Syncope, Hypertension, Hypotension.
Very rare: Unspecified arrhythmias, Torsades de Pointes, Cardiac arrest (especially in patients with severe underlying proarrythmic conditions such as clinically significant bradycardia, acute myocardial ischemia).
Respiratory, thoracic, and mediastinal disorders: Uncommon: Dyspnea (including asthmatic conditions).
Gastrointestinal disorders: Common: Nausea, Vomiting, Gastrointestinal and abdominal pains, Diarrhea.
Uncommon: Decreased appetite and food intake, Constipation, Dyspepsia, Flatulence, Gastroenteritis (excluding erosive gastroenteritis), Increased amylase.
Rare: Dysphagia, Stomatitis, Antibiotic associated colitis.
Hepato-biliary disorders: Common: Increase in transaminases.
Uncommon: Hepatic impairment (including LDH increase), Increased bilirubin, Increase gamma-glutamyl-transferase, Increase in blood alkaline phosphatase.
Rare: Jaundice, Hepatitis (predominantly cholestatic).
Very rare: Fulminant hepatitis.
Skin and subcutaneous tissue disorders: Very rare: Bullous skin reactions like Stevens Johnson Syndrome or Toxic Epidermal Necrolysis.
Musculoskeletal, connective tissue and bone disorders: Uncommon: Arthralgia, Myalgia.
Rare: Tendonitis, Increased muscle tone and cramping, Muscular weakness.
Very rare: Tendon rupture, Arthritis, Gait disturbances (caused by muscular, tendon, or joint symptoms), Exacerbation of symptoms of myasthenia gravis.
Renal and urinary disorders: Uncommon: Dehydration (caused by diarrhea or reduced fluid intake).
Rare: Renal impairment, Renal failure (due to dehydration especially in elderly with pre-existing renal disorders).
General disorders and administration site conditions: Uncommon: Feeling unwell, Unspecific pain and sweating.
Rare: Edema.
Solution for injection: Following are the adverse effects reported with moxifloxacin.
Common: Mycotic superinfections, headache, dizziness, QT prolongation in patients with hypokalemia, nausea, vomiting, gastrointestinal and abdominal pains, diarrhea, increase in transaminases, injection and infusion site reactions.
Uncommon: Anemia, leukopenia, neutropenia, thrombocytopenia, thrombocythemia, prothrombin time prolonged/INR increased, allergic reaction, pruritus, rash, urticaria, blood eosinophilia, hyperlipidemia, anxiety reactions, psychomotor hyperactivity/agitation, par- and dysesthesia, taste disorders (incl. ageusia in very rare cases), confusion and disorientation, sleep disorders, tremor, vertigo, somnolence, visual disturbances (esp in the course of CNS reactions), QT prolongation, palpitations tachycardia, vasodilatation, dyspnea (including asthmatic conditions), anorexia, constipation, dyspepsia, flatulence, gastroenteritis (excl. erosive gastroenteritis), increased amylase, hepatic impairment (incl. LDH increase), increased bilirubin, increased gamma-glutamyl-transferase, increase in blood alkaline phosphatase, arthralgia, myalgia, dehydration (caused by diarrhea or reduced fluid intake), feeling unwell, unspecific pain, sweating, infusion site (thrombo-) phlebitis.
Rare: Thromboplastin level abnormal, anaphylactic/anaphylactoid reaction, allergic edema/angioedema (incl. laryngeal edema, potentially life threatening), hyperglycemia, hyperuricemia, emotional lability, depression (in very rare cases potentially culminating in self-endangering behaviour), hallucinations, hypoesthesia, smell disorders (incl. anosmia), abnormal dreams, disturbed coordination (incl. gait disturbances, esp. due to dizziness or vertigo; in very rare cases leading to fall with injuries, esp. in elderly) seizures of various clinical manifestations (incl. grand mal convulsions), disturbed attention, speech disorders, amnesia, tinnitus, ventricular tachyarrhythmias, syncope, hypertension, hypotension, dysphagia, stomatitis, antibiotic associated colitis (in very rare cases associated with life threatening complications), jaundice, hepatitis (predominantly cholestatic), tendonitis, increased muscle tone and cramping, renal impairment, renal failure (due to dehydration esp. in elderly with pre-existing renal disorders), edema.
Very Rare: Prothrombin level increased/INR decreased, prothrombin level/INR abnormal, anaphylactic/anaphylactoid shock (potentially life threatening), psychiatric disorders, depersonalization, psychotic reactions (potentially culminating in self-endangering behaviour), hyperesthesia, unspecified arrhythmias, torsade de Pointes, cardiac arrest (especially in patients with severe underlying proarrhythmic conditions such as clinically significant bradycardia, acute myocardial ischemia), fulminant hepatitis potentially leading to life-threatening liver failure (including fatal cases), bullous skin reactions like Stevens-Johnson-Syndrome or toxic epidermal necrolysis (potentially life threatening), tendon rupture, arthritis gait disturbance (caused by muscular, tendon or joint symptoms) exacerbation of symptoms of myasthenia gravis.



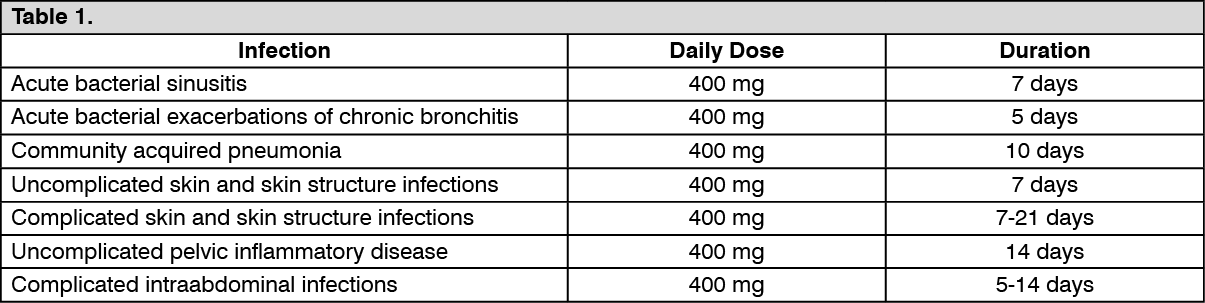 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image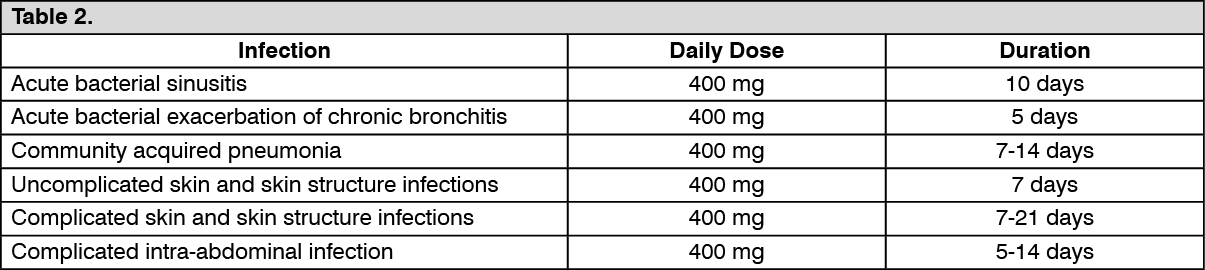 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out