Itraconazole is mainly metabolized through CYP3A4. Other substances that either share this metabolic pathway or modify CYP3A4 activity may influence the pharmacokinetics of Itraconazole. Similarly, Itraconazole may modify the pharmacokinetics of other substances that share this metabolic pathway. Itraconazole is a potent CYP3A4 inhibitor and a P-glycoprotein inhibitor. When using concomitant medication, it is recommended that the corresponding label be consulted for information on the route of metabolism and the possible need to adjust dosages.
Drugs that may decrease Itraconazole plasma concentrations: Drugs that reduce the gastric acidity (e.g. acid neutralizing medicines such as aluminum hydroxide, or acid secretion suppressors such as H2-receptor antagonists and proton pump inhibitors) impair the absorption of Itraconazole from Itraconazole capsules. It is recommended that these drugs be used with caution when co-administered with Itraconazole capsules: It is recommended that Itraconazole be administered with an acidic beverage (such as non-diet cola) upon co-treatment with drugs reducing gastric acidity.
It is recommended that acid neutralizing medicines (e.g. aluminum hydroxide) be administered at least 1 hour before or 2 hours after the intake of Itraconazole Capsules.
Upon co-administration, it is recommended that the antifungal activity be monitored and the Itraconazole dose increased as deemed necessary.
Co-administration of Itraconazole with potent enzyme inducers of CYP3A4 may decrease the bioavailability of Itraconazole and hydroxy-Itraconazole to such an extent that efficacy may be largely reduced.
Examples include:
Antibacterials: isoniazid, rifabutin (see also under Drugs that may have their plasma concentrations increased by Itraconazole), rifampicin.
Anticonvulsants: carbamazepine, (see also under Drugs that may have their plasma concentrations increased by Itraconazole), phenobarbital, phenytoin.
Antivirals: efavirenz, nevirapine.
Therefore, administration of potent enzyme inducers of CYP3A4 with Itraconazole is not recommended. It is recommended that the use of these drugs be avoided from 2 weeks before and during treatment with Itraconazole, unless the benefits outweigh the risk of potentially reduced Itraconazole efficacy. Upon co-administration, it is recommended that the antifungal activity be monitored and the Itraconazole dose increased as deemed necessary.
Drugs that may increase Itraconazole plasma concentrations: Potent inhibitors of CYP3A4 may increase the bioavailability of Itraconazole.
Examples include:
Antibacterials: ciprofloxacin, clarithromycin, erythromycin.
Antivirals: ritonavir-boosted darunavir, ritonavir-boosted fosamprenavir, indinavir (see also under Drugs that may have their plasma concentrations increased by Itraconazole), ritonavir (see also under Drugs that may have their plasma concentrations increased by Itraconazole).
It is recommended that these drugs be used with caution when co-administered with Itraconazole capsules. It is recommended that patients who must take Itraconazole concomitantly with potent inhibitors of CYP3A4 be monitored closely for signs or symptoms of increased or prolonged pharmacologic effects of Itraconazole, and the Itraconazole dose be decreased as deemed necessary. When appropriate, it is recommended that Itraconazole plasma concentrations be measured.
Drugs that may have their plasma concentrations increased by Itraconazole: Itraconazole and its major metabolite, hydroxy-Itraconazole, can inhibit the metabolism of drugs metabolized by CYP3A4 and can inhibit the drug transport by P-glycoprotein, which may result in increased plasma concentrations of these drugs and/or their active metabolite(s) when they are administered with Itraconazole. These elevated plasma concentrations may increase or prolong both therapeutic and adverse effects of these drugs. CYP3A4-metabolised drugs known to prolong the QT interval may be contraindicated with Itraconazole, since the combination may lead to ventricular tachyarrhythmias including occurrences of torsade de pointes, a potentially fatal arrhythmia. Once treatment is stopped, Itraconazole plasma concentrations decrease to an almost undetectable concentration within 7 to 14 days, depending on the dose and duration of treatment. In patients with hepatic cirrhosis or in subjects receiving CYP3A4 inhibitors, the decline in plasma concentrations may be even more gradual. This is particularly important when initiating therapy with drugs whose metabolism is affected by Itraconazole.
The interacting drugs are categorized as follows: 'Contraindicated': Under no circumstances is the drug to be co-administered with Itraconazole, and up to two weeks after discontinuation of treatment with Itraconazole.
'Not recommended': It is recommended that the use of the drug be avoided during and up to two weeks after discontinuation of treatment with Itraconazole, unless the benefits outweigh the potentially increased risks of side effects. If co-administration cannot be avoided, clinical monitoring for signs or symptoms of increased or prolonged effects or side effects of the interacting drug is recommended, and its dosage be reduced or interrupted as deemed necessary. When appropriate, it is recommended that plasma concentrations be measured.
'Use with caution': Careful monitoring is recommended when the drug is co-administered with Itraconazole. Upon co-administration, it is recommended that patients be monitored closely for signs or symptoms of increased or prolonged effects or side effects of the interacting drug, and its dosage be reduced as deemed necessary. When appropriate, it is recommended that plasma concentrations be measured.
Examples of drugs that may have their plasma concentrations increased by Itraconazole presented by drug class with advice regarding co-administration with Itraconazole: See Table 4.
 Click on icon to see table/diagram/image
Drugs that may have their plasma concentrations decreased by Itraconazole:
Click on icon to see table/diagram/image
Drugs that may have their plasma concentrations decreased by Itraconazole: Co-administration of Itraconazole with the NSAID meloxicam may decrease the plasma concentrations of meloxicam. It is recommended that meloxicam be used with caution when co-administered with Itraconazole, and its effects or side effects be monitored. It is recommended that the dosage of meloxicam, if co-administered with Itraconazole, be adapted if necessary.
Pediatric Population: Interaction studies have only been performed in adults.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image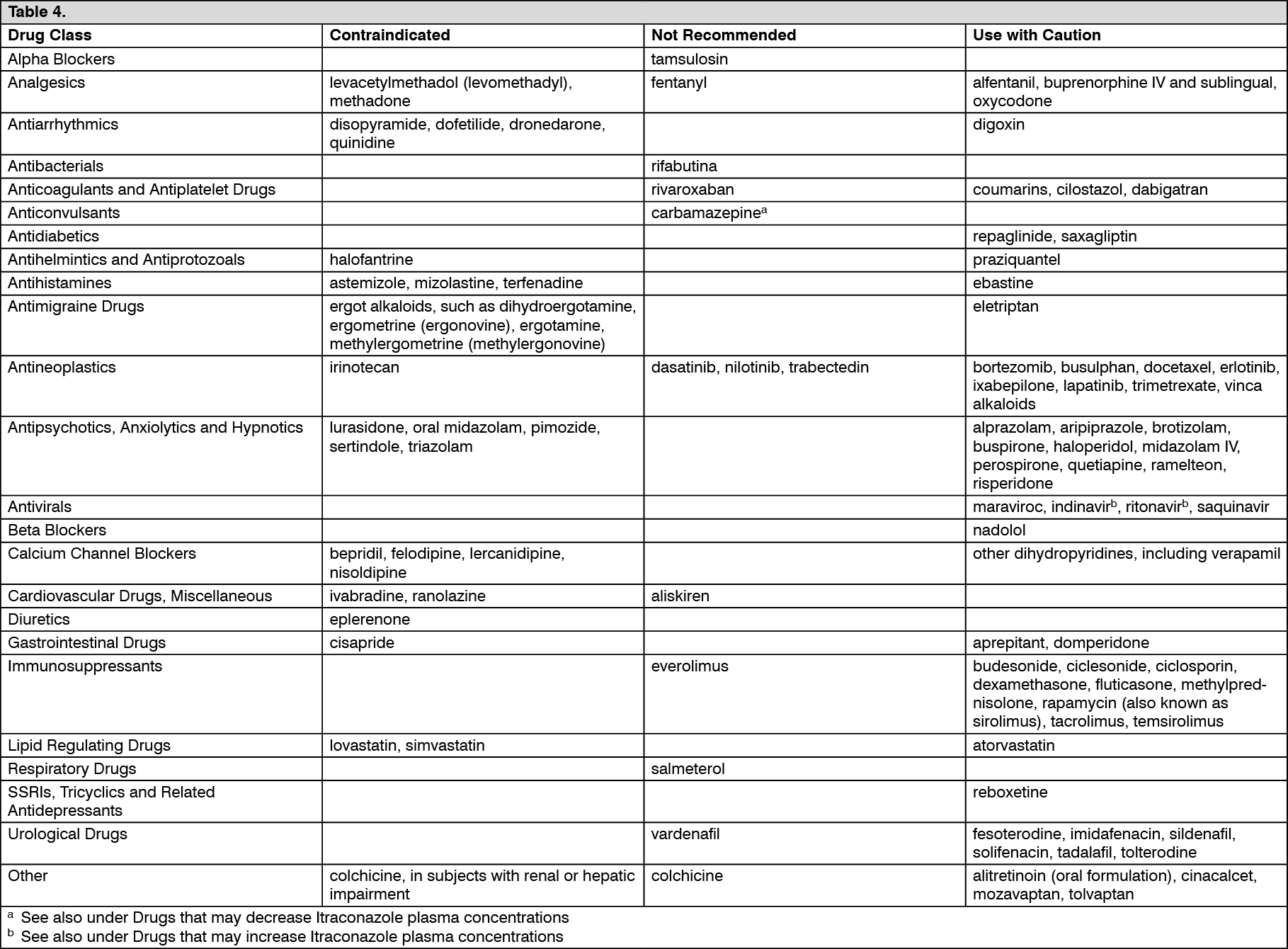 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out