



 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Mechanism of action: The active ingredient of doxorubicin hydrochloride liposome Injection is doxorubicin hydrochloride, a cytotoxic anthracycline antibiotic obtained from Streptomyces peucetius var. caesius. The exact mechanism of the antitumour activity of doxorubicin is not known. It is generally believed that inhibition of DNA, RNA and protein synthesis is responsible for the majority of the cytotoxic effects. This is probably the result of intercalation of the anthracycline between adjacent base pairs of the DNA double helix thus preventing their unwinding for replication.
Clinical efficacy and safety: A phase III randomised study of doxorubicin hydrochloride liposome Injection versus doxorubicin in patients with metastatic breast cancer was completed in 509 patients. The protocol-specified objective of demonstrating non-inferiority between doxorubicin hydrochloride liposome Injection and doxorubicin was met, the hazard ratio (HR) for progression-free survival (PFS) was 1.00 (95% Cl for HR=0.82-1.22). The treatment HR for PFS when adjusted for prognostic variables was consistent with PFS for the ITT population.
The primary analysis of cardiac toxicity showed the risk of developing a cardiac event as a function of cumulative anthracycline dose was significantly lower with doxorubicin hydrochloride liposome Injection than with doxorubicin (HR=3.16, p < 0.001). At cumulative doses greater than 450 mg/m2 there were no cardiac events with doxorubicin hydrochloride liposome Injection.
A phase III comparative study of doxorubicin hydrochloride liposome Injection versus topotecan in patients with epithelial ovarian cancer following the failure of first-line, platinum-based chemotherapy was completed in 474 patients. There was a benefit in overall survival (OS) for doxorubicin hydrochloride liposome Injection-treated patients over topotecan-treated patients as indicated by a hazard ratio (HR) of 1.216 (95% Cl: 1.000; 1.478), p=0.050. The survival rates at 1, 2 and 3 years were 56.3%, 34. 7% and 20.2% respectively on doxorubicin hydrochloride liposome Injection, compared to 54.0%, 23.6% and 13.2% on topotecan.
For the sub-group of patients with platinum-sensitive disease the difference was greater: HR of 1.432 (95% Cl: 1.066; 1.923), p=0.017. The survival rates at 1, 2 and 3 years were 74.1%, 51.2% and 28.4% respectively on doxorubicin hydrochloride liposome Injection, compared to 66.2%, 31.0% and 17.5% on topotecan.
The treatments were similar in the sub-group of patients with platinum-refractory disease: HR of 1.069 (95% Cl: 0.823; 1.387), p=0.618. The survival rates at 1, 2 and 3 years were 41.5%, 21.1% and 13.8% respectively on doxorubicin hydrochloride liposome Injection, compared to 43.2%, 17.2% and 9.5% on topotecan.
A phase III randomised, parallel-group, open-label, multicentre study comparing the safety and efficacy of doxorubicin hydrochloride liposome Injection plus bortezomib combination therapy with bortezomib monotherapy in patients with multiple myeloma who have received at least 1 prior therapy and who did not progress while receiving anthracycline-based therapy, was conducted in 646 patients. There was a significant improvement in the primary endpoint of time to progression (TTP) for patients treated with combination therapy of doxorubicin hydrochloride liposome Injection plus bortezomib compared to patients treated with bortezomib monotherapy as indicated by a risk reduction (RR) of 35% (95% Cl: 21-47%), p < 0.0001, based on 407 TTP events. The median TTP was 6.9 months for the bortezomib monotherapy patients compared with 8.9 months for the doxorubicin hydrochloride liposome Injection plus bortezomib combination therapy patients. A protocol-defined interim analysis (based on 249 TTP events) triggered early study termination for efficacy. This interim analysis showed a TTP risk reduction of 45% (95% Cl: 29-57%), p < 0.0001. The median TTP was 6.5 months for the bortezomib monotherapy patients compared with 9.3 months for the doxorubicin hydrochloride liposome Injection plus bortezomib combination therapy patients. These results, though not mature, constituted the protocol defined final analysis. The final analysis for overall survival (OS) performed after a median follow-up of 8.6 years showed no significant difference in OS between the two treatment arms. The median OS was 30.8 months (95% Cl; 25.2-36.5 months) for the bortezomib monotherapy patients and 33.0 months (95% Cl; 28.9-37.1 months) for the doxorubicin hydrochloride liposome Injection plus bortezomib combination therapy patients.
Pharmacokinetics: Doxorubicin hydrochloride liposome Injection is a long-circulating pegylated liposomal formulation of doxorubicin hydrochloride. Pegylated liposomes contain surface-grafted segments of the hydrophilic polymer methoxypolyethylene glycol (MPEG). These linear MPEG groups extend from the liposome surface creating a protective coating that reduces interactions between the lipid bilayer membrane and the plasma components. This allows the doxorubicin hydrochloride liposome Injection liposomes to circulate for prolonged periods in the blood stream. Pegylated liposomes are small enough (average diameter of approximately 100 nm) to pass intact (extravasate) through defective blood vessels supplying tumours. Evidence of penetration of pegylated liposomes from blood vessels and their entry and accumulation in tumours has been seen in mice with C-26 colon carcinoma tumours and in transgenic mice with KS-like lesions. The pegylated liposomes also have a low permeability lipid matrix and internal aqueous buffer system that combine to keep doxorubicin hydrochloride encapsulated during liposome residence time in circulation.
The plasma pharmacokinetics of doxorubicin hydrochloride liposome Injection in humans differ significantly from those reported in the literature for standard doxorubicin hydrochloride preparations. Al lower doses (10 mg/m2-20 mg/m2) doxorubicin hydrochloride liposome Injection displayed linear pharmacokinetics. Over the dose range of 10 mg/m2-60 mg/m2 doxorubicin hydrochloride liposome Injection displayed non-linear pharmacokinetics. Standard doxorubicin hydrochloride displays extensive tissue distribution (volume of distribution: 700 to 1,100 l/m2) and a rapid elimination clearance (24 to 73 l/h/m2). In contrast, the pharmacokinetic profile of doxorubicin hydrochloride liposome Injection indicates that doxorubicin hydrochloride liposome Injection is confined mostly to the vascular fluid volume and that the clearance of doxorubicin from the blood is dependent upon the liposomal carrier. Doxorubicin becomes available after the liposomes are extravasated and enter the tissue compartment.
At equivalent doses, the plasma concentration and AUG values of doxorubicin hydrochloride liposome Injection which represent mostly pegylated liposomal doxorubicin hydrochloride (containing 90% to 95% of the measured doxorubicin) are significantly higher than those achieved with standard doxorubicin hydrochloride preparations.
Doxorubicin hydrochloride liposome Injection should not be used interchangeably with other formulations of doxorubicin hydrochloride.
Population pharmacokinetics: The pharmacokinetics of doxorubicin hydrochloride liposome Injection was evaluated in 120 patients from 10 different clinical trials using the population pharmacokinetic approach. The pharmacokinetics of doxorubicin hydrochloride liposome Injection over the dose range of 10 mg/m2 to 60 mg/m2 was best described by a two compartment non-linear model with zero order input and Michaelis-Menten elimination. The mean intrinsic clearance of doxorubicin hydrochloride liposome Injection was 0.030 l/h/m2 (range 0.008 to 0.152 l/h/m2) and the mean central volume of distribution was 1.93 l/m2 (range 0.96-3.85 l/m2) approximating the plasma volume. The apparent half-life ranged from 24-231 hours, with a mean of 73.9 hours.
Breast cancer patients: The pharmacokinetics of doxorubicin hydrochloride liposome Injection determined in 18 patients with breast carcinoma were similar to the pharmacokinetics determined in the larger population of 120 patients with various cancers. The mean intrinsic clearance was 0.016 l/h/m2 (range 0.008-0.027 I/him the mean central volume of distribution was 1.46 I/m2 (range 1.10-1.64 l/m2). The mean apparent half-life was 71.5 hours (range 45.2-98.5 hours).
Ovarian cancer patients: The pharmacokinetics of doxorubicin hydrochloride liposome Injection determined in 11 patients with ovarian carcinoma were similar to the pharmacokinetics determined in the larger population of 120 patients with various cancers. The mean intrinsic clearance was 0.021 l/h/m2 (range 0.009-0.041 l/h/m2), the mean central volume of distribution was 1.95 l/m2 (range 1.67-2.40 l/m2). The mean apparent half-life was 75.0 hours (range 36.1-125 hours).
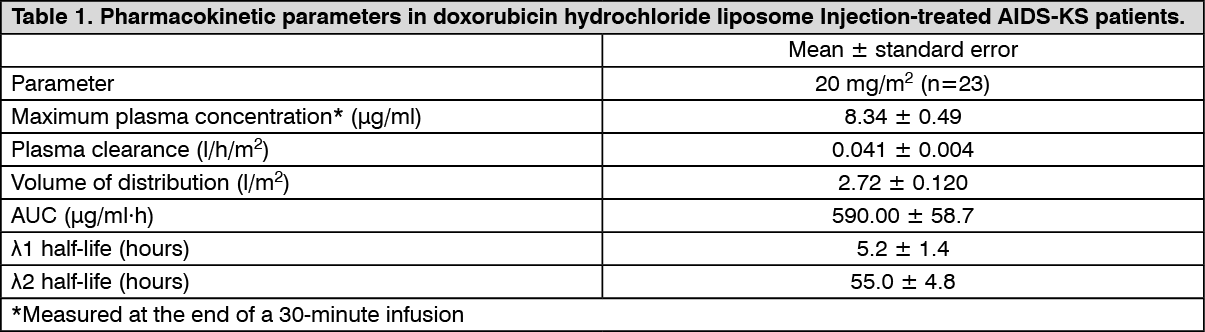
AIDS-related KS patients: The plasma pharmacokinetics of doxorubicin hydrochloride liposome Injection were evaluated in 23 patients with KS who received single doses of 20 mg/m2 administered by a 30-minute infusion. The pharmacokinetic parameters of doxorubicin hydrochloride liposome Injection (primarily representing pegylated liposomal doxorubicin hydrochloride and low levels of unencapsulated doxorubicin hydrochloride) observed after the 20 mg/m2 doses are presented in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageToxicology: Preclinical safety data: In repeat dose studies conducted in animals, the toxicity profile of doxorubicin hydrochloride liposome Injection appears very similar to that reported in humans who receive long-term infusions of standard doxorubicin hydrochloride. With doxorubicin hydrochloride liposome Injection, the encapsulation of doxorubicin hydrochloride in pegylated liposomes results in these effects having a differing strength, as follows.
Cardiotoxicity: Studies in rabbits have shown that the cardiotoxicity of doxorubicin hydrochloride liposome Injection is reduced compared with conventional doxorubicin hydrochloride preparations.
Dermal toxicity: In studies performed after the repealed administration of doxorubicin hydrochloride liposome Injection to rats and dogs, serious dermal inflammations and ulcer formations were observed at clinically relevant dosages. In the study in dogs, the occurrence and severity of these lesions was reduced by lowering the dose or prolonging the intervals between doses. Similar dermal lesions, which are described as palmar-plantar erythrodysesthesia were also observed in patients after long-term intravenous infusion (see Adverse Reactions).
Anaphylactoid response: During repeat dose toxicology studies in dogs, an acute response characterised by hypotension, pale mucous membranes, salivation, emesis and periods of hyperactivity followed by hypoactivity and lethargy was observed following administration of pegylated liposomes (placebo). A similar, but less severe response was also noted in dogs treated with doxorubicin hydrochloride liposome Injection and standard doxorubicin.
The hypotensive response was reduced in magnitude by pretreatment with antihistamines. However, the response was not life-threatening and the dogs recovered quickly upon discontinuation of treatment.
Local toxicity: Subcutaneous tolerance studies indicate that doxorubicin hydrochloride liposome Injection, as against standard doxorubicin hydrochloride, causes slighter local irritation or damage to the tissue after a possible extravasation.
Mutagenicity and carcinogenicity: Although no studies have been conducted with doxorubicin hydrochloride liposome Injection, doxorubicin hydrochloride, the pharmacologically active ingredient of doxorubicin hydrochloride liposome Injection, is mutagenic and carcinogenic. Pegylated placebo liposomes are neither mutagenic nor genotoxic.
Reproductive toxicity: Doxorubicin hydrochloride liposome Injection resulted in mild to moderate ovarian and testicular atrophy in mice after a single dose of 36 mg/kg. Decreased testicular weights and hypospermia were present in rats after repeat doses ≥ 0.25 mg/kg/day and diffuse degeneration of the seminiferous tubules and a marked decrease in spermatogenesis were observed in dogs after repeat doses of 1 mg/kg/day (see Use in Pregnancy & Lactation).
Nephrotoxicity: A study has shown that doxorubicin hydrochloride liposome Injection at a single intravenous dose of over twice the clinical dose produces renal toxicity in monkeys. Renal toxicity has been observed with even lower single doses of doxorubicin HCl in rats and rabbits. Since an evaluation of the post-marketing safety database for doxorubicin hydrochloride liposome Injection in patients has not suggested a significant nephrotoxicity liability of doxorubicin hydrochloride liposome Injection, these findings in monkeys may not have relevance to patient risk assessment.