



 Sign Out
Sign Out
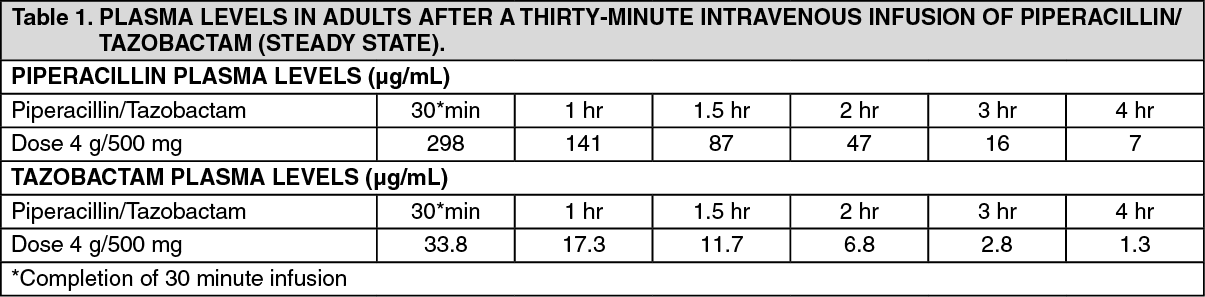
Pharmacokinetics: Distribution and plasma levels: Mean plasma concentrations of piperacillin and tazobactam at steady state of the combination appear in Table 1. Peak piperacillin and tazobactam plasma concentrations are attained immediately after completion of an intravenous infusion. When given tazobactam, piperacillin plasma levels are similar to those attained when equivalent doses of piperacillin are administered alone. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn healthy subjects piperacillin/tazobactam plasma elimination half lives range from 0.7 to 1.2 hours following single or multiple doses. These half-lives are unaffected by dose or duration of infusion. Piperacillin and Tazobactam are 21% and 23% respectively, bound to plasma proteins. The protein binding of either piperacillin or tazobactam is unaffected by the presence of either compound. Piperacillin and Tazobactam are widely distributed in tissues and body fluids including intestinal mucosa, gall bladder, lung and bile.
Biotransformation: Piperacillin does not undergo biotransformation in humans. Approximately 20% of a dose of tazobactam is metabolized to a single metabolite that has been found to be microbiologically inactive.
Excretion: Piperacillin and tazobactam are eliminated by the kidney via glomerular filtration and tubular secretion. Piperacillin is excreted rapidly as unchanged drug, with 69% of the dose appearing in the urine. Piperacillin is also secreted into bile. Tazobactam and its metabolite are eliminated primarily by renal excretion, with 80% of the dose appearing as unchanged drug and the remainder of the dose appearing as the metabolite.
Impaired renal function: The half-life of piperacillin and tazobactam increases with decreasing creatinine clearance. The increase is two-fold and four-fold for piperacillin and tazobactam, respectively, at creatinine clearance below 20 mL/min compared to patients with normal renal function. Dosage adjustment are recommended when creatinine clearance is below 40 mL/min (see Dosage & Administration).
Piperacillin and tazobactam are removed from the body during haemodialysis with 31% and 39% of the doses of piperacillin and tazobactam, respectively recovered in the dialysis fluid. Piperacillin and tazobactam are removed from the body by peritoneal dialysis with 5% and 12% of the dose, respectively, appearing in the dialysate. For dosage recommendations in patients undergoing haemodialysis. (see Dosage & Administration).
Impaired liver function: Piperacillin half-life and AUC were increased by 25% and 40% respectively and tazobactam half-life and AUC 18% and 23% respectively in patients with hepatic impairment. However, dosage adjustments in patients with hepatic impairment are not necessary.
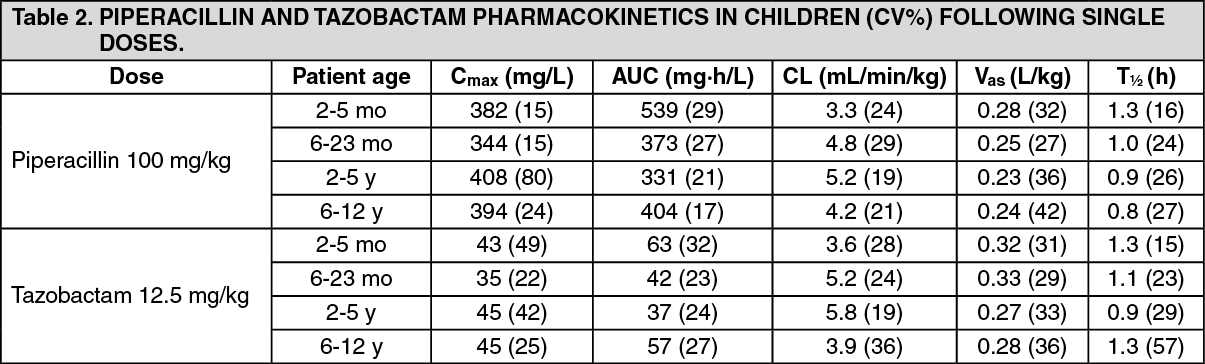
Children: The pharmacokinetics of piperacillin and tazobactam have been examined in 24 pediatric patients aged 2 months to 12 years receiving 100 mg/kg piperacillin/12.5 mg/kg tazobactam (Table 2). The maximum concentration (Cmax) for both piperacillin and tazobactam is increased relative to the maximum adult dose but the predicted time above the minimum inhibitory concentration is slightly decreased. The dosage of 100 mg/kg piperacillin/12.5 mg/kg tazobactam administered every 8 hours is predicted to provide coverage 31% to 61% of the time for the rage of MIC values of 2 μg/mL to 16 μg/mL commonly found in intra-abdominal infections in children.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMicrobiology: Piperacillin and tazobactam for injection is active against most strains of the following β-lactamase producing and non β-lactamase producing microorganisms: Gram-negative bacteria: Escherichia coli, Citrobacter spp. (including K. pneumoniae), Enterobacter spp. (including E. cloacae). Proteus vulgaris, Proteus mirabilis, Serratia spp. (including S. marcescens), Pseudomonas aeruginosa and other Pseudomonas spp., Neisseria gonorrhoeae, Neisseria meningitides, Moraxella catarrhalis, Acinetobacter spp., Haemophilus influenzae.
Gram-positive bacteria: Streptococci (S. pneumoniae, S. pyogenes, S. agalactiae, S. viridans), Enterococci (E. faecalis, E. faecium), Staphylococcus aureus (not methicillin-resistant S. aureus), S. epidermidis (coagulase-negative staphylococci).
Anaerobic bacteria: Bacteroides spp. including Bacteroides fragilis group. Peptostreptococcus spp., Fusobacterium spp., Enbacterium group, Clostridia spp., Veillonella spp.