VALDON is a film-coated tablet that contains 75 mg of Clopidogrel for oral administration.
Each film-coated tablet contains: Clopidogrel (as bisulfate) 75 mg.
Antithrombotic Agent (Platelet Aggregation Inhibitor).
Pharmacology: Pharmacodynamics: Mechanism of action: Clopidogrel is a prodrug, one of whose metabolites is an inhibitor of platelet aggregation. Clopidogrel must be metabolized by CYP450 enzymes to produce the active metabolite that inhibits platelet aggregation. The active metabolite of clopidogrel selectively inhibits the binding of adenosine diphosphate (ADP) to its platelet P2Y12 receptor and the subsequent ADP-mediated activation of the glycoprotein GPIIb/IIIa complex, thereby inhibiting platelet aggregation. Due to the irreversible binding, platelets exposed are affected for the remainder of their lifespan (approximately 7-10 days) and recovery of normal platelet function occurs at a rate consistent with platelet turnover. Platelet aggregation induced by agonists other than ADP is also inhibited by blocking the amplification of platelet activation by released ADP.
Because the active metabolite is formed by CYP450 enzymes, some of which are polymorphic or subject to inhibition by other medicinal products, not all patients will have adequate platelet inhibition.
Pharmacokinetics: Absorption: After single and repeated oral doses of 75 mg per day, clopidogrel is rapidly absorbed. Mean peak plasma levels of unchanged clopidogrel (approximately 2.2-2.5 ng/mL after a single 75 mg oral dose) occurred approximately 45 minutes after dosing. Absorption is at least 50%, based on urinary excretion of clopidogrel metabolites.
Distribution: Clopidogrel and the main circulating (inactive) metabolite bind reversibly in vitro to human plasma proteins (98% and 94% respectively). The binding is non-saturable in vitro over a wide concentration range.
Biotransformation: Clopidogrel is extensively metabolized by the liver. In vitro and in vivo, clopidogrel is metabolized according to two main metabolic pathways: one mediated by esterases and leading to hydrolysis into its inactive carboxylic acid derivative (85% of circulating metabolites), and one mediated by multiple cytochromes P450. Clopidogrel is first metabolized to a 2-oxo-clopidogrel intermediate metabolite. Subsequent metabolism of the 2-oxo-clopidogrel intermediate metabolite results in formation of the active metabolite, a thiol derivative of clopidogrel. The active metabolite is formed mostly by CYP2C19 with contributions from several other CYP enzymes, including CYP1A2, CYP2B6 and CYP3A4. The active thiol metabolite which has been isolated in vitro, binds rapidly and irreversibly to platelet receptors, thus inhibiting platelet aggregation.
The Cmax of the active metabolite is twice as high following a single 300 mg clopidogrel loading dose as it is after four days of 75 mg maintenance dose. Cmax occurs approximately 30 to 60 minutes after dosing.
Elimination: Following an oral dose of 14C-labelled clopidogrel in man, approximately 50% was excreted in the urine and approximately 46% in the feces in the 120 hr interval after dosing. After a single oral dose of 75 mg, clopidogrel has a half-life of approximately 6 hours. The elimination half-life of the main circulating (inactive) metabolite was 8 hours after single and repeated administration.
Secondary prevention of atherothrombotic events: Clopidogrel is indicated in: Adult patients suffering from myocardial infarction (from a few days until less than 35 days), ischemic stroke (from 7 days until less than 6 months) or established peripheral arterial disease.
Adult patients suffering from acute coronary syndrome: Non-ST segment elevation acute coronary syndrome (unstable angina or non-Q-wave myocardial infarction), including patients undergoing a stent placement following percutaneous coronary intervention, in combination with acetylsalicylic acid (ASA); ST segment elevation acute myocardial infarction, in combination with ASA in medically treated patients eligible for thrombolytic therapy.
In patients with moderate to high-risk Transient Ischemic Attack (TIA) or minor Ischemic Stroke (IS).
Clopidogrel in combination with ASA is indicated in: Adult patients with moderate to high-risk TIA (ABCD2 score ≥4) or minor IS (NIHSS ≤3) within 24 hours of either the TIA or IS event.
Prevention of atherothrombotic and thromboembolic events in atrial fibrillation: In adult patients with atrial fibrillation who have at least one risk factor for vascular events, are not suitable for treatment with Vitamin K antagonists (VKA) and who have a low bleeding risk, clopidogrel is indicated in combination with ASA for the prevention of atherothrombotic and thromboembolic events, including stroke.
Posology: Adults and elderly: Clopidogrel should be given as a single daily dose of 75 mg.
In patients suffering from acute coronary syndrome: Non-ST segment elevation acute coronary syndrome (unstable angina or non-Q-wave myocardial infarction): clopidogrel treatment should be initiated with a single 300 mg or 600 mg loading dose. A 600 mg loading dose may be considered in patients <75 years of age when percutaneous coronary intervention is intended. Clopidogrel treatment should be continued at 75 mg once a day (with acetylsalicylic acid (ASA) 75 mg-325 mg daily). Since higher doses of ASA were associated with higher bleeding risk it is recommended that the dose of ASA should not be higher than 100 mg. The optimal duration of treatment has not been formally established. Clinical trial data support uses up to 12 months, and the maximum benefit was seen at 3 months.
ST segment elevation acute myocardial infarction: clopidogrel should be given as a single daily dose of 75 mg initiated with a 300 mg loading dose in combination with ASA and with or without thrombolytics. For medically treated patients over 75 years of age clopidogrel should be initiated without a loading dose. Combined therapy should be started as early as possible after symptoms start and continued for at least four weeks. The benefit of the combination of clopidogrel with ASA beyond four weeks has not been studied in this setting.
Adult patients with moderate to high-risk TIA or minor IS: Adult patients with moderate to high-risk TIA (ABCD2 score ≥4) or minor IS (NIHSS ≤3) should be given a loading dose of clopidogrel 300 mg followed by clopidogrel 75 mg once daily and ASA (75 mg-100 mg once daily). Treatment with clopidogrel and ASA should be started within 24 hours of the event and be continued 21 days followed by single antiplatelet therapy.
In patients with atrial fibrillation, clopidogrel should be given as a single daily dose of 75 mg. ASA (75-100 mg daily) should be initiated and continued in combination with clopidogrel.
If a dose is missed: Within less than 12 hours after regular scheduled time: patients should take the dose immediately and then take the next dose at the regular scheduled time.
For more than 12 hours: patients should take the next dose at the regular scheduled time and should not double the dose.
Pediatric population: Clopidogrel should not be used in children because of efficacy concerns.
Renal impairment: Therapeutic experience is limited in patients with renal impairment.
Hepatic impairment: Therapeutic experience is limited in patients with moderate hepatic disease who may have bleeding diatheses.
Method of administration: For oral use: It may be given with or without food.
Overdose following clopidogrel administration may lead to prolonged bleeding time and subsequent bleeding complications. Appropriate therapy should be considered if bleedings are observed.
No antidote to the pharmacological activity of clopidogrel has been found. If prompt correction of prolonged bleeding time is required, platelet transfusion may reverse the effects of clopidogrel.
Hypersensitivity to the active substance or to any of the excipients.
Severe hepatic impairment.
Active pathological bleeding such as peptic ulcer or intracranial hemorrhage.
The effectiveness of Clopidogrel results from its antiplatelet activity, which is dependent on its conversion to an active metabolite by the cytochrome P450 (CYP) system, principally CYP2C19. Clopidogrel at recommended doses forms less of the active metabolite and so has a reduced effect on platelet activity in patients who are homozygous for nonfunctional alleles of the CYP2C19 gene, (termed "CYP2C19 poor metabolizers"). Tests are available to identify patients who are CYP2C19 poor metabolizers. Consider use of another platelet P2Y12 inhibitor in patients identified as CYP2C19 poor metabolizers.
Bleeding and hematological disorders: Due to the risk of bleeding and hematological adverse reactions, blood cell count determination and/or other appropriate testing should be promptly considered whenever clinical symptoms suggestive of bleeding arise during the course of treatment. As with other antiplatelet agents, clopidogrel should be used with caution in patients who may be at risk of increased bleeding from trauma, surgery or other pathological conditions and in patients receiving treatment with ASA, heparin, glycoprotein IIb/IIIa inhibitors or non-steroidal anti-inflammatory drugs (NSAIDs) including Cox-2 inhibitors, or selective serotonin reuptake inhibitors (SSRIs), or CYP2C19 strong inducers or other medicinal products associated with bleeding risk such as pentoxifylline. Patients should be followed carefully for any signs of bleeding including occult bleeding, especially during the first weeks of treatment and/or after invasive cardiac procedures or surgery. The concomitant administration of clopidogrel with oral anticoagulants is not recommended since it may increase the intensity of bleedings. If a patient is to undergo elective surgery and antiplatelet effect is temporarily not desirable, clopidogrel should be discontinued 7 days prior to surgery. Patients should inform physicians and dentists that they are taking clopidogrel before any surgery is scheduled and before any new medicinal product is taken. Clopidogrel prolongs bleeding time and should be used with caution in patients who have lesions with a propensity to bleed (particularly gastrointestinal and intraocular).
Patients should be told that it might take longer than usual to stop bleeding when they take clopidogrel (alone or in combination with ASA), and that they should report any unusual bleeding (site or duration) to their physician.
The use of clopidogrel 600 mg loading dose is not recommended in patients with non-ST segment elevation acute coronary syndrome and ≥75 years of age due to increased bleeding risk in this population.
Thrombotic Thrombocytopenic Purpura (TTP): Thrombotic Thrombocytopenic Purpura (TTP) has been reported very rarely following the use of clopidogrel, sometimes after a short exposure. It is characterized by thrombocytopenia and microangiopathic hemolytic anemia associated with either neurological findings, renal dysfunction or fever. TTP is a potentially fatal condition requiring prompt treatment including plasmapheresis.
Acquired hemophilia: Acquired hemophilia has been reported following use of clopidogrel. In cases of confirmed isolated activated Partial Thromboplastin Time (aPTT) prolongation with or without bleeding, acquired hemophilia should be considered. Patients with a confirmed diagnosis of acquired hemophilia should be managed and treated by specialists, and clopidogrel should be discontinued.
Recent ischemic stroke: Initiation of therapy: In acute minor IS or moderate to high-risk TIA patients, dual antiplatelet therapy (clopidogrel and ASA) should be started no later than 24 hours after the event onset.
There is no data regarding the benefit-risk of short term dual antiplatelet therapy in acute minor IS or moderate to high-risk TIA patients, with a history of (non-traumatic) intracranial hemorrhage.
In non-minor IS patients, clopidogrel monotherapy should be started only after the first 7 days of the event.
Non-minor IS patients (NIHSS >4): In view of the lack of data, use of dual antiplatelet therapy is not recommended.
Recent minor IS or moderate to high-risk TIA in patients for whom intervention is indicated or planned: There is no data to support the use of dual antiplatelet therapy in patients for whom treatment with carotid endarterectomy or intravascular thrombectomy is indicated, or in patients planned for thrombolysis or anticoagulant therapy. Dual antiplatelet therapy is not recommended in these situations.
Cytochrome P450 2C19 (CYP2C19): Pharmacogenetics: In patients who are poor CYP2C19 metabolizers, clopidogrel at recommended doses forms less of the active metabolite of clopidogrel and has a smaller effect on platelet function. Tests are available to identify a patient's CYP2C19 genotype.
Since clopidogrel is metabolized to its active metabolite partly by CYP2C19, use of medicinal products that inhibit the activity of this enzyme would be expected to result in reduced drug levels of the active metabolite of clopidogrel. The clinical relevance of this interaction is uncertain. As a precaution concomitant use of strong or moderate CYP2C19 inhibitors should be discouraged.
Use of medicinal products that induce the activity of CYP2C19 would be expected to result in increased drug levels of the active metabolite of clopidogrel and might potentiate the bleeding risk. As a precaution concomitant use of strong CYP2C19 inducers should be discouraged.
CYP2C8 substrates: Caution is required in patients treated concomitantly with clopidogrel and CYP2C8 substrate medicinal products.
Cross-reactions among thienopyridines: Patients should be evaluated for history of hypersensitivity to thienopyridines (such as clopidogrel, ticlopidine, prasugrel) since cross-reactivity among thienopyridines has been reported. Thienopyridines may cause mild to severe allergic reactions such as rash, angioedema, or hematological cross-reactions such as thrombocytopenia and neutropenia. Patients who had developed a previous allergic reaction and/or hematological reaction to one thienopyridine may have an increased risk of developing the same or another reaction to another thienopyridine. Monitoring for signs of hypersensitivity in patients with a known allergy to thienopyridines is advised.
Renal impairment: Therapeutic experience with clopidogrel is limited in patients with renal impairment. Therefore, clopidogrel should be used with caution in these patients.
Hepatic impairment: Experience is limited in patients with moderate hepatic disease who may have bleeding diatheses. Clopidogrel should therefore be used with caution in this population.
Excipients: Clopidogrel contains lactose. Patients with rare hereditary problems of galactose intolerance, total lactase deficiency or glucose-galactose malabsorption should not take this medicine.
This medicinal product contains hydrogenated castor oil which may cause stomach upset and diarrhea.
Pregnancy: As no clinical data on exposure to clopidogrel during pregnancy are available, it is preferable not to use clopidogrel during pregnancy as a precautionary measure.
Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/fetal development, parturition or postnatal development.
Lactation: It is unknown whether clopidogrel is excreted in human breast milk. Animal studies have shown excretion of clopidogrel in breast milk. As a precautionary measure, breast-feeding should not be continued during treatment with Clopidogrel.
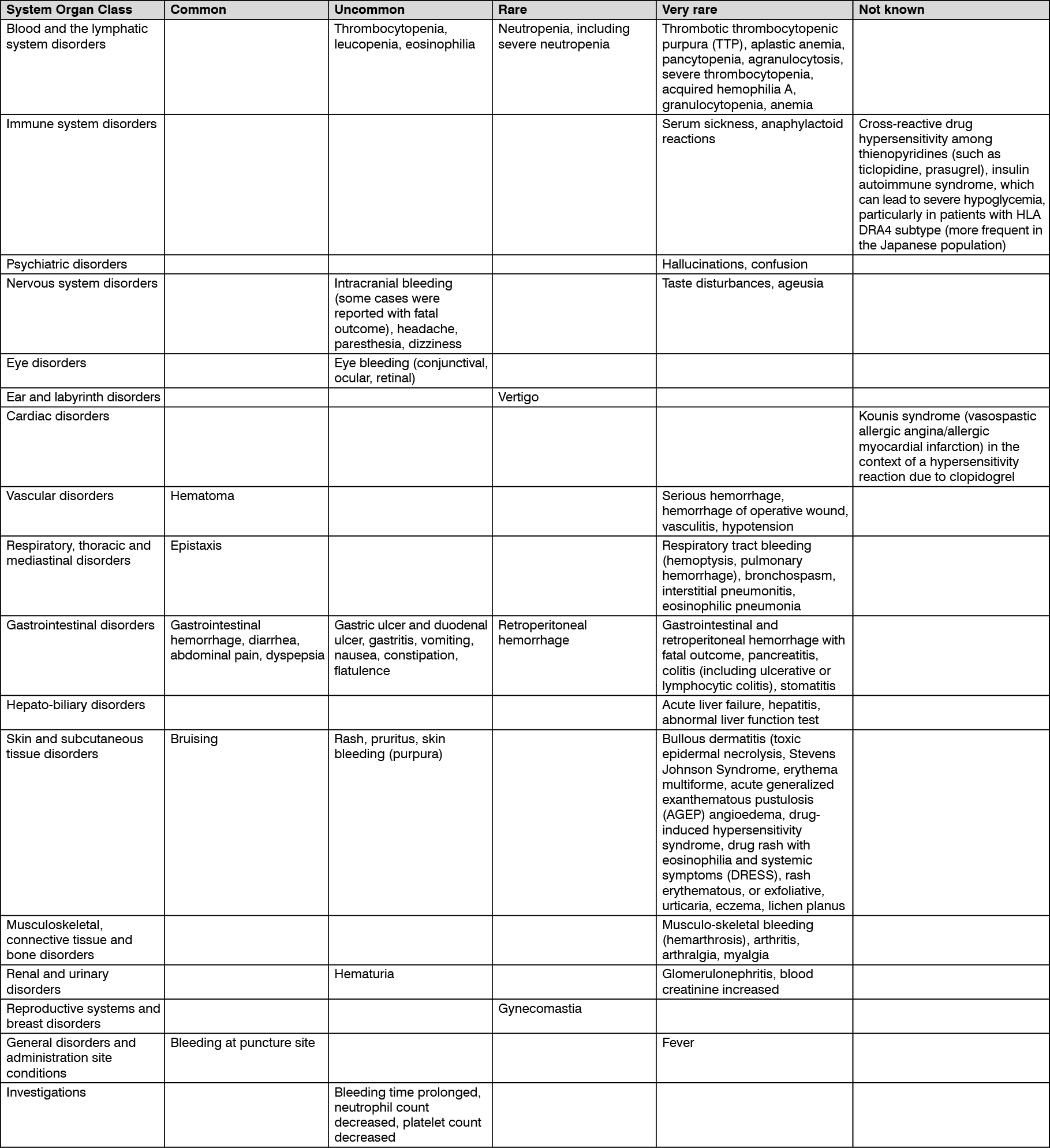
Tabulated list of adverse reactions: Adverse reactions that occurred either during clinical studies or that were spontaneously reported are presented in the table as follows. Their frequency is defined using the following conventions: common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000), not known (cannot be estimated from the available data). Within each system organ class, adverse reactions are presented in order of decreasing seriousness. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Medicinal products associated with bleeding risk: There is an increased risk of bleeding due to the potential additive effect. The concomitant administration of medicinal products associated with bleeding risk should be undertaken with caution.
Oral anticoagulants: The concomitant administration of clopidogrel with oral anticoagulants is not recommended since it may increase the intensity of bleedings. Although the administration of clopidogrel 75 mg/day did not modify the pharmacokinetics of S-warfarin or International Normalized Ratio (INR) in patients receiving long-term warfarin therapy, co-administration of clopidogrel with warfarin increases the risk of bleeding because of independent effects on hemostasis.
Glycoprotein IIb/Illa inhibitors: Clopidogrel should be used with caution in patients who receive concomitant glycoprotein IIb/Illa inhibitors.
Acetylsalicylic acid (ASA): ASA did not modify the clopidogrel-mediated inhibition of ADP-induced platelet aggregation, but clopidogrel potentiated the effect of ASA on collagen-induced platelet aggregation. However, concomitant administration of 500 mg of ASA twice a day for one day did not significantly increase the prolongation of bleeding time induced by clopidogrel intake. A pharmacodynamic interaction between clopidogrel and acetylsalicylic acid is possible, leading to increased risk of bleeding. Therefore, concomitant use should be undertaken with caution. However, clopidogrel and ASA have been administered together for up to one year.
Heparin: In a clinical study conducted in healthy subjects, clopidogrel did not necessitate modification of the heparin dose or alter the effect of heparin on coagulation. Co-administration of heparin had no effect on the inhibition of platelet aggregation induced by clopidogrel. A pharmacodynamic interaction between clopidogrel and heparin is possible, leading to increased risk of bleeding. Therefore, concomitant use should be undertaken with caution.
Thrombolytics: The safety of the concomitant administration of clopidogrel, fibrin or non-fibrin specific thrombolytic agents and heparins was assessed in patients with acute myocardial infarction. The incidence of clinically significant bleeding was similar to that observed when thrombolytic agents and heparin are co-administered with ASA.
NSAIDs: In a clinical study conducted in healthy volunteers, the concomitant administration of clopidogrel and naproxen increased occult gastrointestinal blood loss. However, due to the lack of interaction studies with other NSAIDs, it is presently unclear whether there is an increased risk of gastrointestinal bleeding with all NSAIDs. Consequently, NSAIDs including Cox-2 inhibitors and clopidogrel should be co-administered with caution.
SSRIs: Since SSRIs affect platelet activation and increase the risk of bleeding, the concomitant administration of SSRIs with clopidogrel should be undertaken with caution.
Other concomitant therapy: Inducers of CYP2C19: Since clopidogrel is metabolized to its active metabolite partly by CYP2C19, use of medicinal products that induce the activity of this enzyme would be expected to result in increased drug levels of the active metabolite of clopidogrel.
Rifampicin strongly induces CYP2C19, resulting in both an increased level of clopidogrel active metabolite and platelet inhibition, which in particular might potentiate the risk of bleeding. As a precaution, concomitant use of strong CYP2C19 inducers should be discouraged.
Inhibitors of CYP2C19: Since clopidogrel is metabolized to its active metabolite partly by CYP2C19, use of medicinal products that inhibit the activity of this enzyme would be expected to result in reduced drug levels of the active metabolite of clopidogrel. The clinical relevance of this interaction is uncertain. As a precaution, concomitant use of strong or moderate CYP2C19 inhibitors should be discouraged.
Medicinal products that are strong or moderate CYP2C19 inhibitors include, for example, omeprazole and esomeprazole, fluvoxamine, fluoxetine, moclobemide, voriconazole, fluconazole, ticlopidine, carbamazepine and efavirenz.
Proton Pump Inhibitors (PPI): Omeprazole 80 mg once daily administered either at the same time as clopidogrel or with 12 hours between the administrations of the two drugs decreased the exposure of the active metabolite by 45% (loading dose) and 40% (maintenance dose). The decrease was associated with a 39% (loading dose) and 21% (maintenance dose) reduction of inhibition of platelet aggregation. Esomeprazole is expected to give a similar interaction with clopidogrel.
Inconsistent data on the clinical implications of this pharmacokinetic (PK)/pharmacodynamic (PD) interaction in terms of major cardiovascular events have been reported from both observational and clinical studies. As a precaution, concomitant use of omeprazole or esomeprazole should be discouraged.
Less pronounced reductions of metabolite exposure have been observed with pantoprazole or lansoprazole. The plasma concentrations of the active metabolite were 20% reduced (loading dose) and 14% reduced (maintenance dose) during concomitant treatment with pantoprazole 80 mg once daily. This was associated with a reduction of the mean inhibition of platelet aggregation by 15% and 11%, respectively. These results indicate that clopidogrel can be administered with pantoprazole.
There is no evidence that other medicinal products that reduce stomach acid such as H2 blockers or antacids interfere with antiplatelet activity of clopidogrel.
Boosted anti-retroviral therapy (ART): HIV patients treated with boosted anti-retroviral therapies (ART) are at high risk of vascular events.
A significantly reduced platelet inhibition has been shown in HIV patients treated with ritonavir-or cobicistat-boosted ART. Although the clinical relevance of these findings is uncertain, there have been spontaneous reports of HIV-infected patients treated with ritonavir boosted ART, who have experienced re-occlusive events after de-obstruction or have suffered thrombotic events under a clopidogrel loading treatment schedule. Average platelet inhibition can be decreased with concomitant use of clopidogrel and ritonavir. Therefore, concomitant use of clopidogrel with ART boosted therapies should be discouraged.
Other medicinal products: A number of other clinical studies have been conducted with clopidogrel and other concomitant medicinal products to investigate the potential for pharmacodynamic and pharmacokinetic interactions. No clinically significant pharmacodynamic interactions were observed when clopidogrel was co-administered with atenolol, nifedipine, or both atenolol and nifedipine. Furthermore, the pharmacodynamic activity of clopidogrel was not significantly influenced by the co-administration of phenobarbital or estrogen. The pharmacokinetics of digoxin or theophylline were not modified by the co-administration of clopidogrel. Antacids did not modify the extent of clopidogrel absorption.
Data from the CAPRIE study indicate that phenytoin and tolbutamide which are metabolized by CYP2C9 can be safely co-administered with clopidogrel.
CYP2C8 substrate medicinal products: Clopidogrel has been shown to increase repaglinide exposure in healthy volunteers. In vitro studies have shown the increase in repaglinide exposure is due to inhibition of CYP2C8 by the glucuronide metabolite of clopidogrel. Due to the risk of increased plasma concentrations, concomitant administration of clopidogrel and drugs primarily cleared by CYP2C8 metabolism (e.g., repaglinide, paclitaxel) should be undertaken with caution.
Apart from the specific medicinal product interaction information described above, interaction studies with clopidogrel and some medicinal products commonly administered in patients with atherothrombotic disease have not been performed. However, patients entered into clinical trials with clopidogrel received a variety of concomitant medicinal products including diuretics, beta blockers, ACEI, calcium antagonists, cholesterol lowering agents, coronary vasodilators, antidiabetic agents (including insulin), antiepileptic agents and GPIIb/Illa antagonists without evidence of clinically significant adverse interactions.
As with other oral P2Y12 inhibitors, co-administration of opioid agonists has the potential to delay and reduce the absorption of clopidogrel presumably because of slowed gastric emptying. The clinical relevance is unknown. Consider the use of a parenteral antiplatelet agent in acute coronary syndrome patients requiring co-administration of morphine or other opioid agonists.
Rosuvastatin: Clopidogrel has been shown to increase rosuvastatin exposure in patients by 2-fold (AUC) and 1.3-fold (Cmax) after administration of a 300 mg clopidogrel dose, and by 1.4-fold (AUC) without effect on Cmax after repeated administration of a 75 mg clopidogrel dose.
Store at temperatures not exceeding 30°C.
B01AC04 - clopidogrel ; Belongs to the class of platelet aggregation inhibitors excluding heparin. Used in the treatment of thrombosis.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out