Active ingredient: Granisetron HCl.
Ampoules contain 1 mg of granisetron (free-base equivalent) in 1 ml.
Therapeutic/Pharmacologic Class of Drug: Antiemetics, serotonin (5-HT3) antagonists.
Pharmacology: Pharmacodynamics: Mechanism of Action: Serotonin receptors of the 5-HT3 type are located peripherally in vagal nerve terminals and centrally in the chemoreceptor trigger zone of the area postrema. During chemotherapy-induced vomiting, mucosal enterochromaffin cells release serotonin, which stimulates 5-HT3 receptors. This invokes vagal afferent discharge, inducing vomiting.
Kytril is a potent anti-emetic and highly selective antagonist of 5-hydroxytryptamine (5-HT3) receptors. Radioligand-binding studies have demonstrated that including 5-HT3 and dopamine D2 binding sites.
Clinical/Efficacy Studies: Chemotherapy-induced nausea and vomiting (CINV): Kytril administered intravenously or orally has been shown to be effective in the prevention and treatment of nausea and vomiting associated with cancer chemotherapy in adults. Kytril administered intravenously has been shown to be effective in children aged 2 years and above for the prevention and treatment of acute CINV. There is insufficient information to recommend the oral administration of Kytril in the prevention and treatment of CINV in pediatric patients.
Radiation-induced nausea and vomiting (RINV): Kytril administered orally has been shown to be effective in the prevention and treatment of nausea and vomiting associated with total body or fractionated abdominal irradiation in adults. Efficacy in children has not been established in controlled clinical trials.
Post-operative nausea and vomiting (PONV): Kytril administered intravenously has been shown to be effective for prevention and treatment of post-operative nausea and vomiting in adults.
A prospective, multi-center, randomized, double-blind, parallel-group study evaluated a single dose of granisetron (20 or 40 μg/kg) in 157 children 2 to 16 years of age undergoing elective surgery. Total control of post-operative nausea and vomiting during the first 2 hours after surgery was observed in most patients.
Pharmacokinetics: Absorption: Absorption of Kytril is rapid and complete, though oral bioavailability is reduced to about 60% as a result of first-pass metabolism. Oral bioavailability is generally not influenced by food.
Distribution: Kytril is extensively distributed, with a mean volume of distribution of approximately 3 l/kg. Plasma protein binding is approximately 65%.
Metabolism: Biotransformation pathways involve N-demethylation and aromatic ring oxidation followed by conjugation. In vitro liver microsomal studies show that granisetron's major route of metabolism is inhibited by ketoconazole, suggestive of metabolism mediated by the cytochrome P-450 3A subfamily.
Elimination: Clearance is predominantly by hepatic metabolism. Urinary excretion of unchanged Kytril averages 12% of dose while that of metabolites amounts to about 47% of dose. The remainder is excreted in feces as metabolites. Mean plasma half-life in patients by the oral and intravenous route is approximately 9 hours, with a wide inter-subject variability.
The pharmacokinetics of oral and intravenous Kytril demonstrate no marked deviations from linear pharmacokinetics at oral doses up to 2.5-fold and intravenous doses up to 4-fold the recommended clinical dose.
The results of a study in healthy male volunteers have demonstrated that systemic delivery of 3 mg granisetron from an intramuscular injection is slower than from a 5-minute intravenous infusion (as indicated by lower Cmax and later Tmax). In other respects, the pharmacokinetics of granisetron are virtually indistinguishable when administered by these two different routes.
Pharmacokinetics in Special Populations: Renal failure: In patients with severe renal failure, data indicate that pharmacokinetic parameters after a single intravenous dose are generally similar to those in normal subjects.
Hepatic impairment: In patients with hepatic impairment due to neoplastic liver involvement, total plasma clearance of an intravenous dose was approximately halved compared to patients without hepatic involvement. Despite these changes, no dosage adjustment is necessary.
Elderly: In elderly subjects after single intravenous doses, pharmacokinetic parameters were within the range found for non-elderly subjects.
Pediatrics: In children, after single intravenous doses, pharmacokinetics are similar to those in adults when appropriate parameters (volume of distribution, total plasma clearance) are normalized for body weight.
Toxicology: Preclinical Safety: Preclinical data revealed no special hazard for humans based on conventional studies of safety pharmacology, repeated-dose toxicity, reproductive toxicity and genotoxicity. Carcinogenicity studies revealed no special hazard for humans when used in the recommended human dose. However, when administered in higher doses and over a prolonged period of time the risk of carcinogenicity cannot be ruled out.
Carcinogenicity: In carcinogenicity studies in rats and mice treated orally for their lifetime (2 years), no adverse findings were observed at dosages 25 times the clinical dose. At higher doses, Kytril induced cell proliferation in the rat liver and hepatocellular tumors in rats and mice.
Mutagenicity: Kytril was not mutagenic in mammalian or non-mammalian in vivo or in vitro test systems and there was no evidence of unscheduled DNA synthesis indicating that Kytril is not genotoxic.
Impairment of Fertility: In the rat, Kytril had no untoward effect on reproductive performance, fertility or on pre- and post-natal development.
Teratogenicity: Teratogenic effects were not observed in rats or rabbits.
Kytril is indicated for the prevention and treatment (control) of: acute and delayed nausea and vomiting associated with chemotherapy and radiotherapy; post-operative nausea and vomiting.
Standard dosage by formulation and indication for adult and pediatric patients are shown as follows.
Indication: Chemotherapy Induced Nausea and Vomiting (CINV): Adults: Prevention: A dose of 1-3 mg (10-40 mcg/kg) of Kytril should be administered either as a slow intravenous injection (over 30 seconds) or as an intravenous infusion diluted in 20 to 50 ml infusion fluid and administered over 5 minutes, prior to the start of chemotherapy.
Treatment: A dose of 1-3 mg (10-40 mcg/kg) Kytril should be administered either as a slow intravenous injection (over 30 seconds) or as an intravenous infusion diluted in 20 to 50 ml infusion fluid and administered over 5 minutes. Further treatment doses of Kytril may be administered, if required, at least 10 minutes apart. The maximum dose of Kytril to be administered over 24 hours should not exceed 9 mg.
Pediatrics: Prevention and treatment: A dose of 10-40 mcg/kg body weight (up to 3 mg) should be administered as an intravenous infusion, diluted in 10 to 30 ml over 5 minutes prior to the start of chemotherapy. One additional dose may be administered within a 24-hour period if required. This additional dose should not be administered until at least 10 minutes after the initial infusion.
Indication: Radiotherapy Induced Nausea and Vomiting (RINV): Adults: Prevention: A dose of 1-3 mg (10-40 mcg/kg) of Kytril should be administered either as a slow intravenous injection (over 30 seconds) or as an intravenous infusion diluted in 20 to 50 ml infusion fluid and administered over 5 minutes, prior to the start of radiotherapy.
Treatment: There is insufficient information to recommend the intravenous administration of Kytril in the treatment of RINV in adult patients.
Pediatrics: There is insufficient information to recommend intravenous administration of Kytril in the prevention and treatment of RINV in pediatric patients.
Indication: Post-operative Nausea and Vomiting (PONV): Adults: Prevention: A dose of 1 mg (10 mcg/kg) of Kytril should be administered as a slow intravenous injection (over 30 seconds) prior to induction of anesthesia.
Treatment: A dose of 1 mg (10 mcg/kg) of Kytril should be administered by slow intravenous injection (over 30 seconds). The maximum dose for patients undergoing anesthesia for surgery is a total dose of 3 mg of Kytril i.v. in one day.
Pediatrics: There is insufficient information to recommend the intravenous administration of Kytril in the prevention and treatment of PONV in pediatric patients.
Special Dosage Instructions: Geriatrics: No dosage adjustments required.
Renal impairment: No dosage adjustments required.
Hepatic impairment: No dosage adjustments required.
There is no specific antidote for Kytril. In the case of overdosage with Kytril, symptomatic treatment should be given. Overdosage of up to 38.5 mg of granisetron hydrochloride as a single injection has been reported without symptoms or only the occurrence of a slight headache.
Kytril is contraindicated in patients with known hypersensitivity to granisetron or to any of its excipients.
General: As Kytril may reduce lower bowel motility, patients with signs of sub-acute intestinal obstruction should be monitored closely following administration of Kytril.
As with other 5-HT3 antagonists, cases of ECG modifications including QT prolongation have been reported with Kytril. These ECG changes with Kytril were minor and generally not of clinical significance, specifically with no evidence of proarrhythmia. However, in patients with pre-existing arrhythmias or cardiac conduction disorders, this might lead to clinical consequences. Therefore, caution should be exercised in patients with cardiac comorbidities, on cardiotoxic chemotherapy and/or with concomitant electrolyte abnormalities.
Cross-sensitivity between 5-HT3 antagonists has been reported.
As with other 5-HT3 antagonists, cases of serotonin syndrome (including altered mental status, autonomic dysfunction and neuromuscular abnormalities) have been reported following the concomitant use of Kytril and other serotonergic drugs. If concomitant treatment with granisetron and other serotonergic drugs is clinically warranted, appropriate observation of this patient is advised.
Ability to Drive and Use Machines: In healthy subjects, no clinically relevant effects on resting EEG or on the performance of psychometric tests were observed after i.v. Kytril at any dose tested (up to 200 μg/kg). There are no data on the effect of Kytril on the ability to drive or use machinery.
Pregnancy: There are no studies in pregnant women and it is not known whether granisetron is excreted in human milk. Use of Kytril during pregnancy or lactation should be limited to situations where the potential benefit of the mother justifies the potential risk to the fetus or nursing infant (see Pharmacology: Toxicology: Preclinical Safety under Actions).
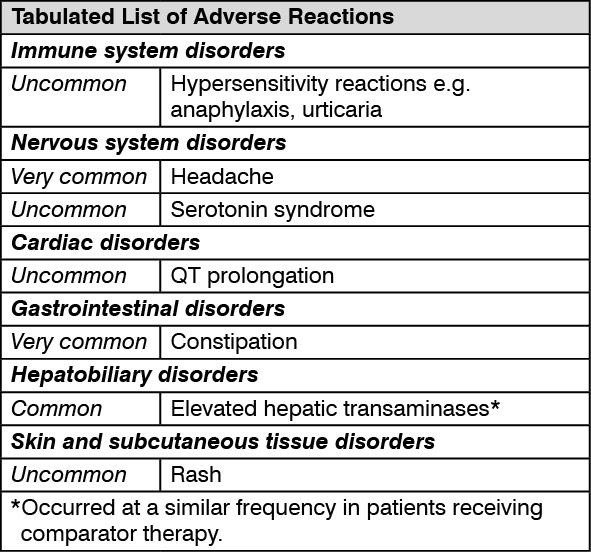
Clinical Trials: Summary of the safety profile: The most frequently reported adverse reactions for Kytril are headache and constipation which may be transient. ECG changes including QT prolongation have been reported with Kytril (see General under Precautions and Interactions).
The following table of listed adverse reactions is derived from clinical trials and post-marketing data associated with Kytril.
Frequency categories are as follows: Very common: ≥1/10; Common: ≥1/100 to <1/10; Uncommon: ≥1/1,000 to <1/100; Rare: ≥1/10,000 to <1/1,000; Very rare: <1/10,000. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Kytril has been well tolerated in human studies. In common with other drugs of this class, headache and constipation have been reported. Cases of hypersensitivity reactions, including rashes and anaphylaxis have been reported. Elevations in hepatic transaminases have been observed and at similar frequency in patients receiving comparator therapy.
As for other 5-HT
3 antagonists, cases of ECG modifications including QT prolongation have been reported with Kytril. These ECG changes with Kytril were minor and generally not of clinical significance, specifically with no evidence of proarrhythmia (see General under Precautions and Interactions).
As with other 5-HT
3 antagonists, cases of serotonin syndrome (including altered mental status, autonomic dysfunction and neuromuscular abnormalities) have been reported following the concomitant use of Kytril and other serotonergic drugs (see General under Precautions and Interactions).
Post Marketing: The post-marketing safety experience in over 4 million patients is consistent with the clinical trial safety information.
For ECG modifications, see Clinical Trials as previously mentioned.
For serotonin syndrome, see Clinical Trials as previously mentioned.
Kytril did not induce or inhibit the cytochrome P450 drug metabolizing enzyme system in rodent studies or inhibit the activity of any well-characterized P450 subfamilies studied in in vitro investigations.
In humans, hepatic enzyme induction with phenobarbital resulted in an increase in total plasma clearance of intravenous Kytril of approximately one-quarter. In in vitro human microsomal studies, ketoconazole inhibited ring oxidation of Kytril. However, given the absence of pK/pD relationship with granisetron, these changes are believed to have no clinical consequences.
Kytril has been safely administered in humans with benzodiazepines, neuroleptics and anti-ulcer medications, commonly prescribed with antiemetic treatments. Additionally, Kytril has shown no apparent drug interaction with emetogenic cancer chemotherapies.
No specific interaction studies have been conducted in anesthetized patients, but Kytril has been safely administered with commonly used anesthetic and analgesic agents. In addition, the activity of the cytochrome P450 subfamily 3A4 (involved in the metabolism of some of the main narcotic analgesic agents) is not modified by Kytril.
As for other 5-HT3 antagonists, cases of ECG modifications including QT prolongation have been reported with Kytril. These ECG changes with Kytril were minor and generally not of clinical significance, specifically with no evidence of proarrhythmia. However, in patients concurrently treated with drugs known to prolong QT interval and/or which are arrhythmogenic, this may lead to clinical consequences.
As with other 5-HT3 antagonists, cases of serotonin syndrome have been reported following the concomitant use of Kytril and other serotonergic drugs. If concomitant treatment with granisetron and other serotonergic drugs is clinically warranted, appropriate observation of this patient is advised (see General under Precautions).
Special Instructions for Use, Handling and Disposal: Preparation of Infusion: For adults: The appropriate dose is diluted with infusion fluid, to a total volume of 20 to 50 ml in any of the following solutions: 0.9% sodium chloride B.P., 0.18% sodium chloride and 4% dextrose B.P., 5% dextrose, Hartmann's solution, sodium lactate and mannitol.
For children: The appropriate dose is diluted infusion fluid (as for adults) to a total volume of 10 to 30 ml.
From a microbiological point of view the diluted product should be used immediately. If not used immediately, in-use storage times and conditions prior to use are the responsibility of the user and would normally not be longer than 24 h at 2°C - 8°C, unless dilution has taken place in controlled and validated aseptic conditions.
Protect from light.
Kytril has been shown to be stable for at least 24 hours when stored at ambient temperature in any of the following solutions: 0.9% sodium chloride B.P., 0.18% sodium chloride and 4% dextrose B.P., 5% dextrose, Hartmann's solution, sodium lactate and mannitol.
A04AA02 - granisetron ; Belongs to the class of serotonin (5HT3) antagonists. Used for the prevention of nausea and vomiting.
Kytril soln for IV infusion 1 mg/mL
1 mL x 5 × 1's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out