



 Sign Out
Sign Out
Combination use with Cisplatin: Malignant Pleural Mesothelioma and Nonsquamous Non-Small Cell Lung Cancer: The recommended dose of Pemetrexed is 500 mg/m2 body surface area (BSA) administered as an intravenous infusion over 10 minutes on Day 1 of each 21-day cycle. The recommended dose of Cisplatin is 75 mg/m2 BSA, and the infusion time should be more than 2 hours. Cisplatin should be administered 30 minutes after finishing i.v. infusion of Pemetrexed of the first day of the 21-day cycle. Patients should receive appropriate hydration prior to and/or after receiving Cisplatin. See Cisplatin package insert for more information.
The single-agent use: Nonsquamous Non-Small Cell Lung Cancer: For patients with nonsquamous non-small cell lung cancer who have received prior chemotherapy, the recommended dose of Pemetrexed is 500 mg/m2 BSA, administered as an intravenous infusion over 10 minutes on Day 1 of each 21-day cycle.
Premedication Regimen: Vitamin Supplementation: To reduce toxicity, patients treated with Pemetrexed must be instructed to take a low-dose oral folic acid preparation or multivitamin with folic acid on a daily basis. In the former 7 days of the first time after administering Pemetrexed, folic acid must be taken once daily for at least 5 days, and dosing should continue during the full course of therapy and for 21 days after the last dose of Pemetrexed. Patients must also receive one intramuscular injection of vitamin B12 during the week preceding the first dose of Pemetrexed and every 3 cycles thereafter. Subsequent vitamin B12 injections may be given the same day as treatment with Pemetrexed. In clinical trials, the dose of folic acid studied ranged from 350 to 1000 μg, and the dose of vitamin B12 was 1000 μg. The most commonly used dose of oral folic acid in clinical trials was 400 μg (see Precautions).
Corticosteroid Supplementation: Skin rash has been reported more frequently in patients not pretreated with a corticosteroid. Pretreatment with dexamethasone (or equivalent) reduces the incidence and severity of cutaneous reaction. In clinical trials, dexamethasone 4 mg was given orally twice daily the day before, the day of, and the day after Pemetrexed administration (see Precautions).
Laboratory Monitoring and Dose Reduction/Discontinuation Recommendations: Monitoring: Complete blood cell counts, including platelet counts, should be performed on all patients receiving Pemetrexed. Patients should be monitored for nadir and recovery, which were tested in the clinical study before each dose and on days 8 and 15 of each cycle. Periodic biochemistry tests should be performed to evaluate renal and hepatic function. Patients should not begin a new cycle of treatment unless the ANC is not less than 1500 cells/mm3, the platelet count is not less than 100,000 cells/mm3, creatinine clearance is not less than 45 mL/min, total bilirubin is not more than 1.5 ULN, alkaline phosphatase (AP), aspartic transaminase (AST or SGOT) and Alanine Aminotransferase (ALT or SGPT) are not more than 3 ULN. If liver is involved, alkaline phosphatase, AST and ALT not more than 5 ULN is accepted [see Precautions].
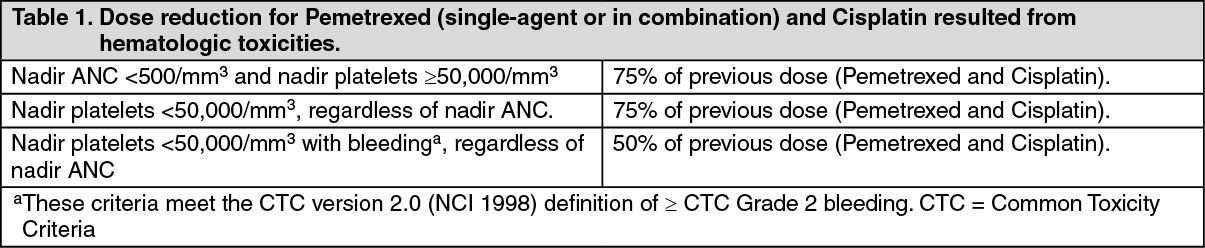
Dose Reduction Recommendations: Dose adjustments at the start of a subsequent cycle should be based on nadir hematologic counts or maximum non-hematologic toxicity from the preceding cycle of therapy. Treatment may be delayed to allow sufficient time for recovery. Upon recovery, patients should be retreated using the guidelines in Tables 1-3, which are suitable for using Pemetrexed as a single-agent or in combination with Cisplatin. (See Table 1.)
 Click on icon to see table/diagram/image
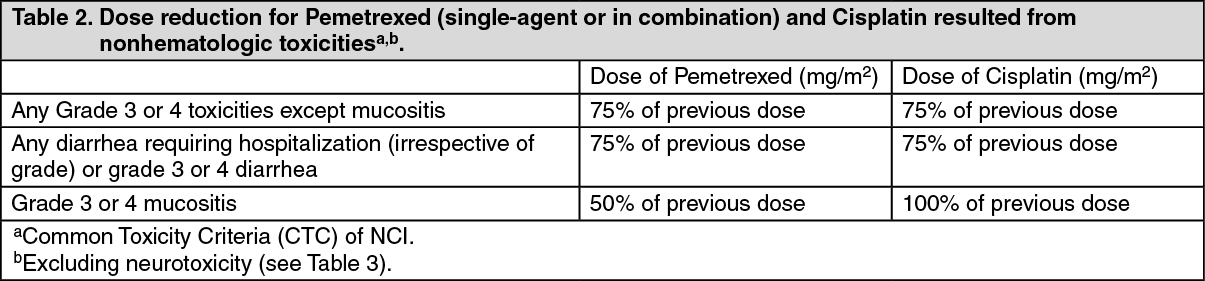
Click on icon to see table/diagram/imageIf patients develop nonhematologic toxicities (excluding neurotoxicity) ≥Grade 3, treatment should be withheld until resolution to less than or equal to the patient's pre-therapy value. Treatment should be resumed according to guidelines in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the event of neurotoxicity, the recommended dose adjustments for Pemetrexed and Cisplatin are described in Table 3. Patients should discontinue therapy if Grade 3 or 4 neurotoxicity is experienced. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDiscontinuation Recommendation: Pemetrexed therapy should be discontinued if a patient experiences any hematologic or nonhematologic Grade 3 or 4 toxicity after 2 dose reductions or immediately if Grade 3 or 4 neurotoxicity is observed.
Renally Impaired Patients: In clinical studies, patients with creatinine clearance ≥45 mL/min required no dose adjustments other than those recommended for all patients. Insufficient numbers of patients with creatinine clearance less than 45 mL/min have been treated to make dosage recommendations for this group of patients [see Pharmacology: Pharmacokinetics under Actions]. Therefore, calculate creatinine clearance based on standard Cockcroft and Gault formula (as follows) or GFR measured by Tc99m-DPTA serum clearance method. Pemetrexed should not be administered to patients whose creatinine clearance is less than 45 mL/min. (See equation.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageBe careful when administering Pemetrexed concurrently with NSAIDs to patients whose creatinine clearance is <80 mL/min (see Interactions).
Liver Impaired Patients: No pharmacokinetics relationship between AST (SGOT), ALT (SGPT) or total bilirubin and Pemetrexed is found. There is no special study conducted on liver impaired patients, such as total bilirubin >1.5 ULN or transaminase >3.0 ULN (No liver metastasis exist) or >5.0 ULN (Liver metastasis exist).
Precautions for Preparation and Administration: As with other potentially toxic anticancer agents, be careful in the handling and preparation of infusion solutions of Pemetrexed. The use of gloves is recommended. If a solution of Pemetrexed contacts the skin, wash the skin immediately and thoroughly with soap and water. If Pemetrexed contacts the mucous membranes, flush thoroughly with water.
Pemetrexed is not a vesicant. There is no specific antidote for extravasation of Pemetrexed. To date, there have been few reported cases of Pemetrexed extravasation, which were not assessed as serious by the investigator.
Pemetrexed extravasation should be managed with local standard practice for extravasation as with other non-vesicants.
Preparation for Intravenous Infusion Solution: (1). Use aseptic technique during redissolving and further dilution of Pemetrexed for intravenous infusion administration.
(2). Calculate the dose of Pemetrexed and determine the number of vials needed. The vials contain an excess of Pemetrexed to facilitate delivery of label amount.
(3). Reconstitute each 200-mg vial with 8 mL of 9 mg/mL (0.9%) Sodium Chloride Injection (preservative free). Reconstitution of either size vial gives a solution containing 25 mg/mL Pemetrexed. Gently swirl each vial until the powder is completely dissolved. The resulting solution is clear and ranges in color from colorless to yellow or green-yellow without adversely affecting product quality. The pH of the reconstituted Pemetrexed solution is between 6.6 and 7.8. FURTHER DILUTION IS REQUIRED.
(4). Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. If particulate matter is observed, do not administer.
(5). An appropriate quantity of the reconstituted Pemetrexed solution must be further diluted into a solution of 0.9% Sodium Chloride Injection (preservative free), so that the total volume of solution is 100 mL. Pemetrexed is administered as an intravenous infusion over 10 minutes.
(6). Chemical and physical stability of reconstituted and infusion solutions of Pemetrexed were demonstrated for up to 24 hours following initial reconstitution, when stored at refrigerated or ambient room temperature and lighting. When prepared as directed, reconstitution and infusion solutions of Pemetrexed contain no antimicrobial preservatives. Discard any unused portion.
(7). Prepared Pemetrexed is appropriate for PVC and intravenous injection bag.
(8). Reconstitution and further dilution prior to intravenous infusion is only recommended with 0.9% Sodium Chloride Injection (preservative free). Pemetrexed is physically incompatible with diluents containing calcium, including Lactated Ringer's Injection (USP) and Ringer's Injection (USP) and therefore these should not be used. Co-administration of Pemetrexed with other drugs and diluents has not been studied, and therefore is not recommended.