Each 5 mL (1 teaspoonful) of reconstituted suspension contains: Clarithromycin 125 mg or 250 mg.
Pharmacology: Pharmacodynamics: Clarithromycin is more active against susceptible streptococci and staphylococci in vitro. The minimum inhibitory concentrations of Clarithromycin are usually two- to fourfold lower than for erythromycin.
Clarithromycin is more active against some mycobacteria and have some in vitro activity against the protozoan Toxoplasma gondii, and may have some activity against cryptosporidium.
The major metabolite, 14-hydroxylclarithromycin, is also active, and may enhance the activity of Clarithromycin in vivo, notably against Haemophilus influenzae.
Clarithromycin has been shown to be active against most strains of the following microorganisms both in vitro and in clinical infections: Gram-positive Aerobes microorganisms: Staphylococcus aureus, Streptococcus pneumoniae, Streptococcus pyogenes, Listeria monocytogenes.
Gram-negative Aerobes microorganisms: Haemophilus influenzae, Haemophilus parainfluenzae, Moraxella catarrhalis, Neisseria gonorrhea, Legionella pneumophila.
Other microorganisms: Mycoplasma pneumoniae, Chlamydia pneumoniae (TWAR strain), Ureaplasma urealyticum.
Mycobacteria: Mycobacteria kansasii, Mycobacterium leprae and Mycobacterium avium complex (MAC) which includes: Mycobacterium avium, Mycobacterium intracellulare.
*Most strains of methicillin-resistant and oxacillin-resistant staphylococci are resistant to Clarithromycin.
Clarithromycin exhibits in vitro activity against most strains of the following microorganisms, but their clinical significance is unknown.
Gram-positive Aerobes microorganisms: Streptococcus agalactiae, Streptococci (Group C, F, G), Viridans group streptococci.
Gram-negative Aerobes microorganisms: Bordetella pertussis, Pasteurella multocida.
Gram-positive Anaerobes microorganisms: Bacteroides melaninogenicus.
Spirochetes: Borrelia burgdorferi, Treponema pallidum.
Campylobacter: Campylobacter jejuni.
Pharmacokinetics: Clarithromycin is rapidly absorbed from the gastrointestinal tract following oral administration, and undergoes first-pass metabolism; the bioavailability of the parent drug is about 55%. The extent of absorption is relatively unaffected by the presence of food. Peak concentrations of Clarithromycin and its principal active metabolite 14-hydroxylclarithromycin are reported to be about 0.6 and 0.7 μg per mL respectively following a single 250 mg dose by mouth; at steady-state the same dose given every 12 hours as tablets produce peak concentrations of Clarithromycin of about 1 μg per mL. The same dose given as a suspension produces a steady-state plasma concentration of about 2 μg per mL.
The pharmacokinetics of Clarithromycin are non-linear and dose dependent; high doses may produce disproportionate increases in peak concentration of the parent drug, due to saturation of the metabolic pathways.
The drug and its principal metabolite are widely distributed, and tissue concentrations exceed those in serum, in part because of intracellular uptake. Clarithromycin has been detected in breast milk. It is extensively metabolized in the liver, and excreted in feces via the bile. Substantial amounts are excreted in urine; at steady-state about 20% and 30% of a 250 mg or 500 mg dose, respectively, is excreted in this way, as unchanged drug. 14-Hydroxylclarithromycin as well as other metabolites are also excreted in the urine accounting for 10 to 15% dose. The terminal half-life of Clarithromycin is reportedly about 3 to 4 hours in patients receiving 250 mg doses twice daily, and about 5 to 7 hours in those receiving 500 mg twice daily. The half-life is prolonged in renal impairment.
Clarithromycin is a macrolide derived from erythromycin with similar actions and uses. It is given in the treatment of infections such as:
a. Respiratory tract infections (e.g. pharyngitis/tonsillitis caused by Streptococcus pyogenes, acute maxillary sinusitis, chronic bronchitis, pneumonia) including otitis media.
b. Skin and soft tissue infection caused by Staphylococcus aureus, Streptococcus pyogenes.
c. For prophylaxis and treatment of opportunistic Mycobacterial infections commonly caused by Mycobacterium kansasii, Mycobacterium avium or Mycobacterium intracellulare and for the treatment of leprosy.
d. For the prevention of disseminated infection due to Mycobacterium avium (MAC) in patients with advanced HIV infection.
e. Protozoal infection, including toxoplasmosis.
f. Clarithromycin may be given to eradicate Helicobacter pylori in the treatment regimens for peptic ulcer disease.
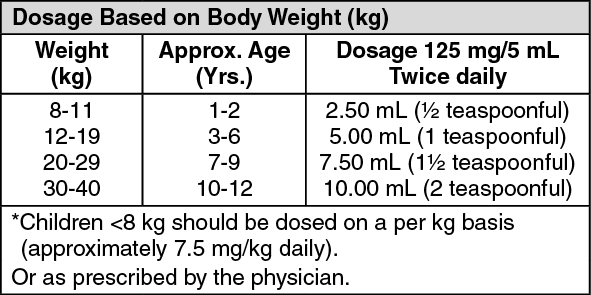
Clarithromycin Pediatric for Suspension: The usual duration of treatment is 5 to 10 days depending on the pathogen involved and the severity of the condition. The reconstituted suspension may be taken with or without meals, and may be taken with milk. (See table.)
 Click on icon to see table/diagram/image
Preparation for use: 250 mg/5 mL:
Click on icon to see table/diagram/image
Preparation for use: 250 mg/5 mL: To make a 35 mL suspension, add 25 mL of water to the granules in the bottle.
To make a 70 mL suspension, add 51 mL of water to the granules in the bottle.
Shake well until the contents are evenly suspended. The reconstituted suspension can be used up to 14 days when stored at temperatures not exceeding 30°C.
Overdosage of Clarithromycin can cause gastrointestinal symptoms such as abdominal pain, vomiting, nausea, and diarrhea.
Adverse reactions accompanying overdosage should be treated by the prompt elimination of unabsorbed drug and supportive measures. As with other macrolides, Clarithromycin serum concentrations are not expected to be appreciably affected by hemodialysis or peritoneal dialysis.
Clarithromycin is contraindicated in patients with known hypersensitivity to any macrolide antibiotics.
Astemizole, cisapride and terfenadine are contraindicated in patients on Clarithromycin.
Pseudomembranous colitis has been reported with nearly all antibacterial agents, including Clarithromycin, and may range in severity from mild to life-threatening. Therefore, it is important to consider this diagnosis in patients who represent with diarrhea subsequent to the administration of Clarithromycin and other antibacterial agents.
Clarithromycin is principally excreted via the liver and kidney. Therefore, it should be administered with caution to patients with impaired renal or hepatic function and doses should be reduced in those with severe renal impairment.
Attention should also be paid to the possibility of cross resistance between Clarithromycin and other macrolide drugs, as well as lincomycin and clindamycin.
Resistance: Prescribing Clarithromycin in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide benefit to the patient and increases the risk of the development of drug-resistance.
Erythromycin-resistant isolates of Streptococcus pneumoniae are commonly cross-resistant to Clarithromycin. The incidence of resistance to Clarithromycin and other macrolides is higher among penicillin-resistant strains than among penicillin-sensitive strains.
Clarithromycin should not be used in pregnant women except in clinical circumstances where no alternative therapy is appropriate. If pregnancy occurs while taking this drug, the patient should be apprised of the potential hazard to the fetus.
It should not be used during pregnancy if possible: high doses have been associated with embryotoxicity in animal studies.
It is not known whether Clarithromycin is excreted in breast milk. Exercise caution when administering to a nursing woman.
Gastrointestinal disturbances, e.g. nausea, dyspepsia, abdominal pain, vomiting, and diarrhea are the most frequent adverse effects of Clarithromycin but are usually mild and less frequent than with erythromycin. Other adverse effects are taste disturbances, stomatitis, glossitis, and tooth decoloration. Transient elevations of liver enzyme values, cholestatic jaundice, and hepatitis have been reported. Headache and rashes from mild skin eruptions to, rarely, Stevens-Johnson syndrome have occurred. There also have been reports of transient CNS effects such as anxiety, dizziness, insomnia, hallucinations, and confusion. Hearing loss has been reported occasionally and is usually reversible. Other effects include hypoglycemia and thrombocytopenia. Interstitial nephritis and renal failure have been reported rarely.
Thrombocytopenic purpura, corneal opacities which is usually reversible upon discontinuation of the treatment, pseudomembranous colitis associated with
Clostridium difficile developed in a child receiving Clarithromycin, acute psychoses, pancreatitis, QT prolongation and Torsade de Pointes, fever associated with Clarithromycin and leukocytoclastic vasculitis have also been reported.
Increased rifabutin toxicity has been reported in patients receiving Clarithromycin and rifabutin. There has been also a report of delirium following concurrent use with fluoxetine.
Antiretroviral drugs: Concomitant administration of the HIV - protease inhibitor ritonavir inhibit the metabolism of Clarithromycin producing elevated plasma concentrations and a prolonged half-life. It has been suggested that other HIV - protease inhibitors and non-nucleoside reverse transcriptase inhibitors may also affect the metabolism of Clarithromycin. Concurrent use of efavirenz with Clarithromycin has resulted in decrease in the plasma concentration of Clarithromycin and increases in its hydroxyl metabolite. This combination has been associated with a high incidence of skin rashes. Decreased concentrations of zidovudine have been reported in patients also taking Clarithromycin. It is recommended that the doses of these two drugs should be separated by 1 to 2 hours.
Administration of cimetidine with Clarithromycin may alter some of the pharmacokinetic parameters of Clarithromycin. The clinical significance of such changes is unknown.
Concomitant administration of omeprazole with Clarithromycin resulted in increased concentrations of Clarithromycin and its active metabolite. There is also an increased and prolonged plasma concentrations of omeprazole. This interaction could account for the synergistic action with the combination when used for eradication of Helicobacter pylori.
Activity with other antimycobacterials: Clarithromycin has been reported to enhance the activity of a number of antimycobacterials including ethambutol, isoniazid, pyrazinamide, and rifampicin against Mycobacterium tuberculosis.
The use of Clarithromycin in patients receiving theophylline may be associated with an increase of serum theophylline concentrations. Monitoring of serum theophylline concentrations should be considered for patients receiving high doses of theophylline or with base line concentrations in the upper therapeutic range.
Concurrent use of single doses of Clarithromycin and carbamazepine has been shown to result in increased plasma concentrations of carbamazepine. Blood level monitoring of carbamazepine may be considered.
When Clarithromycin and terfenadine were co-administered, plasma concentrations of the active acid metabolite of terfenadine were threefold higher, an average, than the values observed when terfenadine was administered alone. The pharmacokinetics of Clarithromycin and the 14-hydroxylclarithromycin were not significantly affected by co-administration of terfenadine once Clarithromycin reached steady-state conditions.
Co-administration of fluconazole and Clarithromycin increased the mean steady-state Clarithromycin Cmin of 33% and AUC of 18%. Steady-state concentrations of 14-hydroxylclarithromycin were not significantly affected by the concomitant administration of fluconazole.
Concurrent use of Clarithromycin and oral anticoagulants may potentiate the effects of the oral anticoagulants. Prothrombin time should be carefully monitored.
There have been reports on increased digoxin serum concentrations when Clarithromycin is co-administered with digoxin. Monitoring of serum digoxin concentrations should be considered.
Colchicine toxicity have been reported with concomitant use of Clarithromycin and colchicine, especially in the elderly, some of which occurred in patients with renal insufficiency.
Clarithromycin is a substrate and inhibitor of the 3A isoform subfamily of the cytochrome P450 enzyme system (CYP3A). Co-administration of Clarithromycin and a drug primarily metabolized by CYP3A may be associated with elevations in drug concentrations that could increase or prolong both the therapeutic and adverse effects of the concomitant drug. The following are examples of clinically significant CYP3A based drug interactions observed with Clarithromycin: Antiarrhythmics: There have been post marketing reports of Torsades de Pointes occurring with concurrent use of Clarithromycin and quinidine or disopyramide. Electrocardiograms should be monitored for QTc prolongation during co-administration of Clarithromycin with these drugs. Serum concentrations of these medications should also be monitored.
Post-marketing reports indicate that co-administration of Clarithromycin with ergotamine or dihydroergotamine has been associated with acute toxicity characterized by vasospasm and ischemia of the extremities and other tissues including the central nervous system. Concomitant administration of Clarithromycin with ergotamine or dihydroergotamine is contraindicated.
Drug interactions and CNS effects (e.g. somnolence and confusion) have been reported with the concomitant use of Clarithromycin and triazolobenzodiazepines (such as triazolam and alprazolam) and other related benzodiazepines (such as midazolam).
Clarithromycin has been reported to increase concentrations of HMG-CoA reductase inhibitors (e.g. lovastatin and simvastatin). There have been rare reports of rhabdomyolysis in patients taking these drugs concomitantly.
Clarithromycin has been reported to increase the systematic exposure (AUC) of sildenafil. Reduction of sildenafil dosage should be considered.
There have been published reports of CYP3A based interactions of Clarithromycin with cyclosporine, carbamazepine, tacrolimus, alfentanil, disopyramide, rifabutin, quinidine, methylprednisolone, cilostazol, and bromocriptine. In addition, there also have been reports of interactions of Clarithromycin with drugs not thought to be metabolized by CYP3A, including hexobarbital, phenytoin and valproate.
Store at temperatures not exceeding 30°C.
For Reconstituted Suspension: After mixing, store at temperatures not exceeding 30°C.
Shake well before each use.
Keep tightly closed. Do not refrigerate.
J01FA09 - clarithromycin ; Belongs to the class of macrolides. Used in the systemic treatment of infections.
Klaryth granules for oral susp 250 mg/5 mL
35 mL x 1's;70 mL x 1's



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out