Teneligliptin: Teneligliptin is well tolerated in various clinical trials. Data from 1,183 patients reported that 118 (10%) patients experienced AEs, and the most common AEs were hypoglycemia (3%) and constipation (0.9%). Hypoglycemia can occur when other antidiabetic drugs are coadministered. Intestinal obstruction may occur with Teneligliptin and must be administered cautiously in patients with a history of intestinal obstruction or surgery. This may be because of reduced gastrointestinal motility due to enhanced activity of incretins. Cases of intestinal obstruction are also reported with other gliptins.
Reported evidence suggests that no QT prolongations were noted with Teneligliptin 40mg daily dose. Nevertheless, mild and transient QTc prolongation can be seen at a supraclinical dose of 160mg/day given for a prolonged period of time in patients who are prone or have comorbid arrhythmia/ischemic heart disease and along with medications known for QT prolongation.
Intestinal obstruction (0.1%): Because bowel obstruction may occur, should be carefully observed, abdominal pain severe constipation, abdominal distension, persist, administration of this drug should be discontinued when an abnormality of vomiting etc. are observed, and appropriate measures should be taken.
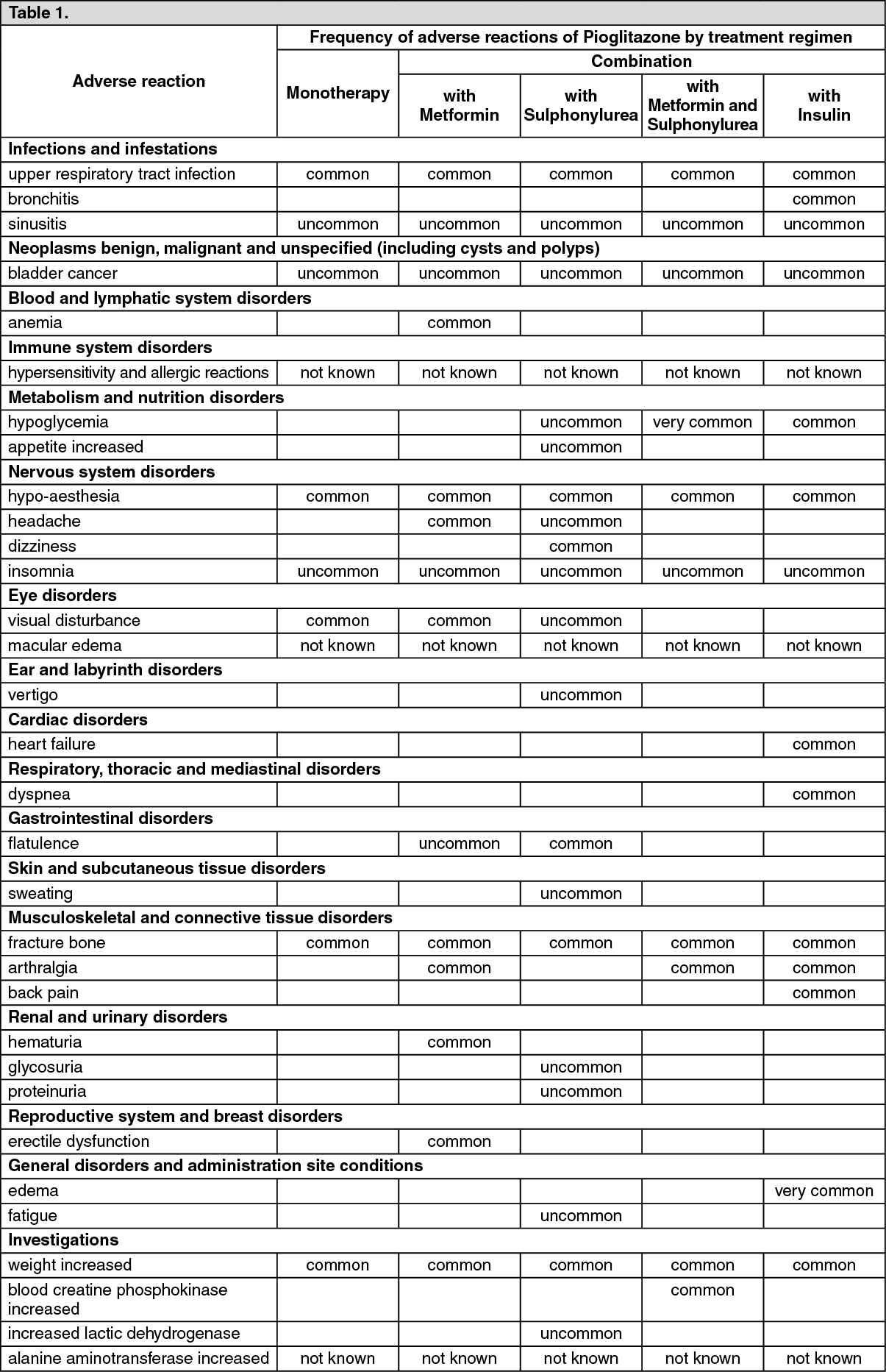
Pioglitazone: Tabulated list of adverse reactions: Adverse reactions reported in excess (> 0.5%) of placebo and as more than an isolated case in patients receiving Pioglitazone in double-blind studies are listed as follows as MedDRA preferred term by system organ class and absolute frequency. Frequencies are defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000); not known (cannot be estimated from the available data). Within each system organ class, adverse reactions are presented in order of decreasing incidence followed by decreasing seriousness. (See Table 1.)
 Click on icon to see table/diagram/image
Description of selected adverse reactions:
Click on icon to see table/diagram/image
Description of selected adverse reactions: Post-marketing reports of hypersensitivity reactions in patients treated with Pioglitazone have been reported. These reactions include anaphylaxis, angioedema, and urticaria.
Visual disturbance has been reported mainly early in treatment and is related to changes in blood glucose due to temporary alteration in the turgidity and refractive index of the lens as seen with other hypoglycemic treatments.
Edema was reported in 6-9% of patients treated with Pioglitazone over one year in controlled clinical trials. The edema rates for comparator groups (sulphonylurea, metformin) were 2-5%. The reports of edema were generally mild to moderate and usually did not require discontinuation of treatment.
In controlled clinical trials the incidence of reports of heart failure with Pioglitazone treatment was the same as in placebo, metformin and sulphonylurea treatment groups, but was increased when used in combination therapy with insulin. In an outcome study of patients with pre-existing major macrovascular disease, the incidence of serious heart failure was 1.6% higher with Pioglitazone than with placebo, when added to therapy that included insulin. However, this did not lead to an increase in mortality in this study. In this study in patients receiving Pioglitazone and insulin, a higher percentage of patients with heart failure were observed in patients aged ≥65 years compared with those less than 65 years (9.7% compared to 4.0%). In patients on insulin with no Pioglitazone the incidence of heart failure was 8.2% in those ≥65 years compared to 4.0% in patients less than 65 years. Heart failure has been reported with marketing use of Pioglitazone, and more frequently when Pioglitazone was used in combination with insulin or in patients with a history of cardiac failure.
A pooled analysis was conducted of adverse reactions of bone fractures from randomized, comparator controlled, double blind clinical trials in over 8100 patients in the Pioglitazone-treated groups and 7400 in the comparator-treated groups of up to 3.5 years duration. A higher rate of fractures was observed in women taking Pioglitazone (2.6%) versus comparator (1.7%). No increase in fracture rates was observed in men treated with Pioglitazone (1.3%) versus comparator (1.5%).
In the 3.5 year PROactive study, 44/870 (5.1%) of Pioglitazone-treated female patients experienced fractures compared to 23/905 (2.5%) of female patients treated with comparator. No increase in fracture rates was observed in men treated with Pioglitazone (1.7%) versus comparator (2.1%).
In active comparator controlled trials mean weight increase with Pioglitazone given as monotherapy was 2-3 kg over one year. This is similar to that seen in a sulphonylurea active comparator group. In combination trials Pioglitazone added to metformin resulted in mean weight increase over one year of 1.5 kg and added to a sulphonylurea of 2.8 kg. In comparator groups addition of sulphonylurea to metformin resulted in a mean weight gain of 1.3 kg and addition of metformin to a sulphonylurea a mean weight loss of 1.0 kg.
In clinical trials with Pioglitazone the incidence of elevations of ALT greater than three times the upper limit of normal was equal to placebo but less than that seen in metformin or sulphonylurea comparator groups. Mean levels of liver enzymes decreased with treatment with Pioglitazone. Rare cases of elevated liver enzymes and hepatocellular dysfunction have occurred in post-marketing experience. Although in very rare cases fatal outcome has been reported, causal relationship has not been established.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out