Pharmacotherapeutic Group: Drugs used in diabetes. Insulins and analogs for injection, long-acting.
ATC Code: A10AE06.
Pharmacology: Pharmacodynamics: Mechanism of Action: Insulin degludec binds specifically to the human insulin receptor and results in the same pharmacological effects as human insulin.
The blood glucose-lowering effect of insulin is due to the facilitated uptake of glucose following the binding of insulin to receptors on muscle and fat cells and to the simultaneous inhibition of glucose output from the liver.
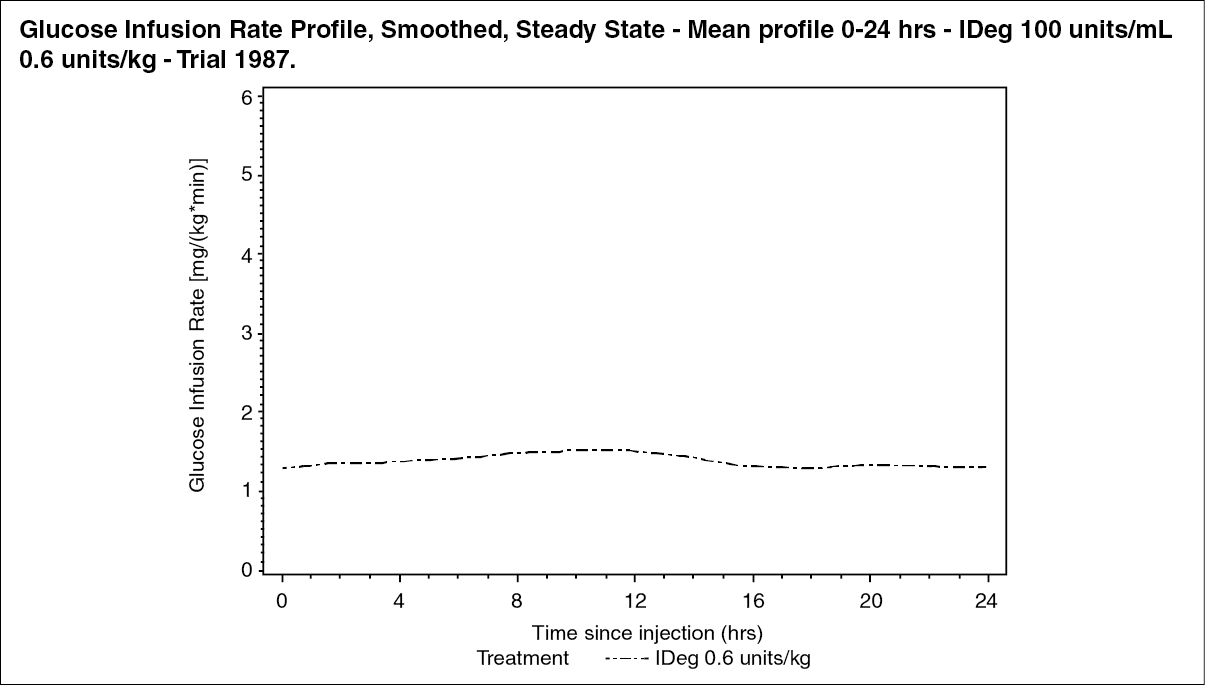
Pharmacodynamic Effects: Insulin degludec is a basal insulin that forms soluble multi-hexamers upon SC injection, resulting in a depot from which insulin degludec is continuously and slowly absorbed into the circulation leading to a flat and stable glucose-lowering effect of insulin degludec (see figure). During a period of 24 hrs with once-daily treatment, the glucose-lowering effect of insulin degludec, in contrast to insulin glargine, was evenly distributed between the 1st and 2nd 12 hrs (AUC
GIR,0-12hr,
SS/AUCG
IR,total,SS=0.5).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The duration of action of insulin degludec is beyond 42 hrs within the therapeutic dose range. Steady state will occur after 2-3 days of dose administration.
The insulin degludec glucose-lowering action at steady state, shows 4 times lower day-to-day variability in terms of Coefficients of Variation (CV) for the glucose-lowering effect during 0-24 hrs (AUC
GIR,τ,SS) and 2-24 hrs (AUC
GIR2-24hr,SS) as compared to insulin glargine, see Table 1.
Click on icon to see table/diagram/image
Total glucose-lowering effect of insulin degludec increases linearly with increasing doses.
There is no clinically relevant difference in the pharmacodynamics of insulin degludec between elderly and younger adult patients.
Clinical Efficacy and Safety: Eleven (11) multinational clinical trials of 26 or 52 weeks' duration were conducted as controlled, open-label, randomized, parallel, treat-to-target trials exposing 4,275 patients to insulin degludec [1,102 in type 1 diabetes mellitus (DM) and 3,173 in type 2 DM].
The effect of insulin degludec was tested in patients with type 1 DM (see Table 3), in insulin naive patients (insulin initiation in type 2 DM, see Table 4) and in previous insulin users (insulin intensification in type 2 DM, see Table 5) with fixed as well as flexible dosing time (see Table 6), and the reduction in HbA
1c from baseline to end of trial was confirmed to be non-inferior in all trials against all comparators (insulin detemir and insulin glargine). While improvements in HbA
1c were non-inferior compared to other insulin products, against sitagliptin insulin degludec was statistically significantly superior in reducing HbA
1c (see Table 5).
In a prospectively planned meta-analysis across 7 treat-to-target confirmatory trials in patients with type 1 and type 2 DM, insulin degludec was superior in terms of a lower number of treatment emergent confirmed hypoglycemic episodes (driven by a benefit in type 2 DM, see Table 2) and nocturnal confirmed hypoglycemic episodes compared to insulin glargine (administered according to label). The reduction in hypoglycemia was achieved at a lower average fasting plasma glucose (FPG) level with insulin degludec than with insulin glargine.
Click on icon to see table/diagram/image
There is no clinically relevant development of insulin antibodies after long-term treatment with insulin degludec.
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Pharmacokinetics: Absorption: After SC injection, soluble and stable multi-hexamers are formed creating a depot of insulin in the SC tissue. Insulin degludec monomers gradually separate from the multi-hexamers thus resulting in a slow and continuous delivery of insulin degludec into the circulation.
Steady state serum concentration is reached after 2-3 days of daily insulin degludec administration.
During a period of 24 hrs with once-daily treatment, the exposure of insulin degludec was evenly distributed between the 1st and 2nd 12 hrs. The ratio between AUC
GIR,0-12hr,SS and AUC
GIR,τ,SS was 0.5.
Distribution: The affinity of insulin degludec to serum albumin corresponds to a plasma protein-binding of >99% in human plasma.
Biotransformation: Degradation of insulin degludec is similar to that of human insulin; all metabolites formed are inactive.
Elimination: The half-life (t
½) after SC administration of insulin degludec is determined by the rate of absorption from the subcutaneous tissue. The t
½ of insulin degludec is approximately 25 hrs independent of dose.
Linearity: Dose proportionality in total exposure is observed after SC administration within the therapeutic dose range.
Gender: There is no gender difference in the pharmacokinetic properties of insulin degludec.
Elderly, Race, Renal and Hepatic Impairment: There is no difference in the pharmacokinetics of insulin degludec between elderly and younger adult patients, between races or between healthy subjects and patients with renal or hepatic impairment.
Pediatric Population: Pharmacokinetic properties of insulin degludec were investigated in children (6-11 years) and adolescents (12-18 years), and were comparable to those observed in adults with type 1 DM. Total exposure after a single dose is however, higher in children and adolescents than in adults with type 1 DM.
Toxicology: Preclinical Safety Data: Nonclinical data reveal no safety concerns for humans based on studies of safety pharmacology, repeated dose toxicity, carcinogenic potential and toxicity to reproduction.
The ratio of mitogenic relative to metabolic potency for insulin degludec is comparable to that of human insulin.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image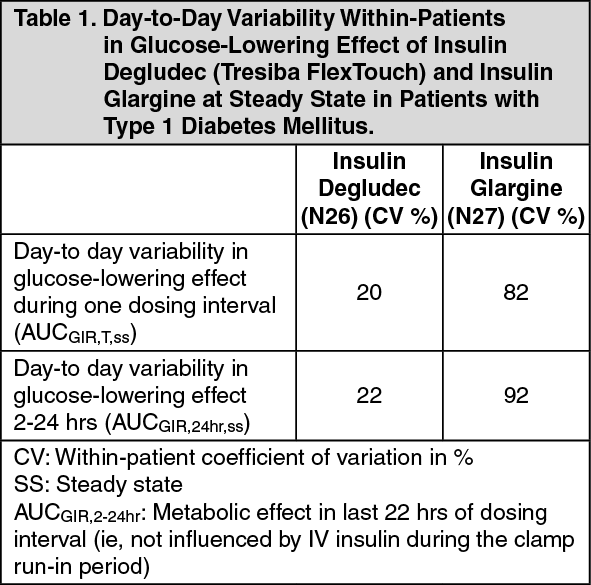 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image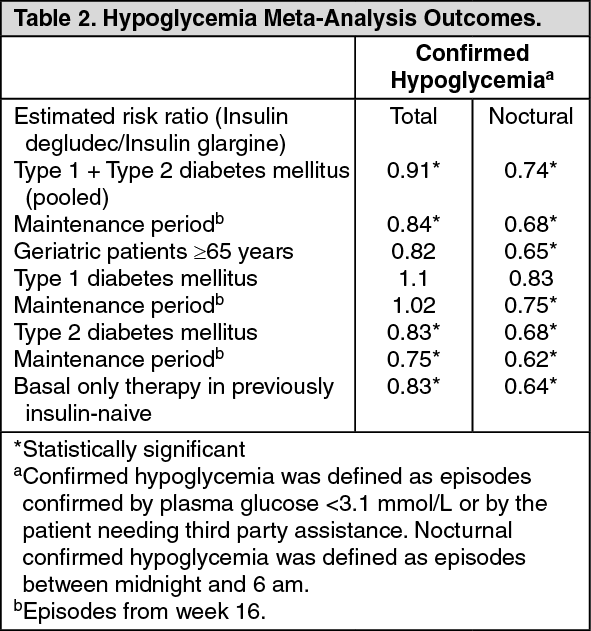 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image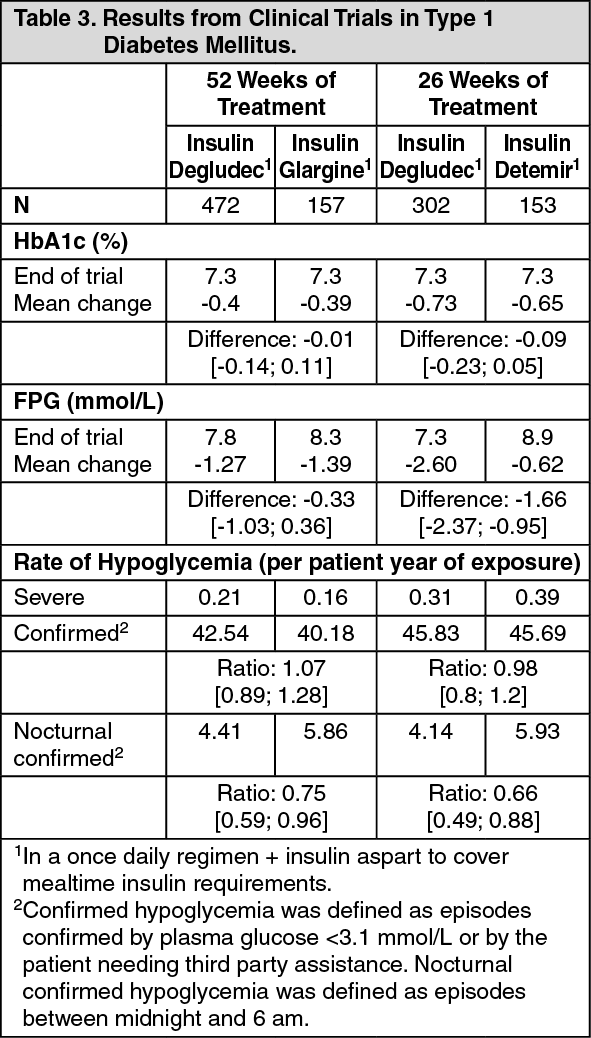 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image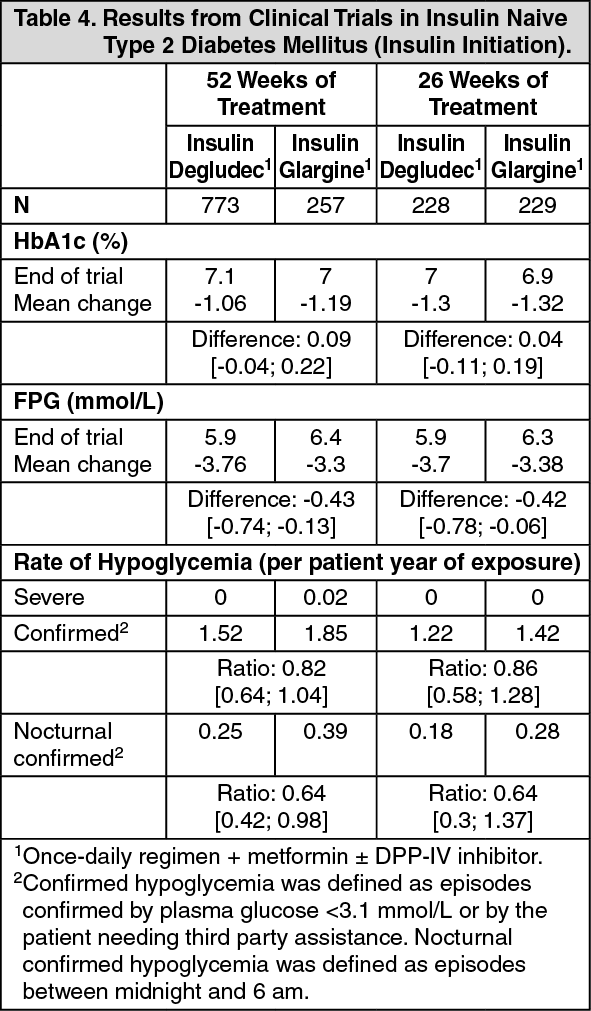 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image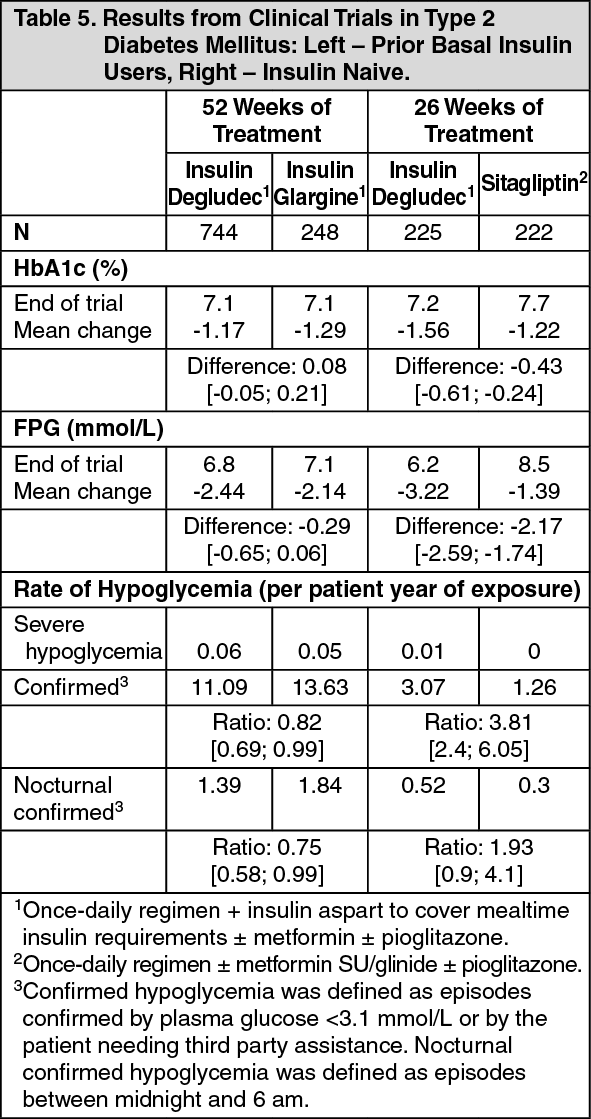 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image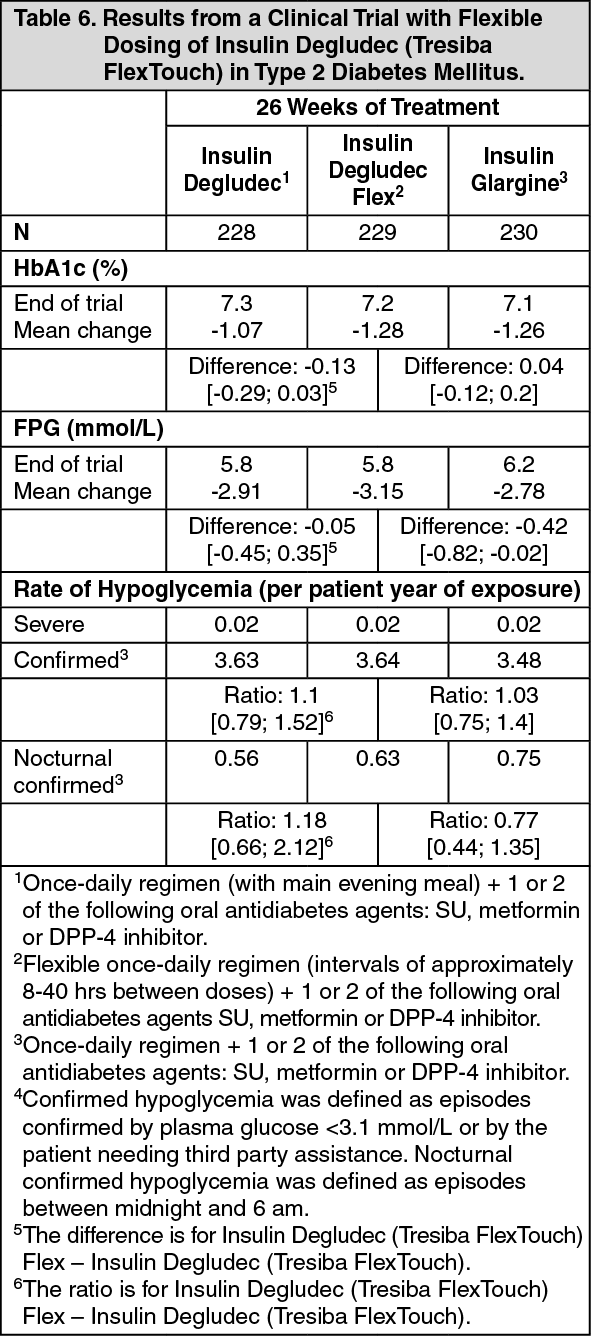 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out