Pink, round, film-coated tablet.
Each film-coated tablet contains: Evogliptin tartrate 6.869 mg (5 mg as Evogliptin).
Anti-Diabetic (DPP-4 inhibitor).
Pharmacology: Pharmacodynamics: Evogliptin is a member of a class of oral anti-hyperglycaemic agents called DPP-4 inhibitors. Evogliptin selectively inhibits the activity of DPP-4 by reversibly binding to DPP-4, an enzyme that inactivates incretin hormones such as GLP-1 (Glucagon-like peptide-1). Evogliptin dose-dependently inhibits the activity of DPP-4, thereby blocking GLP-1 from being inactivated by DPP-4, increasing the concentration of endogenous active GLP-1 and prolonging its action, and improves glucose-dependent insulin secretion in pancreatic beta cells by GLP- 1, and suppresses increase in blood sugar. The IC50 of evogliptin against recombinant human DPP-4 was 0.980 nM, and the inhibitory constant (Ki) was 0.525 nM. Compared to DPP-8 and DPP-9, evogliptin showed high selectivity of about 7,898 times and about 6,058 times, respectively, to DPP-4 (in vitro).
Pharmacokinetics: Absorption: After a single oral administration of evogliptin 5mg in fasting state, the maximum blood concentration reached in about 4 hours. In repeated oral administration, steady state reached in 48 hours after the first administration. Comparing the bioavailability of evogliptin 10 mg between fast state and fed state (high-fat meal), it was found that there is no food effect in terms of bioavailability of evogliptin.
Distribution: Evogliptin is widely distributed to tissues after administration. When reacting evogliptin in heparin-treated plasma of mice, rats, dogs, and humans, the plasma protein binding rates of evogliptin were about 63%, about 25%, about 43%, and about 46%, respectively; binding rates were not related to the concentration of evogliptin in the reacted range (100-1,000 ng/mL). In pregnant female rats and rabbits or lactating rats, the concentration of evogliptin in fetal plasma or milk increased maternal exposure dependently.
Metabolism: Metabolic stability of evogliptin was confirmed in in vitro tests using liver microsomes or hepatocytes. Evogliptin circulates in plasma mainly as parent, and the major metabolites are M16, M8, M7, and M13. The main metabolic pathways were hydroxylation (M7, M8), sulfation (M13) by CYP3A4 and glucuronidation by UGT2B7 (M7 → M16). The major metabolites M16, M8, M7, and M13 were all identified as active forms, but showed at least 110 times lower DPP-4 inhibitory activity compared to the evogliptin parent. Therefore, considering the blood exposure level and inhibitory activity of major metabolites, it is very unlikely that the metabolites will reach effective blood levels.
Excretion: After a single oral administration of evogliptin 5mg in fasting state, the mean half-life (t½) of elimination was about 32.5 hours. After a single oral administration of [14C]-evogliptin 5mg in fasting state, 74.9% to 93.9% were excreted through urine and feces, respectively. The average excretion rates in urine and feces were 46.1% and 42.8%, respectively, and the main excretory body was the evogliptin parent.
Suganon is indicated as an adjunct to diet and exercise to improve glycemic control in patients with type 2 diabetes mellitus.
Monotherapy; Combination therapy.
The recommended dose of Suganon is 5 mg once daily as monotherapy or combination therapy, and the maximum daily dose of Suganon is 5 mg. Suganon can be taken with or without food. Dosage and administration adjustment is not needed in patients with mild to moderate hepatic impairment.
In clinical trials of Suganon, single dose of Suganon up to 60 mg daily was administered in healthy adults. In case of an overdose, perform symptomatic therapy (e.g., remove unabsorbed substance from the gastrointestinal tract, conduct clinical monitoring including electrocardiogram), and perform supportive therapy depending on the patient's condition.
Patients who show serious hypersensitivity such as anaphylaxis or angioedema to Suganon or other dipeptidyl peptidase 4 (DPP-4) inhibitors.
Patients with type I diabetes or diabetic ketoacidosis.
Concomitant administration with drugs known to cause hypoglycemia: Insulin secretagogues such as insulin or sulfonylurea may cause hypoglycemia. Thus, lowering the dose of insulin or insulin secretagogues may be required to minimize the risk of hypoglycemia in case of concomitant administration with Suganon.
Severe and disabling joint pain: Severe and disabling joint pain has been reported in patients administering other DPP-4 inhibitors in postmarketing studies. The time to onset of symptoms following initiation of drug therapy varied from 1 day to years. Patients experienced relief of symptoms upon discontinuation of the medication. Some patients had a recurrence of severe joint pain when restarted on either their original DPP-4 inhibitor medication or another DPP-4 inhibitor. Consider DPP-4 inhibitors as a possible cause of severe joint pain and discontinue Suganon if appropriate.
Bullous pemphigoid: Postmarketing cases of bullous pemphigoid requiring hospitalization have been reported with other DPP-4 inhibitor use. In reported cases, patients typically recovered with topical or systemic immunosuppressive treatment and discontinuation of the DPP-4 inhibitor. Tell patients to report development of blisters or erosions while receiving Suganon. If bullous pemphigoid is suspected, Suganon should be discontinued and referral to a dermatologist should be considered for diagnosis and appropriate treatment.
Use in Pregnant Women: No comparative study result is available in pregnant women. Results of animal studies showed that evogliptin was detected in the blood stream of fetus across the placenta up to 61.7% in pregnant rats and 14.1% in pregnant rabbits 2 hours after administration. Therefore, use in pregnant women is not recommended.
Use in Nursing Mothers: It is not evaluated whether Suganon is excreted in human milk. Since animal studies confirmed that evogliptin is secreted in the milk, Suganon should not be used in nursing mothers.
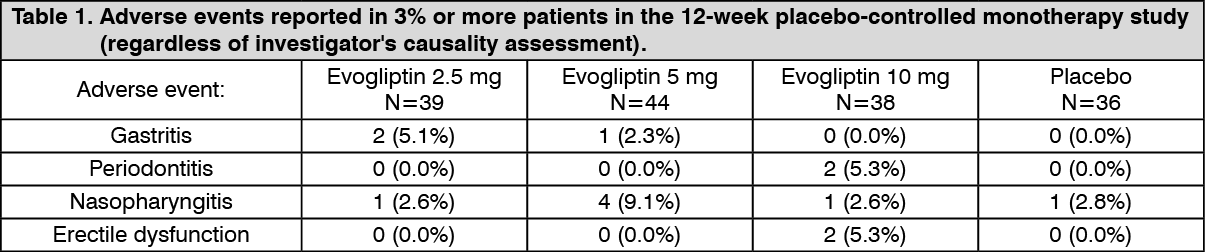
Monotherapy: In the 12-week placebo-controlled monotherapy study using 2.5 mg, 5 mg, or 10 mg of Suganon or placebo once daily, the adverse events reported with a frequency of 3% or higher are listed in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In the 24-week placebo-controlled monotherapy study using 5 mg of Suganon or placebo once daily, the adverse events reported with a frequency of 3% or higher are listed in Table 2. (See Table 2.)
Click on icon to see table/diagram/image
In patients administering Suganon 5 mg once daily as monotherapy for 52 weeks, the adverse events that occurred during the extension period (last 28 weeks) regardless of causality with increased frequency by 1% or higher compared to those of the 24-week study were toothache (3.1% vs. 1.3%) and contact dermatitis (3.1% vs. 1.3%). Compared to the 24-week study, there was no newly reported adverse event that occurred in two or more patients (3.1 %).
Combination therapy: In the 24-week active-drug-controlled combination therapy study with stable doses of metformin and either Suganon 5 mg or sitagliptin 100 mg once daily, the adverse events reported with a frequency of 3% or higher are listed in Table 3. (See Table 3.)
Click on icon to see table/diagram/image
In the 52-week study using Suganon 5 mg once daily combined with metformin, the adverse events that occurred during the extension period (last 28 weeks) regardless of causality with increased frequency by 1% or higher compared to those of the 24-week study were gastritis (2.2% vs. 0.9%) and upper respiratory tract infection (4.3% vs. 2.7%). Compared to the 24-week study, sciatica (2.2%) was a newly reported adverse event that occurred in two or more patients (2.2%).
Hypoglycemia: In the 24-week monotherapy and combination therapy study with evogliptin 5 mg, hypoglycemia was each reported in one patient (monotherapy 1.3%, combination therapy 0.9%). All reported hypoglycemia cases were mild in severity and resolved without any action taken.
Vital signs: No clinically significant change in vital signs was observed in patients treated with Suganon.
Bullous pemphigoid: There have been postmarketing reports of bullous pemphigoid requiring hospitalization in patients taking other DPP-4 inhibitors.
Evogliptin is mainly metabolized by CYP3A4. In in vitro studies, evogliptin was not an inhibitor of CYP1A2, 2B6, 2C8, 2C9, 2C19, 206, and 3A4 enzymes or an inducer of CYP1A2, 2B6, and 3A4 enzymes. Thus, evogliptin is unlikely to cause interactions with other drugs acting as a substrate of such enzymes. Although evogliptin was proved to be a
p-glycoprotein (P-gp) substrate and weak BCRP substrate based on in vitro studies, it did not inhibit transport mediated by these transporters. In addition, evogliptin was not a substrate of OAT1, OAT3, OCT2, OATP1 B1, and OATP1 B3 and did not inhibit them. Therefore, evogliptin is unlikely to cause interactions with drugs that act as a substrate of such transporters in the clinical dose.
Interaction of evogliptin with other drugs: Metformin: Multiple administration of evogliptin 5 mg and twice daily metformin 1,000 mg (a substrate of OCT1 and OCT2) until steady state was reached did not show clinically meaningful change in the pharmacokinetics of evogliptin or metformin.
Clarithromycin: Multiple administration of a potent CYP3A4 inhibitor, clarithromycin 1,000 mg/day, until steady state was reached and single administration of evogliptin 5 mg showed increased Cmax of evogliptin by 2.1 times and its AUC by 2.0 times. Caution needs to be exercised as pharmacokinetic exposure of evogliptin may increase with concomitant administration of CYP3A4 inhibitors.
Instructions and Special Precautions for Handling and Disposal: As keeping this drug in other containers may result in an accident caused by misuse or in decreased quality of the drug, store in the original container.
Store at temperatures not exceeding 30°C.
A10BH07 - evogliptin ; Belongs to the class of dipeptidyl peptidase 4 (DPP-4) inhibitors. Used in the treatment of diabetes.
Suganon FC tab 5 mg
30's (P1,620/box)



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image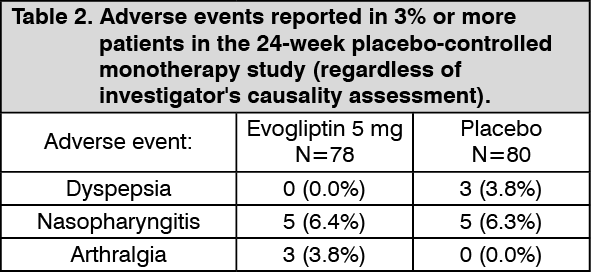 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image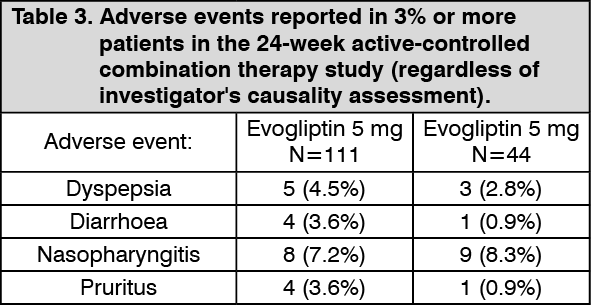 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out