5α-reductase inhibitor.
Pharmacology: Pharmacodynamics: Finasteride is a competitive and specific inhibitor of Type II 5α-reductase, an intracellular enzyme that converts the androgen testosterone into DHT. Two distinct isozymes are found in mice, rats, monkeys, and humans: Type I and II. Each of these isozymes is differentially expressed in tissues and developmental stages, In humans, Type I 5α-reductase is predominant in the sebaceous glands of most regions of skin, including scalp, and liver. Type I 5α-reductase is responsible for approximately one-third of circulating DHT. The Type II 5-reductase isozyme is primarily found in prostate, seminal vesicles, epididymides, and hair follicles as well as liver, and is responsible for two-thirds of circulating DHT.
In humans, the mechanism of action of finasteride is based on its preferential inhibition of the Type II isozyme. Using native tissues (scalp and prostate), in vitro binding studies examining the potential of finasteride to inhibit either isozyme revealed a 100-fold selectivity for the human Type II 5α-reductase over Type I isozyme (IC
50=500 and 4.2 nM for Type I and II, respectively). For both isozymes, the inhibitions by finasteride are accompanied by reduction of the inhibitor to dihydrofinasteride and adduct formation with NADP+. The turnover for the enzyme complex is slow (t
1/2 approximately 30 days for the Type II enzyme complex and 14 days for the Type I complex).
Finasteride has no affinity for the androgen receptor and has no androgenic, antiandrogenic, estrogenic, antiestrogenic, or progestational effects. Inhibition of Type II 5α-reductase blocks the peripheral conversion of testosterone to DHT resulting in significant decreases in serum and tissue DHT concentrations. Finasteride produces a rapid reduction in serum DHT concentration, reaching 65% suppression within 24 hours of oral dosing with a 1 mg tablet. Mean circulating levels of testosterone and estradiol were increased by approximately 15% as compared to baseline, but these remained within the physiologic range.
In men with male pattern hair loss (androgenetic alopecia), the balding scalp contains miniaturized hair follicles and increased amounts of DHT compared with hairy scalp. Administration of finasteride decreases scalp and serum DHT concentrations in these men. The relative contributions of these reductions to the treatment effect of finasteride have not been defined. By this mechanism, finasteride appears to interrupt a key factor in the development of androgenetic alopecia in those patients genetically predisposed.
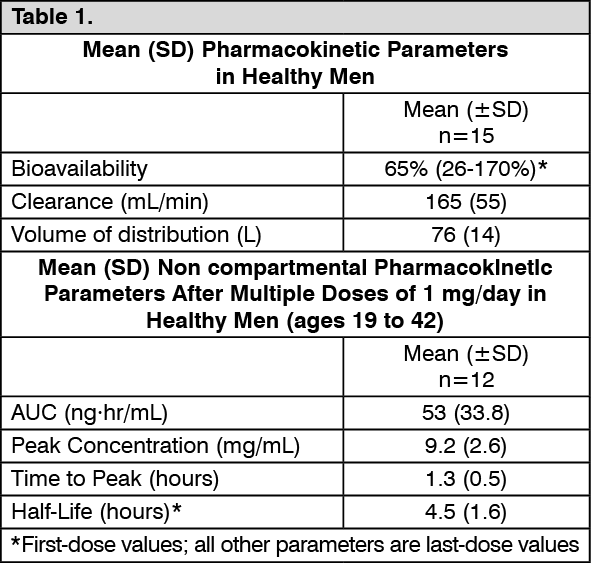
Pharmacokinetics: Absorption: In a study of 15 healthy young male subjects, the mean bioavailability of finasteride 1 mg tablets was 65% (range, 26 to 170%), based on the ratio of area under the curve (AUC) relative to an intravenous (IV) reference dose. At steady state following dosing with 1 mg/day (n=12), maximum finasteride plasma concentration averaged 9.2 ng/mL (range, 4.9 to 13.7 ng/mL) and was reached 1 to 2 hours postdose: AUC
(0 to 24 hr) was 53 ng·hr/ml (range, 20 to 154 ng·hr/mL). Bioavailability of finasteride was not affected by food.
Distribution: Mean steady-state volume of distribution was 76 liters (range, 44 to 96 liters: n=15). Approximately 90% of circulating finasteride is bound to plasma proteins. There is a slow accumulation phase for finasteride after multiple dosing.
Finasteride has been found to cross the blood-brain barrier.
Metabolism: Finasteride is extensively metabolized in the liver, primarily via the cytochrome P450 3A4 enzyme subfamily, two metabolites, the t-butyl side chain monohydroxylated and monocarboxylic acid metabolites, have been identified that possess no more than 20% of the 5α-reductase inhibitory activity of finasteride.
Excretion: Following intravenous infusion in healthy young subjects (n=15), mean plasma clearance of finasteride was 165 mL/min (range, 70 to 279 mL/min). Mean terminal half-life in plasma was 4.5 hours (range, 3.3 to 13.4 hours: n=12). Following an oral dose of
14C-finasteride in man (n=6), a mean of 39% (range, 32 to 46%) of the dose was excreted in the urine in the form of metabolites: 57% (range, 51 to 64%) was excreted in the feces.
Mean terminal half-life is approximately 5 to 6 hours in men 18 to 60 years of age and 8 hours in men more than 70 years of age.
Special populations: Pediatric: Finasteride pharmacokinetics have not been investigated in patients <18 years of age.
Gender: Finasteride tablets are not indicated for use in women.
Geriatric: No dosage adjustment is necessary in the elderly. Although the elimination rate of finasteride is decreased in the elderly, these findings are of no clinical significance. (See also Pharmacodynamics: Pharmacokinetics: Excretion as previously mentioned and Use in the Elderly under Precautions).
Race: The effect of race on finasteride pharmacokinetics has not been studied.
Renal Insufficiency: No dosage adjustment is necessary in patients with renal insufficiency. In patients with chronic renal impairment, with creatinine clearances ranging from 9.0 to 55 mL/min, AUC, maximum plasma concentration, half-life, and protein binding after a single dose of
14C-finasteride were similar to those obtained in healthy volunteers. Urinary excretion of metabolites was decreased in patients with renal impairment. This decrease was associated with an increase in fecal excretion of metabolites. Plasma concentrations of metabolites were significantly higher in patients with renal impairment (based on a 60% increase in total radioactivity AUC). However, finasteride has been well tolerated in men with normal renal function receiving up to 80 mg/day for 12 weeks, where exposure of these patients to metabolites would presumably be much greater.
Hepatic Insufficiency: The effect of hepatic insufficiency on finasteride pharmacokinetics has not been studied. Caution should be used in the administration of finasteride tablets in patients with liver function abnormalities, as finasteride is metabolized extensively in the liver. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out