General (applies to all uses of iodinated contrast media): As follows are listed as possible general side effects in relation with radiographic procedures which include the use of non-ionic monomeric contrast media. For side effects specific to mode of administration, refer to the specific sections.
The listed frequencies are based on internal clinical documentation and published large scale studies, comprising more than 200,000 patients.
Undesirable effects associated with the use of iodinated contrast media are usually mild to moderate and transient in nature, and less frequent with non-ionic than with ionic contrast media. Serious reactions as well as fatalities are only seen on very rare occasions. The most frequent adverse event is a mild, general sensation such as a feeling of warmth or a transient metallic taste.
Abdominal discomfort/pain is very rare (incidence <1:1000) and gastrointestinal reactions like nausea or vomiting are rare (incidence <1:100, but >1:1000).
Hypersensitivity reactions are rare and usually present as mild respiratory or cutaneous symptoms like dyspnoe, rash, erythema, urticaria, pruritus and angioedema.
They may appear either immediately after the injection or up to a few days later. Severe manifestations such as laryngeal oedema, bronchospasm or pulmonary oedema are very rare. Severe and even toxic skin reactions have been reported.
Anaphylactoid reactions may occur irrespectively of the dose and mode of administration and mild symptoms of hypersensitivity may represent the first signs of a serious reaction. Administration of the contrast medium must be discontinued immediately and, if necessary, specific therapy instituted via the vascular access. Patients using beta blockers may present with atypical symptoms of anaphylaxis which may be misinterpreted as a vagal reaction.
Vagal reactions giving hypotension and bradycardia are seen on very rare occasions. Headache of fever may occur. Episodes of hypertension may also occur. Pyrexia with rigors are seen on rare occasions.
Iodism or "iodide mumps" is a very rare complication of iodinated contrast media resulting in swelling and tenderness of the salivary glands for up to approximately 10 days after the examination.
Intravascular use (Intraarterial and Intravenous use): First read General as previously mentioned. As follows, only undesirable events with frequency during intravascular use of non-ionic monomeric contrast media are described.
The nature of the undesirable effects specifically seen during intraarterial use depend on the site of injection and dose given. Selective arteriographies and other procedures in which the contrast medium reaches a particular organ in high concentrations may be accompanied by complications in that particular organ. Distal pain or heat sensation in peripheral angiography is common (incidence >1:10).
A transient increase in S-creatinine is common after iodinated contrast media, but usually of no clinical relevance. Renal failure is very rare. However, renal failure may occur in high risk patients and among such patients fatalities have been reported.
Arterial spasm may follow injection into coronary, cerebral or renal arteries and result in transient ischaemia.
Neurological reactions are very rare. They may include seizures or transient motor or sensory disturbances. On very rare occasions the contrast medium may cross the blood-brain barrier resulting in uptake of contrast medium in the cerebral cortex being visible on CT-scanning until the day following examination, sometimes associated with transient confusion or cortical blindness.
Serious cardiac complications, including cardiac arrest, arrhythmia, depression or signs of ischaemia, are very rare. Post phlebographic thrombophlebitis or thrombosis is very rare. A very few cases of arthralgia has been reported.
Intrathecal use: First read General as previously mentioned. as follows, only undesirable events with frequency during intrathecal use of non-ionic monomer contrast media are described.
Undesirable effects following intrathecal use may be delayed and present some hours or even days after the procedure. The frequency is similar to lumbar puncture alone.
Headache, nausea, vomiting or dizziness are common and may largely be attributed to pressure loss in the subarachnoid space resulting from leakage at the puncture site. Some of these patients may experience a severe headache lasting for several days. Excessive removal of cerebrospinal fluid should be avoided in order to minimize pressure loss.
Mild local pain, paraesthesia and radicular pain occasionally (incidence <1:10, but >1:100) occur at the site of injection. Cramping and pain in the lower limbs are seen on very rare occasions.
Meningeal irritation giving photophobia and meningism happens occasionally. Frank chemical meningitis appear on very rare occasions. The possibility of an infective meningitis should also be considered. On very rare occasions, manifestations of transient cerebral dysfunction are seen. These include seizures, transient confusion or transient motor or sensory dysfunction. Changes in the EEG may be noted in a few of these patients.
Use in Body Cavities: First read General. As follows, only undesirable events with frequency during use of non-ionic monomeric contrast media in body cavities are described.
Systemic hypersensitivity reactions are rare.
Endoscopic Retrograde Choleangio Pancreatography (ERCP): Some elevation of amylase levels is common. Post ERCP renal opacification is seen on rare occasions and is associated with an increased risk of post ERCP pancreatitis. Rare cases of necrotizing pancreatitis have also been described.
Oral use: Gastrointestinal upset occasionally occur.
Hysterosalpingography (HSG): Transient pain in the lower abdomen is common.
Arthrography: Post procedural pain is common. Frank arthritis is rare. The possibility of infective arthritis should be considered in such cases.
Herniography: Mild postprocedural pain is common.




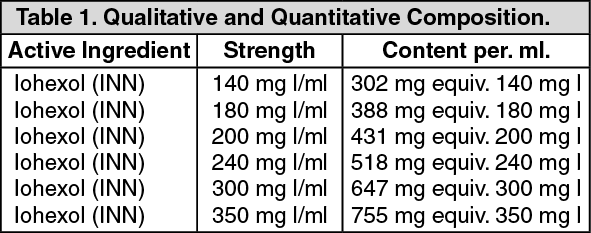 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image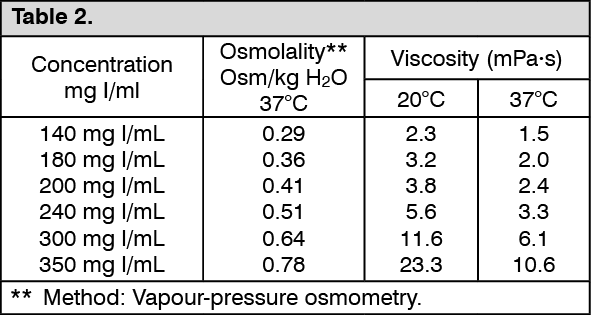 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image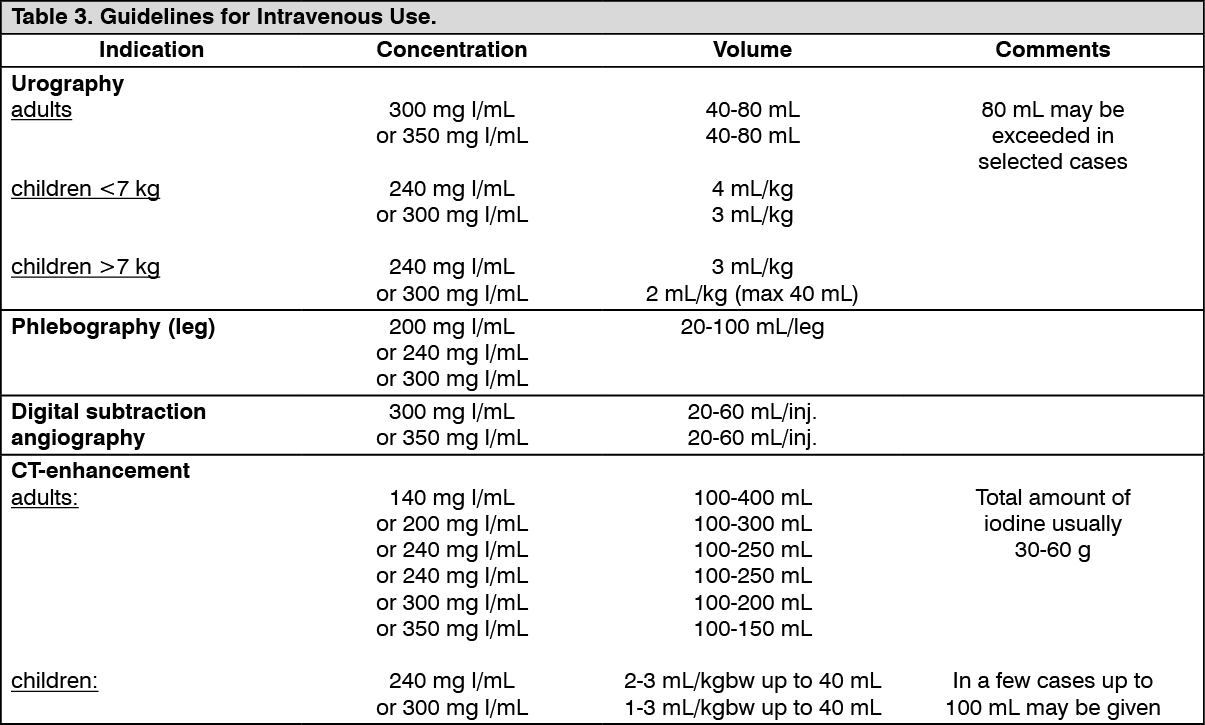 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image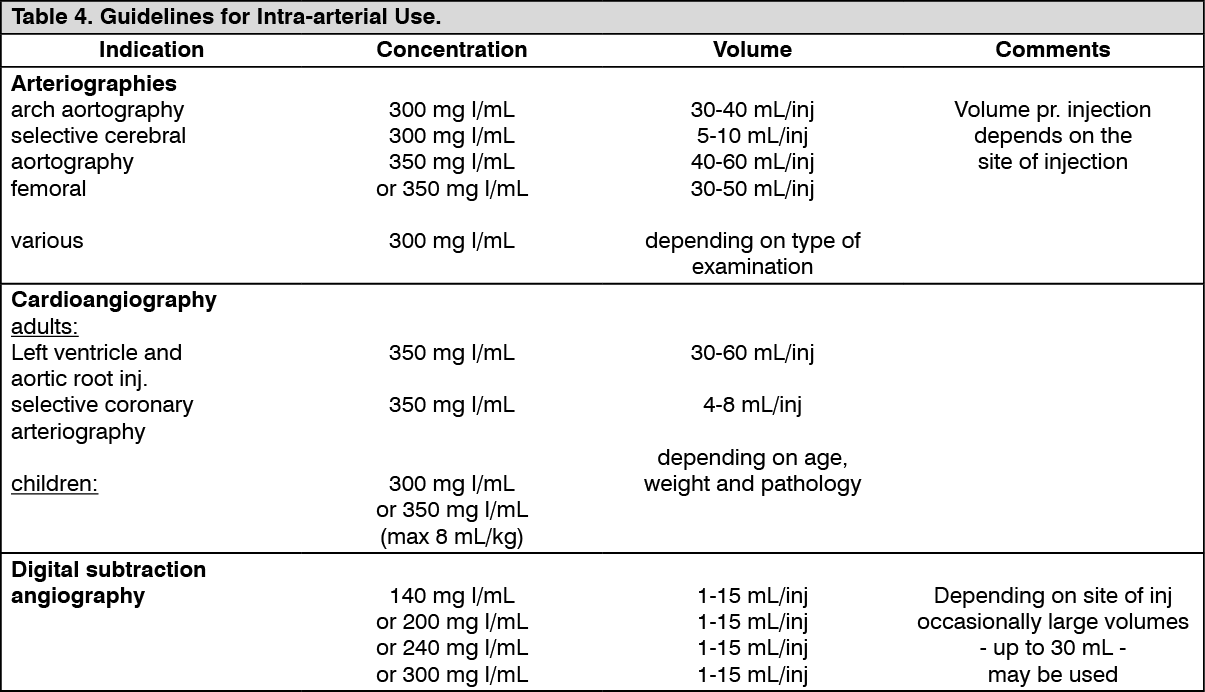 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image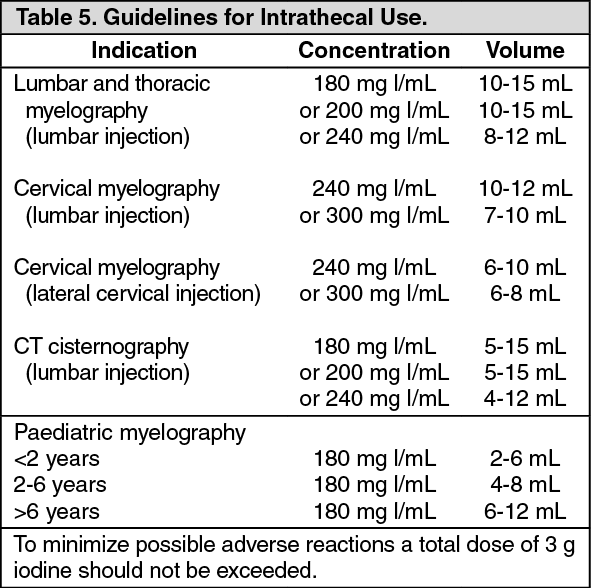 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image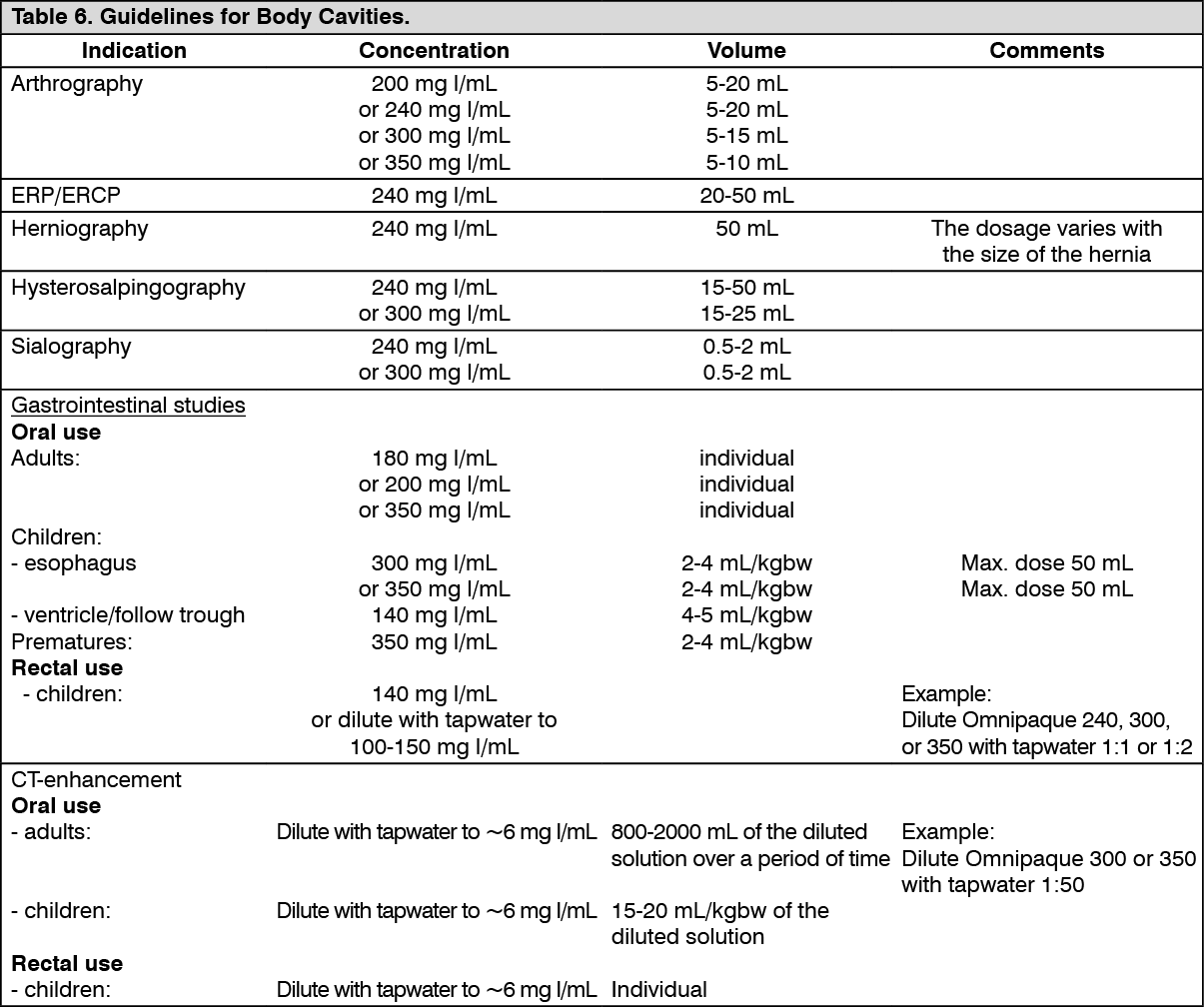 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out