Letrozole tablet was generally well tolerated across all studies as first-line and second-line treatment for breast cancer and adverse reaction rates were similar in both settings.
Adjuvant Treatment of Early Breast Cancer: Adverse reactions are mentioned as follows: Hypercholesterolemia, Hot Flashes/Flushes, Arthralgia/Arthritis, Night Sweats, Bone Fractures, Weight Increase, Nausea, Bone Fractures, Fatigue (Lethargy, Malaise, Asthenia), Myalgia, Edema, Weight Decrease, Vaginal Bleeding, Back Pain, Osteoporosis NOS, Bone Pain, Depression, Vaginal Irritation, Headache, Pain in extremity, Osteopenia, Dizziness/Light-Headedness, Alopecia, Vomiting, Cataract, Constipation, Breast pain, Anorexia, Endometrial Hyperplasia/Cancer, Endometrial Proliferation Disorders, Endometrial Hyperplasia/Cancer, Other Endometrial Disorders, Myocardial Infarction, Myocardial Ischemia, Cerebrovascular Accident, Angina, Thromboembolic Event, Other Cardiovascular, Second Malignancies.
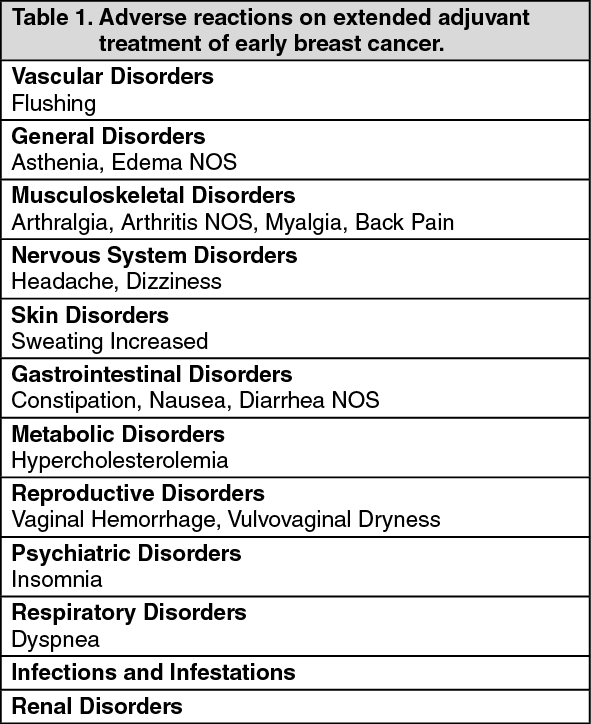
Extended Adjuvant Treatment of Early Breast Cancer: Adverse reactions are seen in the following table: See Table 1.
 Click on icon to see table/diagram/image
First-line breast cancer:
Click on icon to see table/diagram/image
First-line breast cancer: The most frequently reported adverse experiences were bone pain, hot flushes, back pain, nausea, arthralgia, dyspnea. Adverse events with Letrozole Tablets 2.5 mg are shown in the following table: See Table 2.
Click on icon to see table/diagram/image
Other less frequent (<2%) adverse experiences considered consequential for both treatment groups, included peripheral thromboembolic events, cardiovascular events, and cerebrovascular events. Peripheral thromboembolic events included venous thrombosis, thrombophlebitis, portal vein thrombosis and pulmonary embolism. Cardiovascular events included angina, myocardial infarction, myocardial ischemia, and coronary heart disease. Cerebrovascular events included transient ischemic attacks, thrombotic or hemorrhagic strokes and development of hemiparesis.
Second-line breast cancer: Adverse reactions are shown in the following table: See Table 3.
Click on icon to see table/diagram/image



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image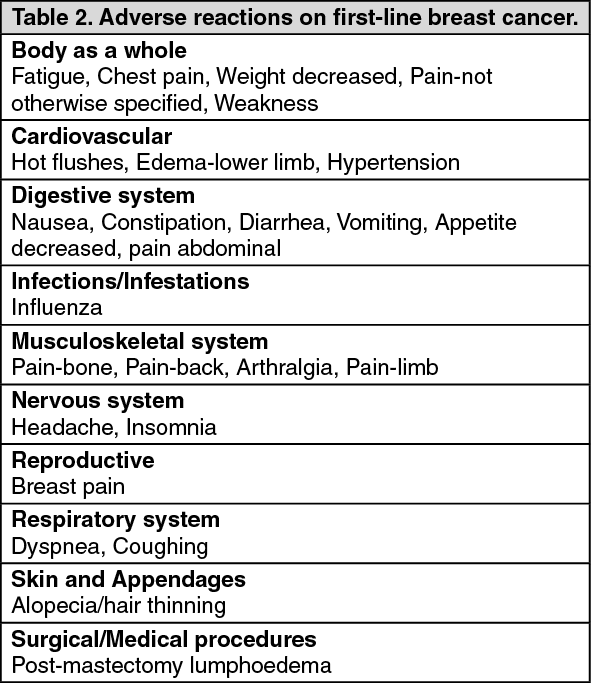 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image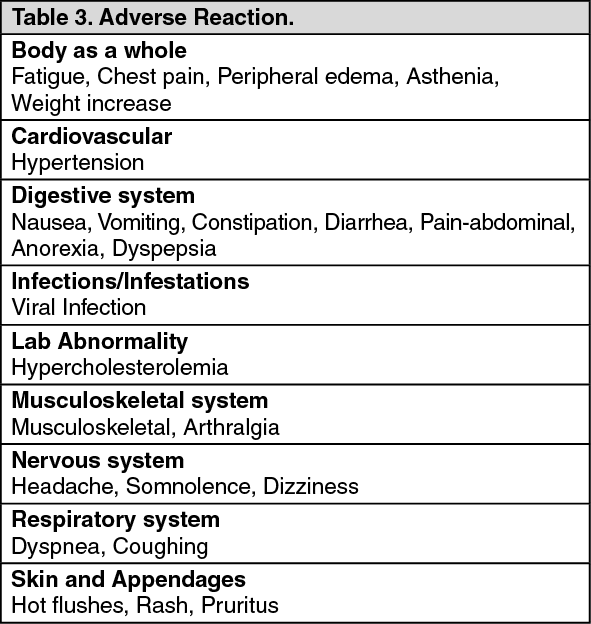 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out