Pharmacology: Pharmacodynamics: Patients with chronic kidney disease retain phosphorus and can develop hyperphosphataemia. High serum phosphorus can precipitate serum calcium resulting in ectopic calcifications. When the product of serum calcium and phosphorus concentrations (Ca x P) exceeds 55 mg/dL there is an increased risk that ectopic calcification will occur. Hyperphosphatemia plays a role in the development of secondary hyperparathyroidism in renal insufficiency. An increase in parathyroid hormone (PTH) level is characteristic of patients with chronic kidney disease. Increased levels of PTH can lead to osteitis fibrosa. A decrease in serum phosphorus may decrease serum PTH levels.
Treatment of hyperphosphatemia includes reduction of dietary intake of phosphate, inhibition of intestinal phosphate absorption with phosphate binders and removal of phosphate with dialysis. Sevelamer Carbonate taken with meals has been shown to decrease serum phosphorus concentrations in patients with chronic kidney disease who are on hemodialysis. In vitro studies have shown that the capsule and tablet formulations bind phosphate to a similar extent. Sevelamer Carbonate (Khrizvela) treatment also results in a lowering of low-density lipoprotein (LDL) and total serum cholesterol levels.
Mechanism of action: Sevelamer Carbonate (Khrizvela) contains Sevelamer hydrochloride, a non-absorbed phosphate binding poly (allylamine hydrochloride) polymer, free of metal and calcium. It contains multiple amines separated by one carbon from the polymer backbone. These amines exist in a partially protonated form in the intestine and interact with phosphate molecules through ionic and hydrogen bonding. By binding phosphate in the dietary tract, Sevelamer hydrochloride lowers the phosphate concentration in the serum. In clinical trials, Sevelamer hydrochloride has been shown to be effective in reducing serum phosphorus in patients receiving hemodialysis or peritoneal dialysis.
Sevelamer hydrochloride decreases the incidence of hypercalcemic episodes as compared to patients using calcium based phosphate binders alone. The effects on phosphate and calcium were proven to be maintained throughout a study with one year follow-up. Sevelamer hydrochloride has been shown to bind bile acids in vitro and in vivo in animal models. Bile acid binding by ion exchange resins is a well-established method of lowering blood cholesterol. In clinical trials both the mean total and LDL cholesterol declined by 15-31%. This effect is observed after 2 weeks and is maintained with long-term treatment. Triglycerides, HDL cholesterol and albumin did not change. In the clinical studies in hemodialysis patients, Sevelamer hydrochloride alone did not have a consistent and clinically significant effect on serum intact parathyroid hormone (iPTH). In patients with secondary hyperparathyroidism Sevelamer Carbonate (Khrizvela) should be used within the context of a multiple therapeutic approach, which could include calcium supplements, and 1,25-dihydroxy vitamin D3 or one of its analogues to lower the intact parathyroid hormone (iPTH) levels.
Clinical efficacy/Clinical: The ability of Sevelamer Carbonate (Khrizvela) to lower serum phosphorus in CKD patients on hemodialysis was demonstrated in six clinical trials, one double-blind placebo controlled 2-week study (Sevelamer Carbonate (Khrizvela) N=24); two open-label uncontrolled 8-week studies (Sevelamer Carbonate (Khrizvela) N=220) and three active control open-label studies with treatment durations of 8 to 52 weeks (Sevelamer Carbonate (Khrizvela) N=256). Three of the active-controlled studies are described here. One trial was a crossover trial with two 8-week periods comparing Sevelamer Carbonate (Khrizvela) to calcium acetate. The second trial was a 52-week parallel design trial comparing Sevelamer Carbonate (Khrizvela) with calcium acetate or calcium carbonate. The third was a 12-week parallel design study was conducted comparing Sevelamer Carbonate (Khrizvela) and calcium acetate in peritoneal dialysis patients.
Crossover Study of Sevelamer Carbonate (Khrizvela) and calcium acetate: Eighty-four CKD patients on hemodialysis who were hyperphosphatemic (serum phosphorus > 6 mg/dL) following a 2-week phosphate binder washout period were randomized to receive either Sevelamer Carbonate (Khrizvela) for 8 weeks followed by calcium acetate for 8 weeks or calcium acetate for 8 weeks followed by Sevelamer Carbonate (Khrizvela) for 8 weeks. 4 Treatment periods were separated by a 2-week phosphate binder washout period. Patients started on Sevelamer Carbonate (Khrizvela) capsules or calcium acetate tablets 3 times per day with meals. Over each 8-week treatment period, at three separate time points the dose of either agent could be titrated up one capsule or tablet per meal (3 per day) to control serum phosphorus. Sevelamer Carbonate (Khrizvela) and calcium acetate both significantly decreased mean serum phosphorus by approximately 2 mg/dL.
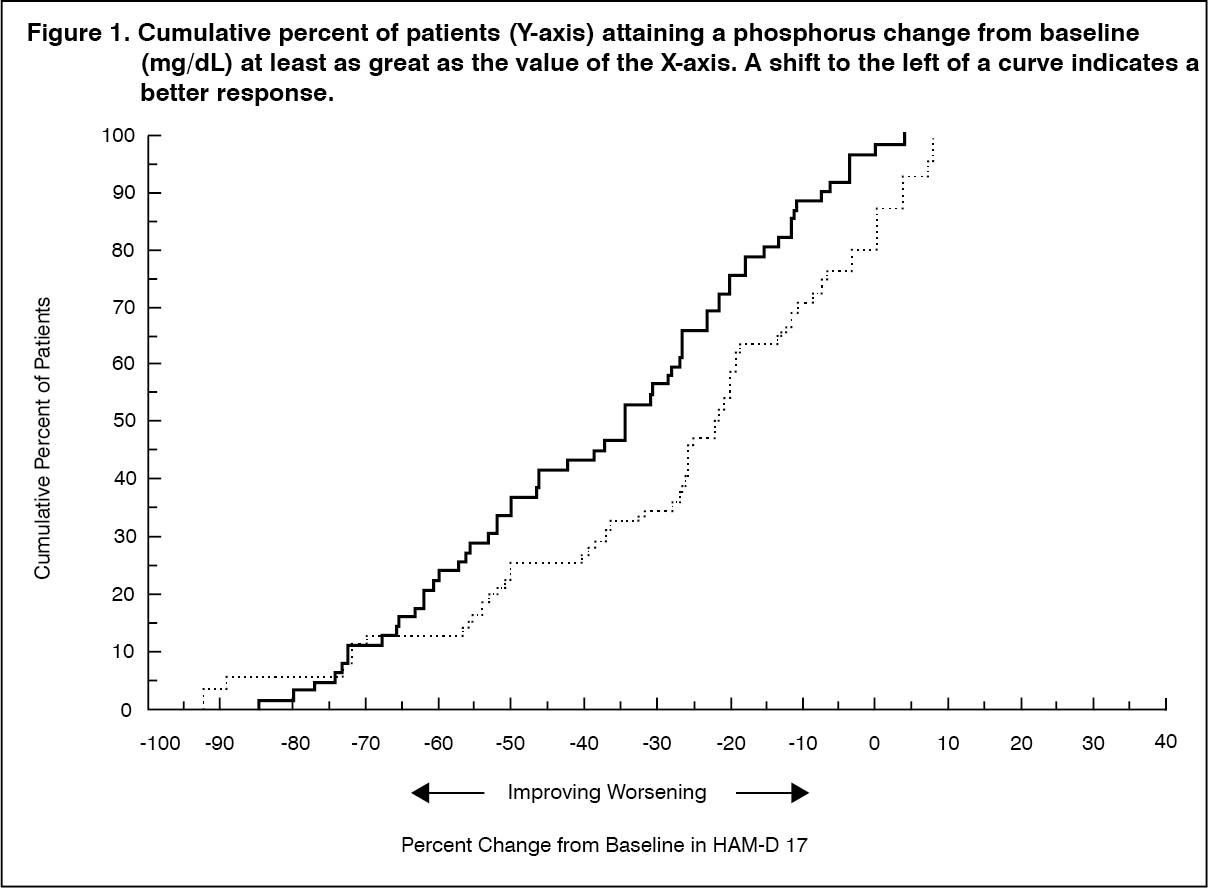
Sixty one percent of Sevelamer Carbonate (Khrizvela) patients and 73% of the calcium patients completed the full 52 weeks of treatment. The major reason for dropout in the Sevelamer Carbonate (Khrizvela) group was gastrointestinal adverse events.
Figure 1, a plot of the phosphorus change from baseline for the completers, illustrates the durability of response for patients who are able to remain on treatment. (See Figure 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Average daily consumption at the end of the treatment was 6.5 g of Sevelamer hydrochloride (range of 0.8 to 13 g) or approximately eight 800 mg (range of 1 to 16 tablets), 4.6 g of calcium acetate (range of 0.7 to 9.5 g) and 3.9 g of calcium carbonate (range of 1.3 to 9.1 g). During calcium treatment 34% of patients developed serum calcium corrected for albumin ≥ 11.0 mg/dL on at least one occasion versus 7% for Sevelamer Carbonate (Khrizvela) (p<0.05). Thus the risk of developing hypercalcemia is less with Sevelamer Carbonate (Khrizvela) compared to calcium based binders.
Mean LDL cholesterol and mean total cholesterol declined significantly (p<0.05) on Sevelamer Carbonate (Khrizvela) treatment (-32% and -20%, respectively) compared to calcium (+0.2% and -2%, respectively). Triglycerides, HDL cholesterol, and albumin did not change.
Parallel Study of Sevelamer Hydrochloride or Calcium Acetate in Peritoneal Dialysis Patients: One hundred and forty three patients on peritoneal dialysis who were hyperphosphatemic (serum phosphorus > 5.5 mg/dL) following a two-week phosphate binder washout period were randomized to receive Sevelamer Carbonate (Khrizvela) 800 mg tablets (N=97) or calcium acetate (N=46). Treatment for 12 weeks with Sevelamer Carbonate (Khrizvela) was non-inferior to calcium acetate in reducing serum phosphorus. There were statistically significant changes in serum phosphorus (p< 0.001) from baseline for both the Sevelamer Carbonate (Khrizvela) (-1.61 mg/dl from 7.48 mg/dL) and calcium acetate (-1.81 mg/dL from 7.29 mg/dL) groups.
Average daily consumption at the end of treatment was 5.9 g for Sevelamer Carbonate (Khrizvela) (range of 0.8 to 14.3 g) and 4.3 g for calcium acetate (range of 1.7 to 9.0 g). During calcium acetate treatment, 18% of patients had a serum calcium corrected for albumin > 11.0 mg/dL at the end of the study versus 2% for Sevelamer Carbonate (Khrizvela) (p=0.001).
A statistically significant decrease from baseline for total-, LDL-, and non-HDL cholesterol was observed in the Sevelamer Carbonate (Khrizvela) group, but not the calcium group.
Pharmacokinetics: Absorption: A mass balance study using
14C-Sevelamer hydrochloride, in 16 healthy male and female volunteers showed that Sevelamer hydrochloride is not systematically absorbed. No absorption studies have been performed in patients with renal disease.
Toxicology: Non-Clinical Safety Data: Non-clinical safety studies were conducted for Sevelamer Carbonate and Sevelamer hydrochloride which contains the same active moiety, Sevelamer.
Acute toxicity: In preclinical studies in rats and dogs, Sevelamer hydrochloride at a human equivalent dose of 10 times the maximum clinical trial dose of 14.4 g/day, reduced absorption of fat soluble vitamins D, E and K, and folic acid.
A single dose study with Sevelamer Carbonate at doses of 10,000, 15,000 and 20,000 mg/kg by oral route (dietary admixture) was conducted in rats. At 20,000 mg/kg/day, there were no unscheduled deaths or any clinical signs observed during the treatment or observation periods. Slightly lower food consumption was recorded for both sexes during the 24-hour treatment period, probably due to minor unpalatability of the dietary admixture at this concentration, but no evidence of a persistent effect was noted during the observation period. Both sexes also had a slightly lower mean body weight gain over the treatment period compared to controls; however, this was not evident during the observation period. Hematology, blood biochemistry and organ weights were unremarkable, and no treatment-related macroscopic findings were observed. Therefore it was considered that the No Observed Adverse Effect Level (NOAEL) for Sevelamer Carbonate administered over a 24-hour period was 20,000 mg/kg/day.
Carcinogenicity: Standard lifetime carcinogenicity bioassays were conducted in mice and rats. Rats were given Sevelamer hydrochloride by diet at 0.3, 1, or 3 g/kg/day. There was an increased incidence of urinary bladder transitional cell papilloma in male rats (3 g/kg/day) at a human equivalent dose 2 times the maximum clinical trial dose of 12 g/day. Mice received mean dietary doses of 0.8, 3, or 9 g/kg/day. No increased incidence of tumors was observed in mice at a human equivalent dose 3 times the maximum clinical trial dose of 13 g/day, based on a comparison of relative body surface area. (See Table 1.)
Click on icon to see table/diagram/image
Figure 2 illustrates that the proportion of patients achieving a given level of serum phosphorus lowering is comparable between the two treatment groups. For example, about half the patients in each group had a decrease of at least 2 mg/dL at endpoint. (See Figure 2.)
Click on icon to see table/diagram/image
Average daily consumption at the end of treatment was 4.9 g Sevelamer hydrochloride (range of 0 to 12.6 g) and 5.0 g of calcium acetate (range of 0 to 17.8 g). During calcium acetate treatment, 22% of patients developed serum calcium ≥ 11 mg/dL on at least one occasion versus 5% for Sevelamer hydrochloride (p<0.05). Thus the risk of developing hypercalcemia is less with Sevelamer Carbonate (Khrizvela) compared to calcium acetate.
Mean LDL cholesterol and mean total cholesterol declined significantly on Sevelamer Carbonate (Khrizvela) treatment (-24% and -15%, respectively). Neither LDL nor total cholesterol changed on calcium acetate treatment. Triglycerides, high-density lipoprotein (HDL) cholesterol, and albumin did not change on either treatment. Similar reductions in serum phosphorus and LDL cholesterol were observed in an 8-week open-label, uncontrolled study of 172 end-stage renal disease patients on hemodialysis.
Parallel study of Sevelamer Carbonate (Khrizvela) and calcium acetate or calcium carbonate: Two hundred CKD patients on hemodialysis who were hyperphosphatemic (serum phosphorus > 5.5 mg/dL) following a two-week phosphate binder washout period were randomized to receive Sevelamer Carbonate (Khrizvela) 800 mg tablets (N=99) or calcium, either calcium acetate (N=54) or calcium carbonate (N=47). Calcium acetate and calcium carbonate produced comparable decreases in serum phosphorus. At week 52, using last-observation-carried-forward, Sevelamer Carbonate (Khrizvela) and calcium both significantly decreased mean serum phosphorus. (See Table 2.)
Click on icon to see table/diagram/image
To investigate the mechanism of action of proliferative effects (development of urinary bladder transitional cell papilloma) noted previously in the rat study, Sevelamer Carbonate was administered to male rats by dietary admixture for a period of 13 weeks at nominal dose-levels of 250, 1000 or 4500 mg/kg/day followed by 6 week treatment free period. Sevelamer Carbonate was well tolerated at all dose-levels. Only slightly lower body weight gain was observed in rats treated with 4500 mg/kg/day over the study period. No treatment-related changes were seen in the macroscopic or microscopic examinations. The urine of the mid and high dose Sevelamer Carbonate groups contained significant levels of calcium oxalate crystals, and plasma vitamin E levels were significantly decreased in the high dose group. Known effects of the pharmacological action of Sevelamer Carbonate include decreased vitamin E uptake and modification of other electrolytes in the blood and urine due to altered calcium metabolism. This study confirmed these effects but did not reproduce the proliferative effects observed in the urinary tract in a previous study.
Mutagenicity: In an in vitro mammalian cytogenetic test with metabolic activation, Sevelamer hydrochloride caused a statistically significant increase in the number of structural chromosome aberrations. Sevelamer hydrochloride was not mutagenic in the Ames bacterial mutation assay.
Impairment of fertility: In a study designed to assess potential impairment of fertility, female rats were given dietary doses of 0.5, 1.5, or 4.5 g/kg/day beginning 14 days prior to mating and continuing through gestation. Male rats were given the same doses and treated for 28 days before mating. Sevelamer hydrochloride did not impair fertility in male or female rats at exposures at a human equivalent dose 2 times the maximum clinical trial dose of 13 g/day, based on a comparison of relative body surface area.
Reproduction toxicity: In pregnant rats given dietary doses of 0.5, 1.5 or 4.5 g/kg/day of Sevelamer hydrochloride during organogenesis, reduced or irregular ossification of fetal bones, probably due to a reduced absorption of fat-soluble vitamin D, occurred in mid- and high-dose groups (human equivalent doses less than the maximum clinical trial dose of 13 g). In pregnant rabbits given oral doses of 100, 500 or 1000 mg/kg/day of Sevelamer hydrochloride by gavage during organogenesis, an increase or early resorptions occurred in the high-dose group (human equivalent dose twice the maximum clinical trial dose).



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image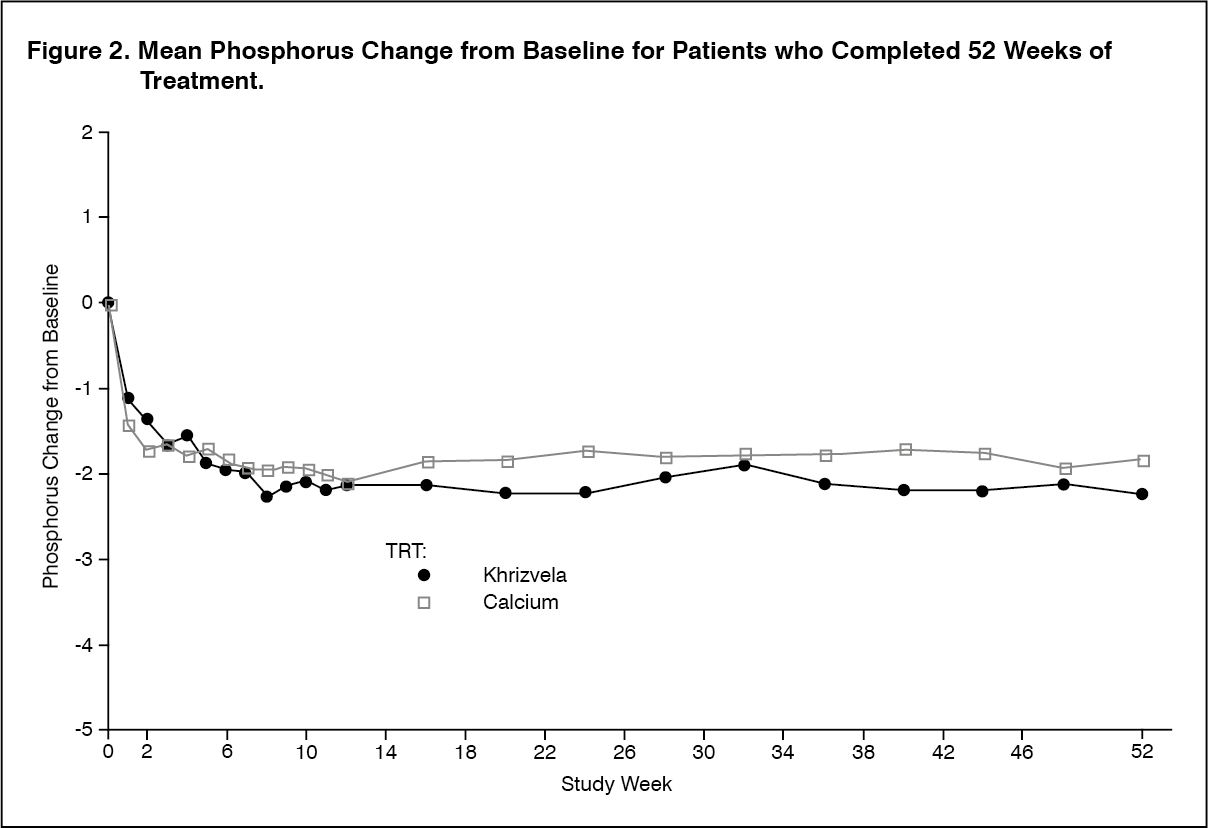 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image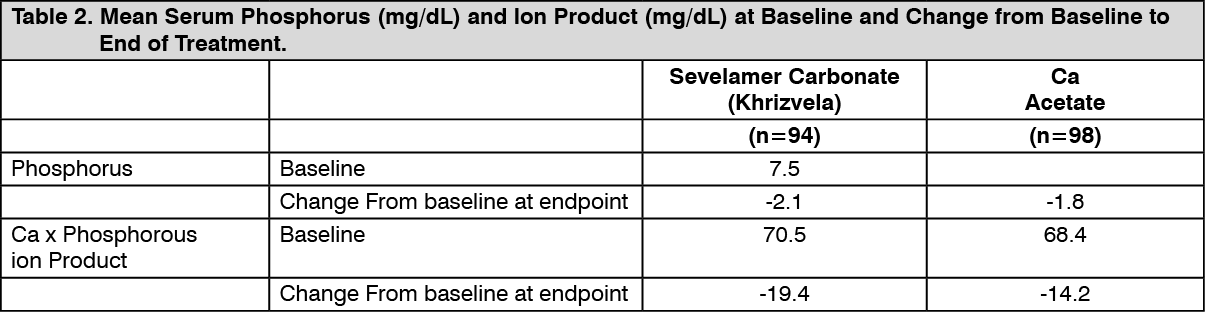 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out