Gastrointestinal Disorders: Diarrhea, nausea, stomatitis, vomiting, abdominal pain, constipation, upper abdominal pain, dyspepsia; GI motility disorder, oral discomfort, Upper GI inflammatory disorder, GI haemorrhage, ileus; dry mouth.
Skin and Subcutaneous Tissue Disorders: Hand and foot syndrome, alopecia, rash, erythema, dermatitis, skin discoloration, nail disorder, rash erythematous, nail discoloration, onycholysis, pruritus.
General Disorders and Administration Site Conditions: Fatigue, pyrexia, asthenia, lethargy, fatigue, weakness, chest pain, pain in limb, influenza like illness.
Nervous System Disorders: Dizziness, headache, dysgeusia, peripheral sensory neuropathy, insomnia, paresthesia, hypoaesthesia.
Metabolism and Nutrition Disorders: Anorexia, appetite decreased, dehydration, weight decreased.
Eye Disorders: Conjunctivitis, eye irritation, abnormal vision, increased lacrimation.
Blood and lymphatic system disorders: Neutropenia, anemia, neutropenic fever, thrombocytopenia, lymphocytopenia, granulocytopenia.
Respiratory thoracic and mediastinal disorders: Epistaxis, dyspnea, cough, pharyngeal disorder, sore throat, rhinorrhea, pleural effusion.
Musculoskeletal: Back pain, Arthralgia, myalgia, bone pain.
Vascular: Venous thrombosis, flushing, lymphoedema.
Psychiatric: Mood alteration, depression.
Infection: Viral, oral candidiasis, urinary tract infection, upper respiratory tract infection.





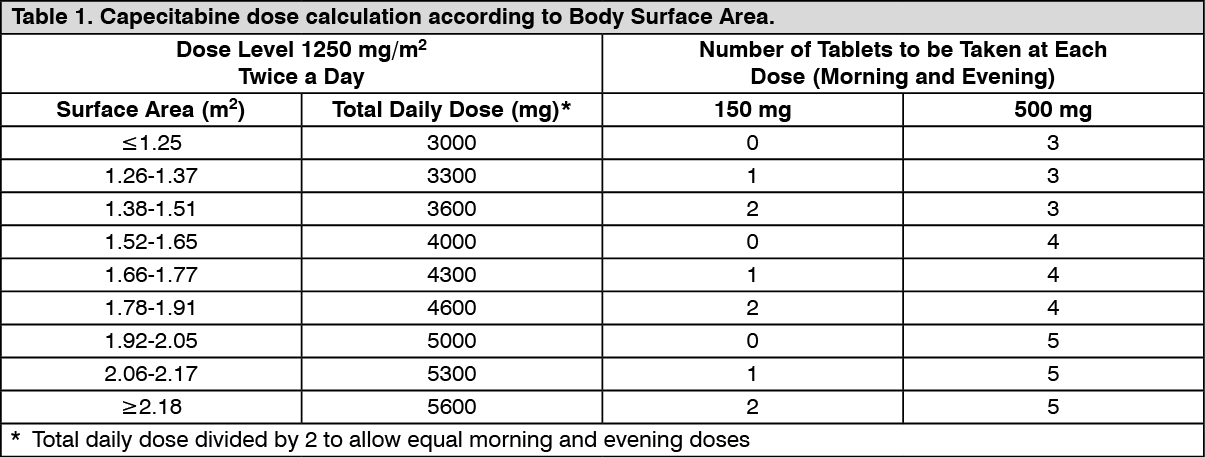 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image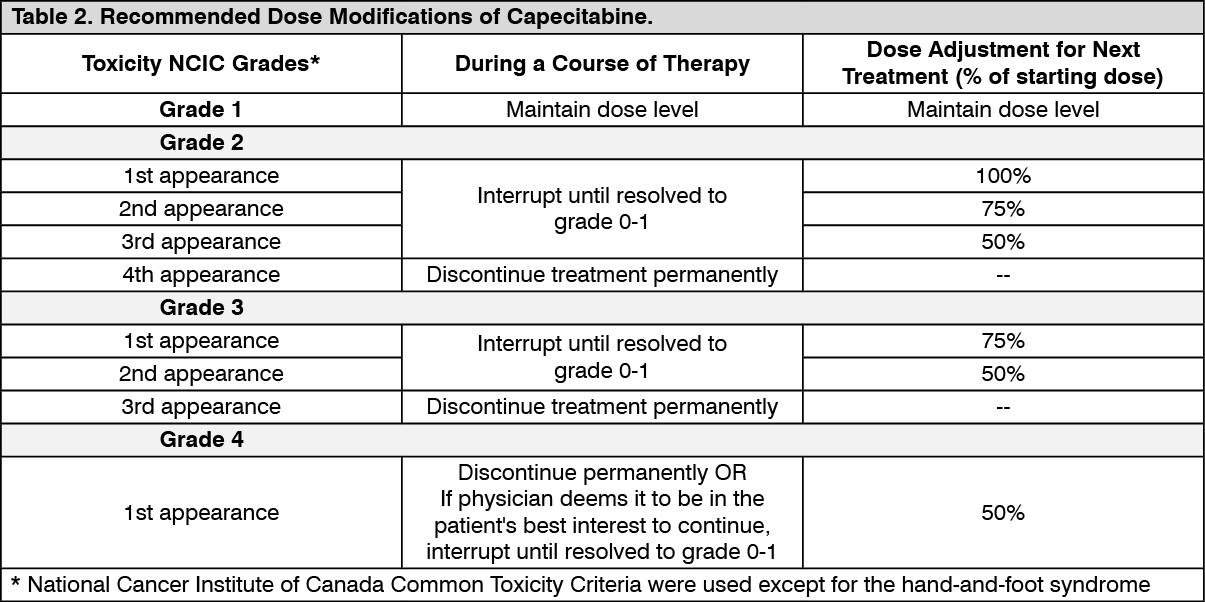 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image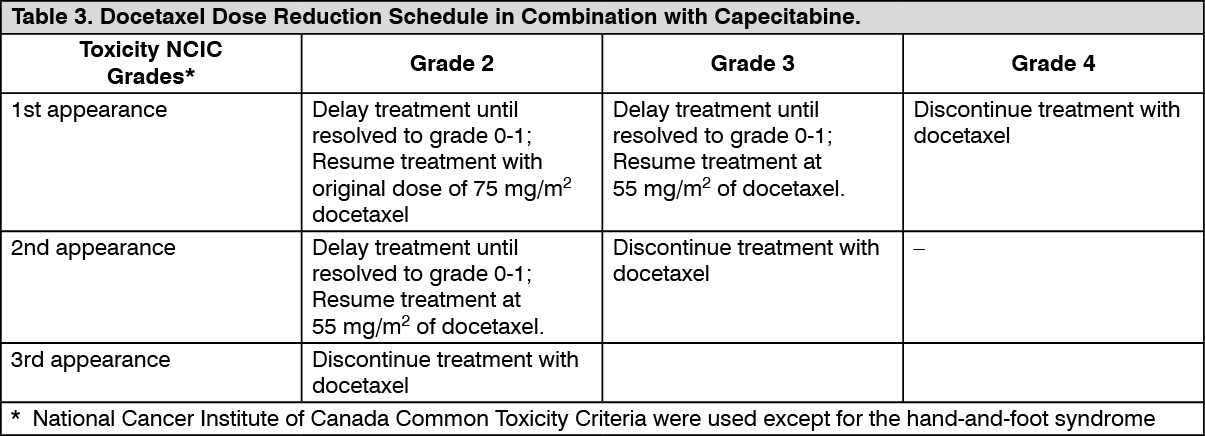 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out