



 Sign Out
Sign Out
Adults with normal renal function (GFR=90 mL/min): For patients inadequately controlled on maximal tolerated dose of metformin monotherapy: For patients not adequately controlled on metformin alone, the usual starting dose should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose) plus the dose of metformin already being taken.
For patients switching from co-administration of sitagliptin and metformin: For patients switching from co-administration of sitagliptin and metformin, Metformin Hydrochloride + Sitagliptin should be initiated at the dose of sitagliptin and metformin already being taken.
For patients inadequately controlled on dual combination therapy with the maximal tolerated dose of metformin and a sulfonylurea: The dose should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose) and a dose of metformin similar to the dose already being taken. When Metformin Hydrochloride + Sitagliptin is used in combination with a sulfonylurea, a lower dose of the sulfonylurea may be required to reduce the risk of hypoglycemia.
For patients inadequately controlled on dual combination therapy with the maximal tolerated dose of metformin and a PPARγ agonist: The dose should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose) and a dose of metformin similar to the dose already being taken.
For patients inadequately controlled on dual combination therapy with insulin and the maximal tolerated dose of metformin: The dose should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose) and a dose of metformin similar to the dose already being taken. When Metformin Hydrochloride + Sitagliptin is used in combination with insulin, a lower dose of insulin may be required to reduce the risk of hypoglycemia.
For the different doses on metformin, Metformin Hydrochloride + Sitagliptin is available in strengths of 50 mg sitagliptin and 850 mg metformin hydrochloride or 1,000 mg metformin hydrochloride.
All patients should continue their recommended diet with an adequate distribution of carbohydrate intake during the day.
Special populations: Renal impairment: No dose adjustment is needed for patients with mild renal impairment (glomerular filtration rate [GFR]=60 mL/min). A GFR should be assessed before initiation of treatment with metformin-containing products and at least annually thereafter. In patients at increased risk of further progression of renal impairment and in the elderly, renal function should be assessed more frequently, e.g. every 3-6 months.
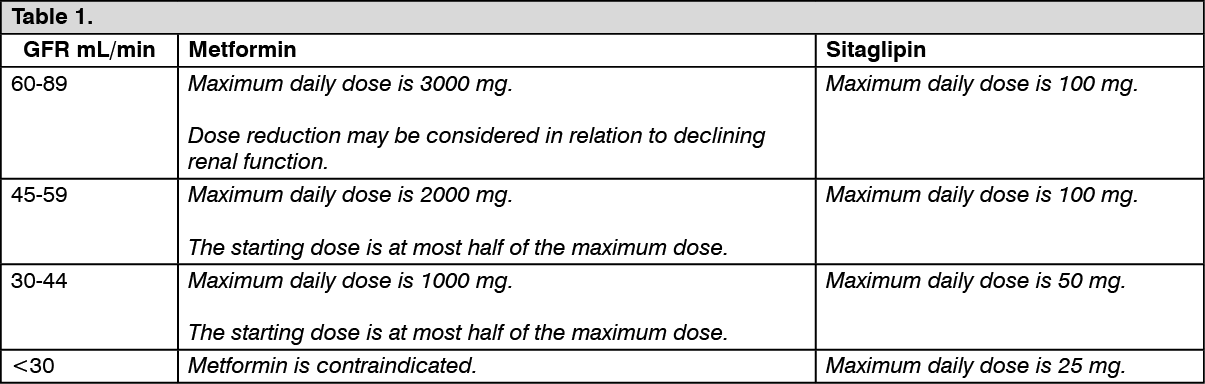
The maximum daily dose of metformin should preferably be divided into 2-3 daily doses. Factors that may increase the risk of lactic acidosis should be reviewed before considering initiation of metformin in patients with GFR <60 mL/min.
If no adequate strength of Metformin Hydrochloride + Sitagliptin is available, individual mono components should be used instead of the fixed-dose combination. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageHepatic impairment: Metformin Hydrochloride + Sitagliptin must not be used in patients with hepatic impairment.
Elderly: As Metformin and Sitagliptin are excreted by the kidney, Metformin Hydrochloride + Sitagliptin should be used with caution as age increases. Monitoring of renal function is necessary to aid in prevention of metformin-associated lactic acidosis, particularly in the elderly.
Pediatric population: The safety and efficacy of Metformin Hydrochloride + Sitagliptin in children and adolescents from birth to <18 years of age have not been established. No data are available.
Method of administration: Metformin Hydrochloride + Sitagliptin should be given twice daily with meals to reduce the gastrointestinal adverse reactions associated with metformin.