



 Sign Out
Sign Out
CHILDREN 2 to 12 years: Initial dose is 300 mcg/kg bodyweight daily in 1 or 2 divided doses for 2 weeks followed by 600 mcg/kg body weight in 2 divided doses for 2 weeks; thereafter the dose is increased by 600 mcg/kg body weight daily every 1 to 2 weeks to usual maintenance dose of 4.5 to 7.5 mg/kg body weight daily (maximum of 300 mg daily in 2 divided doses). Maintenance dose in patients less than 30 kg may need to be increased by as much as 50%, based on clinical response. Or as prescribed by the physician.
Add on therapy (without valproate): ADULTS: 50 mg once daily for 2 weeks followed by 50 mg twice daily for 2 weeks, thereafter, the dose is increased by 100 mg/day every 1 to 2 weeks to usual maintenance doses of 300 to 500 mg daily given in 2 divided doses.
CHILDREN 2 to 12 years: Initial dose is 600 mcg/kg body weight daily in 2 divided doses for 2 weeks followed by 1.2 mg/kg body weight in two divided doses for 2 weeks; thereafter the dose is increased by a maximum of 1.2 mg/kg body weight every 1 to 2 weeks to a usual maintenance dose of 5 to 15 mg/kg body weight (maximum 400 mg/day) given in 2 divided doses. Maintenance dose in patients less than 30 kg may need to be increased by as much as 50%, based on clinical response. Or as prescribed by the physician.
Add on therapy (with valproate): ADULTS: Initial dose is 25 mg every other day for 2 weeks followed by 25 mg once daily for 2 weeks; thereafter the dose is increased by 25 to 50 mg/day every 1 to 2 weeks to usual maintenance doses of 100 to 200 mg daily with valproate alone and 100 to 400 mg daily with valproate and other drugs that induce glucuronidation, given as a single dose or in 2 divided doses.
CHILDREN: Initial dose is 150 mcg/kg body weight once daily for 2 weeks followed by 300 mcg/kg once daily for 2 weeks, thereafter the dose is increased by 300 mcg/kg every 1 to 2 weeks to usual maintenance dose of 1 mg to 5 mg/kg body weight (maximum 200 mg/day in 1 or 2 divided doses) which may be given once daily or in 2 divided doses and 1 mg to 3 mg/kg/day for those patients taking valproate alone as an add on. Maintenance dose in patients less than 30kg may need to be increased by as much as 50%, based on clinical response. Or as prescribed by the physician.
NOTE: If the calculated dose for children lies between 1 and 2 mg then 2 mg may be given on alternate days for the first 2 weeks of therapy. Lamotrigine should not be administered if the calculated dose is less than 1 mg.
Usual Adjunctive Maintenance Dose: In patients receiving multidrug regimens employing carbamazepine, phenytoin, phenobarbital or primidone without valproate, maintenance doses of adjunctive lamotrigine as high as 700 mg/day have been used. In patients receiving valproate alone, maintenance doses of adjunctive lamotrigine as high as 200 mg/day have been used.
Conversion from Adjunctive Therapy to Monotherapy: The goal of the transition regimen is to attempt to maintain seizure control while mitigating the risk of serious rash associated with the rapid titration of lamotrigine.
The recommended maintenance dose of lamotrigine as monotherapy is 500 mg/day given in 2 divided doses.
To avoid an increased risk of rash, the recommended initial dose and subsequent dose escalations for lamotrigine should not be exceeded.
Conversion from Adjunctive Therapy with Carbamazepine, Phenytoin, Phenobarbital, or Primidone to Monotherapy with Lamotrigine: After achieving a dose of 500 mg/day of lamotrigine, the concomitant enzyme-inducing antiepileptic drugs should be withdrawn by 20% decrements each week over a 4-week period. The regimen for the withdrawal of the concomitant antiepileptic drug is based on experience gained in the controlled monotherapy clinical trial.
Conversion from Adjunctive Therapy with Valproate to Monotherapy with Lamotrigine: The conversion regimen involves 4 steps outlined as follows: See Table 1.
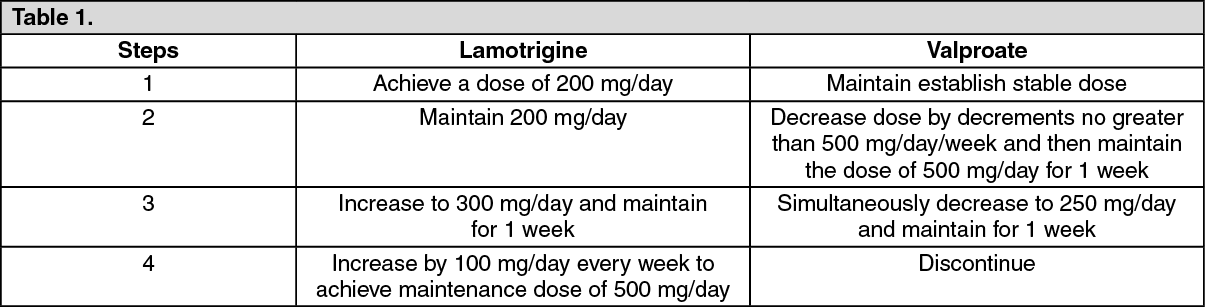 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageConversion from Adjunctive Therapy with Antiepileptic Drugs other than Carbamazepine, Phenytoin, Phenobarbital, Primidone, or Valproate to Monotherapy with Lamotrigine: No specific dosing guidelines can be provided for conversion to monotherapy with lamotrigine with antiepileptic drugs other than carbamazepine, phenytoin, phenobarbital, primidone, or valproate.
For Bipolar Disorder: As Monotherapy: The initial recommended dosage is 25 mg once daily which is gradually increased to 200 mg daily over 6 weeks. Dosages over 200 mg/day as monotherapy are not recommended.
For patients taking valproate: 25 mg every other day and the target dosage is 100 mg/day from week 6.
In recipients of carbamazepine (or other enzyme inducing drugs): The initial recommended dosage is 50 mg once daily which is gradually increased up to 400 mg I day from week 7. Dosages > 50 mg/day can be given once daily or as two divided doses. (See Table 2.)
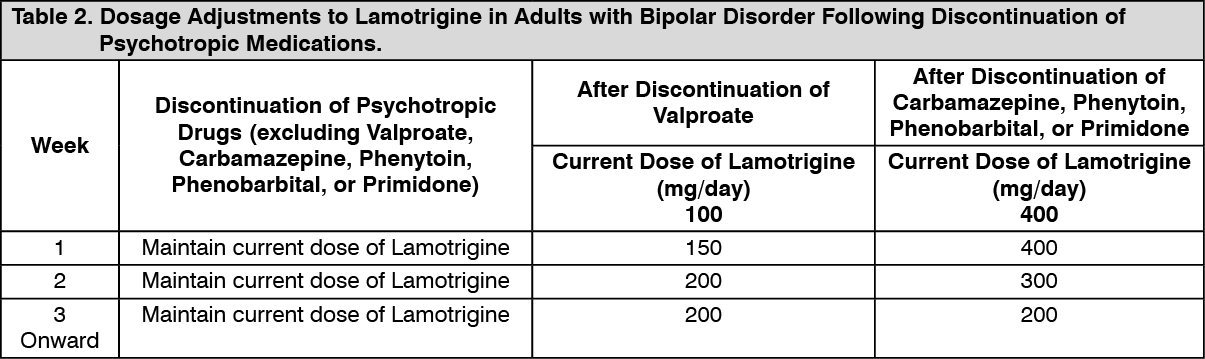 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image