The overall incidence of adverse reactions has been established from clinical studies in which 316 patients (132 patients suffering from NSCLC and 184 patients suffering from breast cancer) received the recommended protocol for vinorelbine soft-gelatin capsule (first three administrations at a dose of 60 mg/m
2/week followed by administrations at a dose of 80 mg/m
2/week).
The adverse reactions reported have been listed as follows by system organ class and incidence. The additional adverse reactions pooled from post-marketing experience and clinical trials have been added with unknown incidence consistent with the MedDRA classification.
The reactions are defined as follows using the NCI CTC severity grades. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The reactions are described using the WHO classification (grade 1=G1; grade 2=G2; grade 3=G3; grade 4=G4; grade 1-4=G1-4; grade 1-2=G1-2; grade 3-4=G3-4).
Adverse reactions reported with vinorelbine soft-gelatin capsule: Pre-marketing experience: The most commonly reported adverse effects are bone marrow depression with neutropenia, anaemia and thrombocytopenia together with gastrointestinal toxicity, with nausea, vomiting, diarrhoea, stomatitis and constipation. Fatigue and fever have also been reported commonly.
Post-marketing experience: Vinorelbine soft-gelatin capsule is used as monotherapy or in combination with other chemotherapeutic agents such as cisplatin or capecitabin.
The system organ classes most affected in post-marketing experience are the "Haematological and lymphatic system disorders", the "Gastrointestinal disorders" and the "general disorders and administration site abnormalities". This information is consistent with the pre-marketing experience.
Infections and Infestations: Very common: Bacterial, viral or fungal infections without neutropenia affecting different systems (respiratory, gastrointestinal, urinary) G1-4: 12.7%; G3-4: 4.4%.
Common: Bacterial, viral or fungal infections as a result of bone marrow depression or immunological disorder (infections associated with neutropenia) usually reversible with appropriate treatment.
Infections associated with G3-4 neutropenia: 3.5%.
Not known: Septic neutropenia. Complicated septicaemia, occasionally fatal.
Severe sepsis sometimes with other organ failure.
Septicemia.
Blood and lymphatic system disorders: Very common: Bone marrow depression, particularly causing neutropenia (G1-4: 71.5%; G3: 21.8%: G4 25.9%; reversible and representing the dose limiting toxicity.
Leucopenia G1-4: 70.6%; G3: 24.7% : G4: 6%.
Anaemia G1-4: 67.4%; G3-4: 3.8%.
Thrombocytopenia G1-2: 10.8%.
Common: G4 neutropenia associated with fever over 38°C, including 2.8% febrile neutropenia.
Not known: Thrombocytopenia G3-4.
Pancytopenia.
Endocrine disorders: Not known: Inappropriate antidiuretic hormone secretion (SIADH).
Metabolism and nutrition disorders: Very common: Anorexia G1-2: 34.5%; G3-4: 4.1%.
Not known: Severe hyponatraemia.
Psychiatric disorders: Common: Insomnia G1-2: 2.8%.
Central nervous system disorders: Very common: Neuro-sensory disorders (G1-2: 11.1%) generally restricted to loss of tendon reflexes and infrequently severe.
Common: Neuromotor disorders, G1-4: 9.2%; G3-4:1.3%.
Headache G1-4 4.1%; G3-4: 0.6%.
Dizziness G1-4: 6%; G3-4: 0.6%.
Altered taste G1-2: 3.8%.
Uncommon: Ataxia, G3: 0.3%.
Eye disorders: Common: Visual impairment, G1-2: 1.3%.
Cardiac disorders: Uncommon: Heart failure and cardiac dysrhythmias.
Not known: Myocardial infarction in patients with history of cardiac disorders or risk factors.
Vascular disorders: Common: Arterial hypertension G1-4 2.5%; G3-4: 0.3%.
Arterial hypotension, G1-4: 2.2%; G3-4: 0.6%.
Respiratory, thoracic and mediastinal disorders: Common: Dyspnoea, G1-4: 2.8%; G3-4: 0.3%.
Cough, G1-2: 2.8%.
Gastro-intestinal disorders: Very common: Nausea, G1-4: 74.7%; G3-4: 7.3%.
Vomiting, G1-4: 54.7%; G3-4: 6.3%; occurrence of nausea and vomiting may be reduced with adjuvant treatment (oral setrons).
Diarrhoea, G1-4: 49.7%; G3-4: 5.7%.
Stomatitis, G1-4: 10.4%; G3-4: 0.9%.
Abdominal pain, G1-4 14.2%.
Constipation G1-4: 19%; G3-4: 0.9%.
It may be appropriate to prescribe laxatives to patients with history of constipation and/or on concomitant treatment with morphine or morphine-mimetics.
Gastric disorders: G1-4: 11.7%.
Common: Oesphagitis, G1-3: 3.8%; G3: 0.3%.
Dysphagia, G1-2: 2.3%.
Uncommon: Paralytic ileus G3-4 (0.9%) [Exceptionally fatal].
Treatment can be restarted as bowel motility has returned to normal.
Not known: Gastrointestinal bleeding.
Hepatobiliary disorders: Common: Hepatic disorders: G1-2: 1.3%.
Not known: Transient elevations of liver function tests.
Skin and subcutaneous tissue disorders: Very common: Alopecia G1-2 (29.4%), generally may occur and is generally mild.
Common: Skin reactions G1-2: 5.7%.
Musculoskeletal and connective tissue disorders: Common: Arthralgia, particularly jaw pain.
Myalgia (G1-4: 7%; G3-4: 0.3%).
Renal and urinary disorders: Common: Dysuria, G1-2: 1.6%.
Other genito-urinary symptom G1-2: 1.9%.
General disorders and administration site abnormalities: Very common: Fatigue/malaise G1-4: 36.7%; G3-4: 8.5%.
Fever, G1-4: 13.0%; G3-4: 12.1%.
Common: Pain, particularly at the site of the tumour. G1-4: 3.8%; G3-4: 0.6%.
Chills: G1-2: 3.8%.
Investigations: Very common: Weight loss G1-4: 25%; G3-4: 0.3%.
Common: Weight gain G1-2: 1.3%.
For the intravenous formulation of Navelbine, the following additional Adverse Drug Reactions were reported: systemic allergic reactions, severe paresthesias, weakness of lower extremities, heart rhythm disorders, flushing, peripheral coldness, collapse, angina pectoris, bronchospasm, interstitial pneumopathy, pancreatitis, palmar-plantar erythrodysesthesia syndrome.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image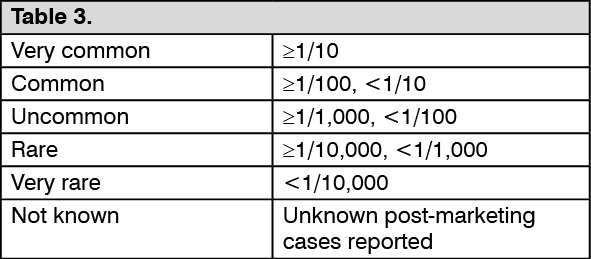 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out