Pharmacotherapeutic group: immunosuppressant. (
ATC code: L04 A A06).
Pharmacology: Mechanism of Action: MPA inhibits the proliferation of T- and B lymphocytes more potently than other cells because in contrast to other cell types that can utilize purine salvage pathways the lymphocyte proliferation is critically dependent on de novo synthesis. Thus the mode of action is complementary to calcineurin inhibitors which interfere with cytokine transcription and resting T-lymphocytes.
Clinical Studies: Two multi-center randomized, double-blind pivotal trials were used for mycophenolic acid (MPA) approval in adults. Both studies were reference therapy-controlled clinical studies using commercially marketed MMF (Cellcept) as the comparator. Both studies demonstrated comparable efficacy and safety to MMF. The first study included 423 adult de novo renal transplants (ERLB301) and demonstrated that MPA was equivalent to MMF in efficacy and had a comparable safety profile. The second study was conducted in 322 maintenance kidney transplant recipients (ERLB302) and demonstrated that renal transplant patients receiving MMF maintenance immunosuppressive therapy could be safely converted to MPA without compromising efficacy.
De novo adult renal transplant patients (study ERL B301):
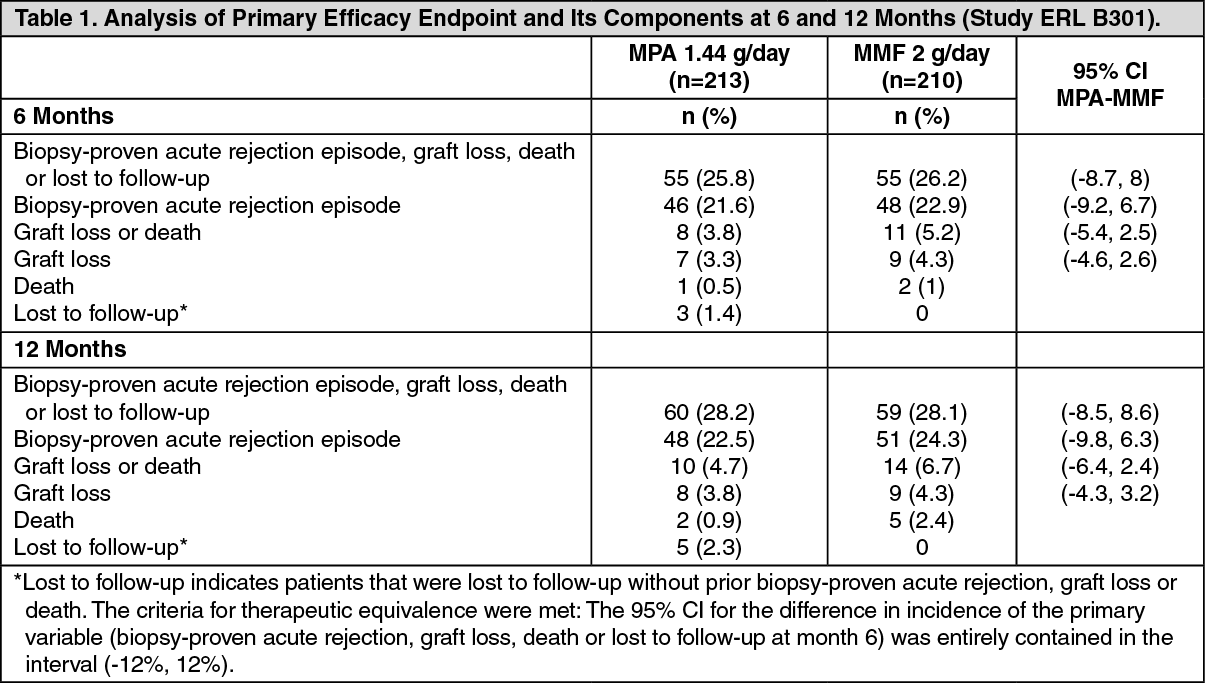
The double-blind, double-dummy randomized de novo study (ERLB301) was conducted in 423 renal transplant patients (MPA=213, MMF=210), aged 18-75 years, and was designed prospectively to test therapeutic equivalence of MPA to MMF as measured by the incidence of efficacy failure (i.e., biopsy proven acute rejection (BPAR), graft loss, death or loss to follow up) within the first 6 months of treatment (primary endpoint) and by the incidence of death, graft loss or loss to follow-up at 12 months (co-primary endpoint).
Patients were administered either MPA 1.44 g/day or MMF 2 g/day within 48 hours post-transplant for 12 months in combination with cyclosporine, and corticosteroids. In the MPA and MMF groups, 39.4% and 42.9%, respectively, received antibody therapy as an induction treatment.
Based on the incidence of efficacy failure at 6 months (MPA 25.8% vs. MMF 26.2%; 95% CI: [-8.7, +8.0]) therapeutic equivalence was demonstrated. At 12 months, the incidence of BPAR, graft loss or death was 26.3% and 28.1%, and incidence of BPAR alone was 22.5% and 24.3% for MPA and MMF, respectively. Among those with BPAR, the incidence of severe acute rejection was 2.1% with MPA and 9.8% with MMF (p=ns). (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The overall safety and hematologic profiles were similar between the two treatment groups. Drug-suspected AEs were 51.1% and 60.5% in the MPA vs. MMF groups, respectively. No difference in overall incidence of infection was observed. The overall incidence of serious infections was 22.1% in the MPA group and 27.1% in the MMF group. The incidence of serious pneumonia was lower in the MPA group (0.5% vs 4.3%, p=0.01). No difference in the overall incidence of GI AEs was observed (80.8% vs. 80%, p=ns, MPA vs. MMF, respectively).
Maintenance adult renal transplant patients (study ERL B302):
The maintenance study was conducted in 322 renal transplant patients (MPA=159, MMF=163), aged 18 to 75 years, who were at least 6 months post-transplant receiving 2 g/day MMF in combination with cyclosporine, with or without corticosteroids for at least four weeks prior to entry in the study. Patients were randomized 1:1 to MPA 1.44 g/day or MMF 2 g/day for 12 months. The efficacy endpoint was the incidence of efficacy failure (i.e., BPAR, graft loss, or death) at 6 and 12 months.
At 12 months, similar rates of efficacy failure (MPA 2.5%; MMF 6.1%; p=ns), biopsy-proven acute rejection (MPA 1.3%; MMF 3.1%; p=ns) and biopsy-proven chronic rejection (MPA 3.8%; MMF 4.9%; p=ns) were observed in both groups. (See Table 2.)
Click on icon to see table/diagram/image
The maintenance study also demonstrated an overall similar safety profile, with the exception of the incidence of serious infections (8.8 vs 16%, p<0.05, MPA vs. MMF). The incidence of overall infections was 59% in each group. Less pneumonia was observed in the MPA group (1.9%) than the MMF group (4.9%), but it was not statistically significant. A similar incidence of overall GI AEs was observed (69.2 vs 61.8%, MPA vs. MMF), although "any GI AE" was numerically higher in the MPA-treated patients up to 12 months (29.6% vs. 24.5% at month 12), and the increase in GI severity tended to be lower in MPA patients.
Pharmacokinetics: Absorption: Following oral administration, mycophenolate sodium is extensively absorbed. Consistent with its enteric coated design, the time to maximal MPA concentration was approximately 1.5 to 2 hours. In vitro
studies demonstrated that the enteric coated mycophenolic acid (Myfortic) formulation -prevents the release of MPA under acidic conditions as in the stomach.
In stable renal transplant patients on ciclosporin for microemulsion based immunosuppression, the gastrointestinal absorption of MPA was 93% and the absolute bioavailability was 72%. Mycophenolic acid pharmacokinetics are dose proportional and linear over the studied dose range of 180 to 2,160 mg. Compared to the fasting state, administration of 720 mg mycophenolic acid (Myfortic) with a high fat meal (55 g fat, 1,000 calories) had no effect on the systemic exposure of MPA (AUC) which is the most relevant PKparameter linked to efficacy. However there was a 33% decrease in the maximal concentration of MPA (C
max).
Distribution: The volume of distribution of MPA at steady state is 50 liters. Both mycophenolic acid and mycophenolic acid glucuronide are highly protein bound, 97% and 82%, respectively. The free MPA concentration may increase under conditions of decreased protein binding sites (uremia, hepatic failure, hypoalbuminemia, concomitant use of drugs with high protein binding). This may put patients at increased risk of MPA-related adverse effects.
Biotransformation/ Metabolism: The half-life of MPA is 11.7 hours and the clearance is 8.6 L/hr. MPA is metabolized principally by glucuronyl transferase to form the phenolic glucuronide of MPA, mycophenolic acid glucuronide (MPAG) MPAG is the predominant metabolite of MPA and does not manifest biologic activity. In stable renal transplant patients on ciclosporin for microemulsion based immunosuppression, approximately 28% of the oral mycophenolic acid (Myfortic) dose is converted to MPAG by presystemic metabolism. The half-life of MPAG is longer than that of MPA, approximately 15.7 hours and its clearance is 0.45 L/hr.
Elimination: Although negligible amounts of MPA are present in the urine (<1.0%), the majority of MPA is eliminated in the urine as MPAG. MPAG secreted in the bile is available for deconjugation by gut flora. The MPA resulting from this deconjugation may then be reabsorbed. Approximately 6 to 8 hours after mycophenolic acid (Myfortic) dosing a second peak of MPA concentration can be measured, consistent with reabsorption of the deconjugated MPA.
Pharmacokinetics in renal transplant patients on ciclosporin for microemulsion based immunosuppression:
Table 3 as follows shows mean pharmacokinetic parameters for MPA following mycophenolic acid (Myfortic) administration. Single dose pharmacokinetics predicts multiple dose and chronic dosing pharmacokinetics. In the early post-transplant period, mean MPA AUC and mean MPA C
max was approximately one-half of that measured six months post-transplant. (See Table 3.)
Click on icon to see table/diagram/image
Special Populations: Renal impairment: MPA pharmacokinetic appeared to be unchanged over the range of normal to absent renal function. In contrast, MPAG exposure increased with decreased renal function; MPAG exposure being approximately 8 fold higher in the setting of anuria. Clearance of either MPA or MPAG was unaffected by hemodialysis. Free MPA may also significantly increase in the setting of renal failure. This may be due to decreased MPA plasma protein binding in the presence of high blood urea concentration.
Hepatic impairment: In volunteers with alcoholic cirrhosis, hepatic MPA glucuronidation processes were relatively unaffected by hepatic parenchymal disease. Effects of hepatic disease on this process probably depend on the particular disease. However, hepatic disease with predominantly biliary damage, such as primary biliary cirrhosis, may show a different effect.
Pediatric population (below 18 years):
Safety and efficacy in children have not been established. Limited pharmacokinetics data are available on the use of mycophenolic acid (Myfortic) in children. In the table previously mentioned, mean (SD) MPA pharmacokinetics are shown for stable pediatric renal transplant patients on ciclosporin microemulsion based immunosuppression. Increased variability of MPA C
max and AUC were noted in these pediatric patients compared to adult renal transplant patients. Mean MPA AUC at this dose was higher than typically measured in adults receiving 720 mg. The mean apparent MPA clearance was approximately 7.7 L/hr. A dose of 200 to 300 mg/m
2 would be expected to result in a MPA AUC of 30 to 50 micrograms hr/mL.
Gender: There are no clinically significant gender differences in mycophenolic acid (Myfortic) pharmacokinetics.
Geriatric population (65 years of age or above): Based on preliminary data MPA exposure does not appear to vary to a clinically significant degree by age.
Race/ethnicity: Following a single dose administration of 720 mg mycophenolic acid (Myfortic) to 18 healthy Japanese and Caucasian subjects, the exposure (AUC
inf) for MPA and MPAG were 15 and 22% lower in Japanese subjects compared to Caucasians. The peak MPAG concentrations (C
max) were similar between the two populations, however, Japanese subjects had 9.6% higher C
max for MPA. These results do not suggest any clinically relevant differences.
Toxicology: Non-Clinical Safety Data: Carcinogenicity and mutagenicity: In a 104-week oral carcinogenicity study in rats, mycophenolate sodium at daily doses up to 9 mg/kg was not tumorigenic. The highest dose tested resulted in approximately 0.6 to 1.2 times the systemic exposure observed in renal transplant patients at the recommended dose of 1440 mg/day. Similar results were observed in a parallel study in rats performed with mycophenolate mofetil. In a 26-week oral carcinogenicity assay in a P53± (heterozygous) transgenic mouse model, mycophenolate sodium at daily doses up to 200 mg/kg was not tumorigenic. The highest dose tested was 200 mg/kg, resulting in approximately 5 times the systemic exposure observed in renal transplant patients (1440 mg/day).
The genotoxic potential of mycophenolate sodium was determined in five assays. MPA was genotoxic in the mouse lymphoma/thymidine kinase assay, the micronucleus test in V79 Chinese hamster cells and the in vivo mouse micronucleus assay. Mycophenolate sodium was not genotoxic in the bacterial mutation assay or the chromosomal aberration assay in human lymphocytes. The lowest dose showing genotoxic effects in a mouse bone marrow micronucleus resulted in approximately 3 times the systemic exposure (AUC or C
max) observed in renal transplant patients at the tested clinical dose of 1440 mg of mycophenolic acid per day. It is probable that the mutagenic activity observed was due to a shift in the relative abundance of the nucleotides in the cellular pool used for DNA synthesis.
Fertility: Mycophenolate sodium had no effect on male rats fertility at oral doses up to 40 mg/kg/day. The systemic exposure at this dose represents approximately 9 times the clinical exposure at the tested clinical MRHD of 1440 mg mycophenolic acid (Myfortic) per day. No effects on female fertility were seen up to a dose of 20 mg/kg/day, a dose at which maternal toxicity and embryotoxicity were already observed.
Safety pharmacology and repeat dose toxicity: The hematopoietic and lymphoid systems were the primary organs affected in toxicology studies conducted with mycophenolate sodium in rats and mice. Aplastic, regenerative anemia was identified as the dose-limiting toxicity in MPA-exposed rodents. Evaluation of myelograms showed a marked decrease in erythroid cells (polychromatic erythroblasts and normoblasts) and a dose-dependent spleen enlargement and increase in extramedullary hematopoiesis. These effects occurred at systemic exposure levels which are equivalent to or less than the clinical exposure at the recommended dose of 1440 mg/day mycophenolic acid in renal transplant patients.
The non-clinical toxicity profile of mycophenolate sodium appears to be consistent with adverse events observed in MPA-exposed humans, which now provide safety data of more relevance to the patient population (see ADVERSE REACTIONS).
Single oral doses of MPA are moderately well tolerated in rats (LD50 of 350 to 700 mg/kg), well tolerated in mice or monkeys (LD50 of more than 1,000 mg/kg), and extremely well tolerated in rabbits (LD50 of more than 6,000 mg/kg).
Reproductive toxicity: For information on reproductive toxicity, see USE IN PREGNANCY & LACTATION.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image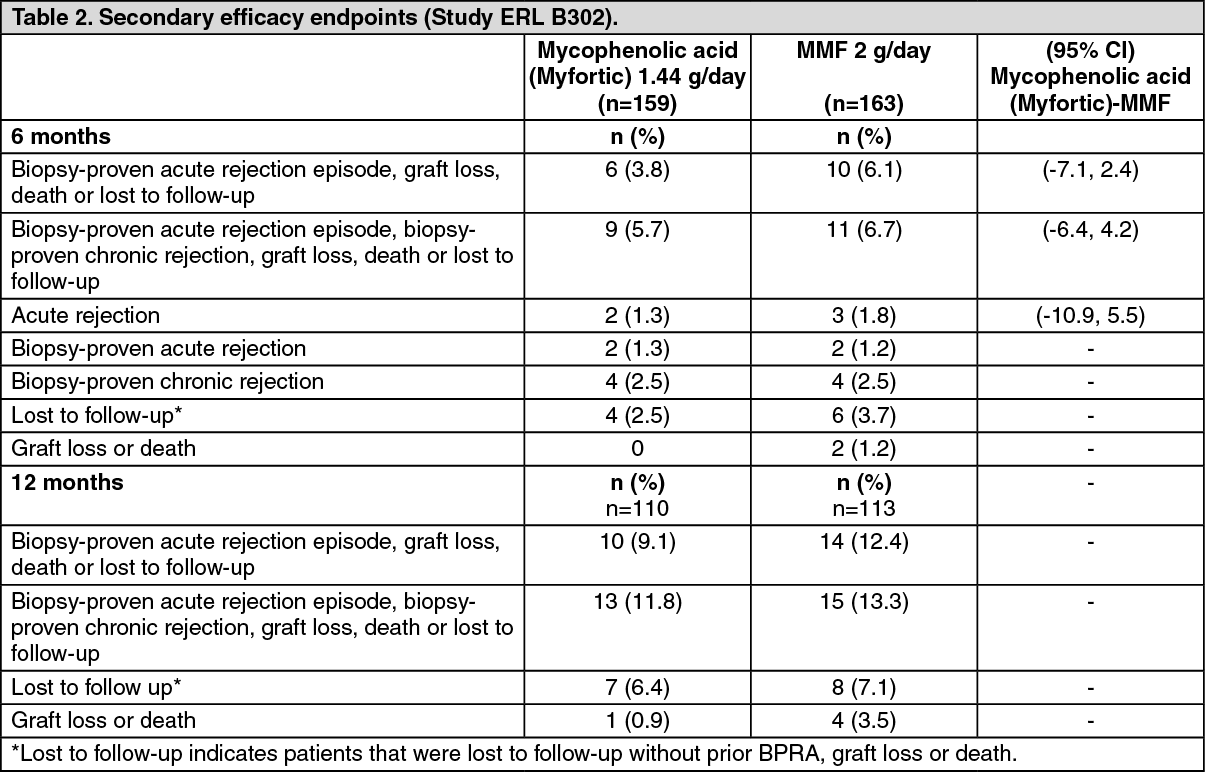 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image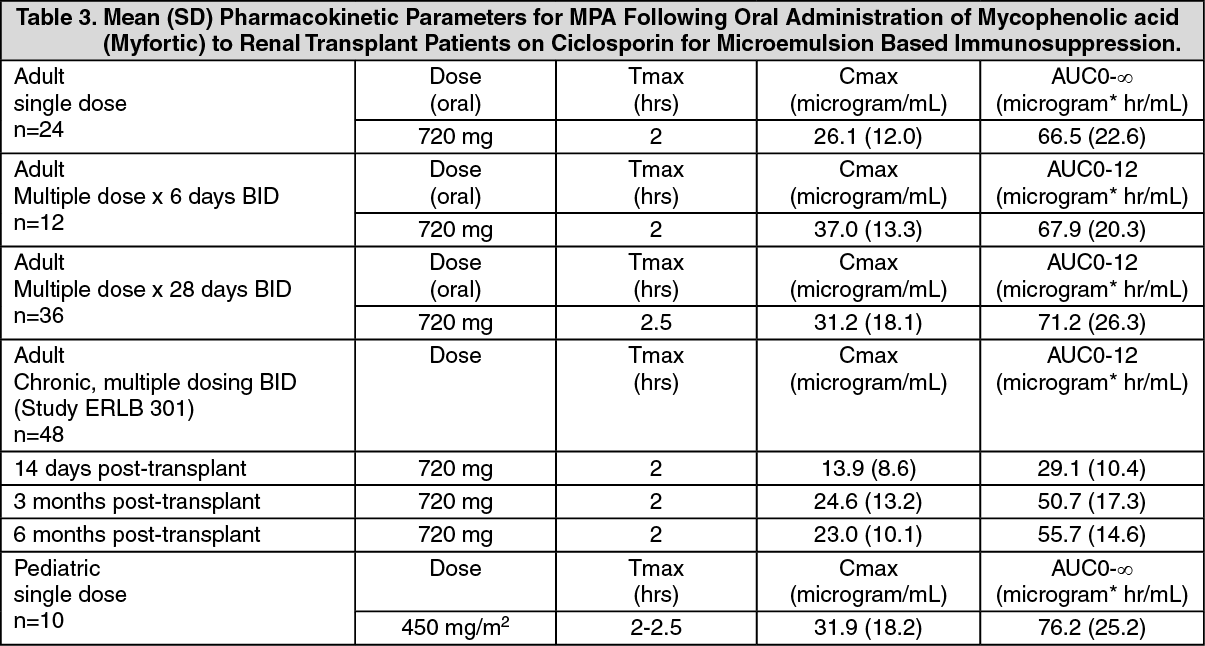 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image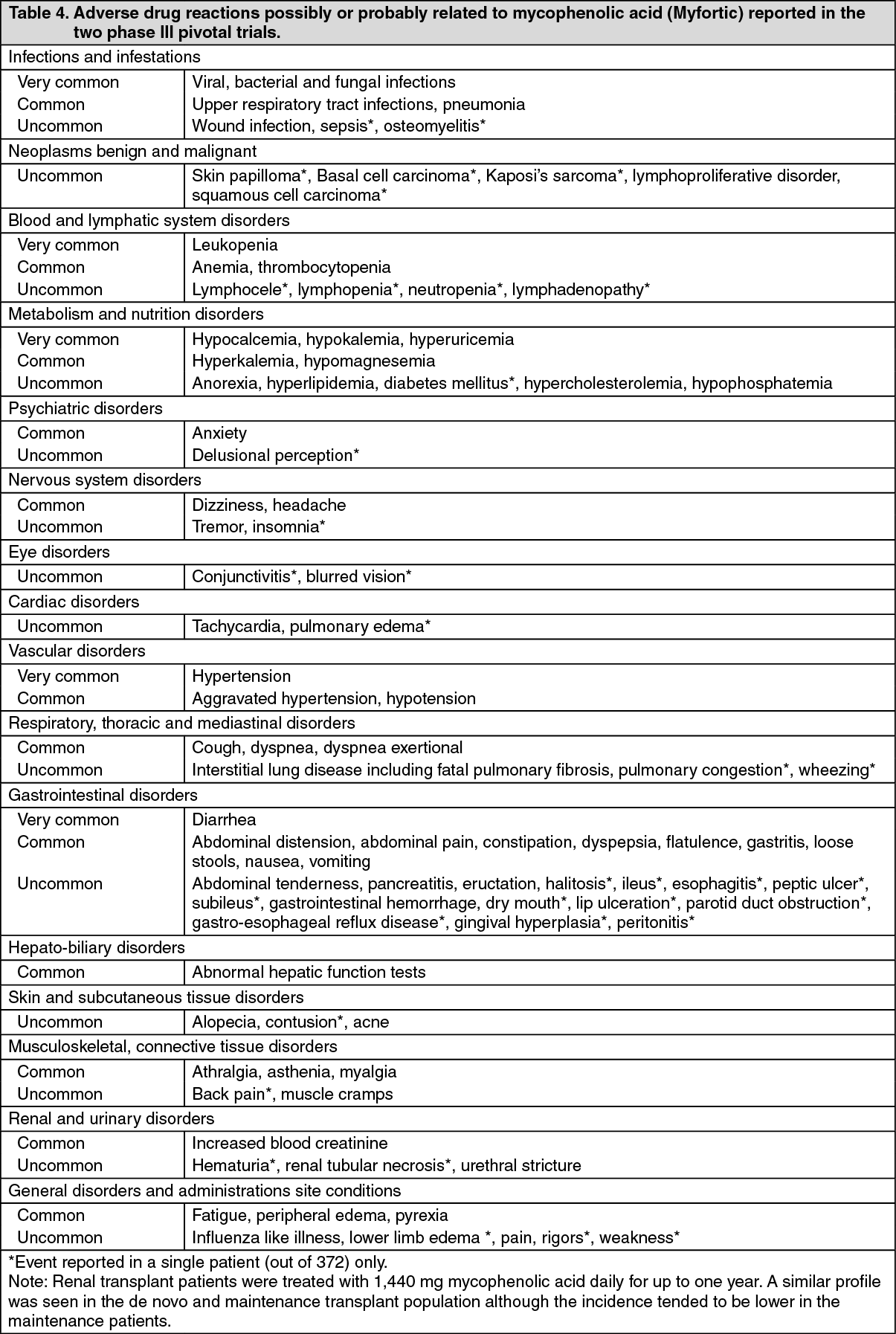 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out