Summary of the safety profile: Tremelimumab (IMJUDO) in combination with durvalumab: The safety of tremelimumab 300 mg as a single dose in combination with durvalumab, is based on pooled data in 462 HCC patients (HCC pool) from the HIMALAYA Study and another study in HCC patients, Study 22. The most common (>10%) adverse reactions were rash (32.5%), pruritus (25.5%), diarrhoea (25.3%), abdominal pain (19.7%), aspartate aminotransferase increased/alanine aminotransferase increased (18.0%), pyrexia (13.9%), hypothyroidism (13.0%), cough/productive cough (10.8%) and oedema peripheral (10.4%). (See Tables 5a and 5b.)
The most common (>3%) severe adverse reactions (NCI CTCAE Grade ≥3) were aspartate aminotransferase increased/alanine aminotransferase increased (8.9%), lipase increased (7.1%), amylase increased (4.3%) and diarrhoea (3.9%).
The most common (>2%) serious adverse reactions were colitis (2.6%), diarrhoea (2.4%) and pneumonia (2.2%).
The frequency of treatment discontinuation due to adverse reactions is 6.5%. The most common adverse reactions leading to treatment discontinuation were hepatitis (1.5%) and aspartate aminotransferase increased/alanine aminotransferase increased (1.3%).
Tremelimumab (IMJUDO) in combination with durvalumab and chemotherapy: The safety of tremelimumab given in combination with durvalumab and chemotherapy is based on data in 330 patients with metastatic NSCLC. The most common (>10%) adverse reactions were anaemia (49.7%), nausea (41.5%), neutropenia (41.2%), fatigue (36.1%), decreased appetite (28.2%), rash (25.8%), thrombocytopenia (24.5%), diarrhoea (21.5%), leukopenia (19.4%), constipation (19.1%), vomiting (18.2%), aspartate aminotransferase increased/alanine aminotransferase increased (17.6%), pyrexia (16.1%), upper respiratory tract infections (15.5%), pneumonia (14.8%), hypothyroidism (13.3%), arthralgia (12.4%), cough/productive cough (12.1%) and pruritus (10.9%).
The most common (>3%) severe adverse reactions (NCI CTCAE Grade ≥3) were neutropenia (23.9%), anaemia (20.6%), pneumonia (9.4%), thrombocytopenia (8.2%), leukopenia (5.5%), fatigue (5.2%), lipase increased (3.9%) and amylase increased (3.6%).
The most common (>2%) serious adverse reactions were pneumonia (11.5%), anaemia (5.5%), thrombocytopenia (3%), colitis (2.4%), diarrhoea (2.4%), pyrexia (2.4%) and febrile neutropenia (2.1%).
Tremelimumab was discontinued due to adverse reactions in 4.5% of patients. The most common adverse reactions leading to treatment discontinuation were pneumonia (1.2%) and colitis (0.9%).
Tremelimumab was interrupted due to adverse reactions in 40.6% of patients. The most common adverse reactions leading to dose interruption were neutropenia (13.6%), thrombocytopenia (5.8%), leukopenia (4.5%), diarrhoea (3.0%), pneumonia (2.7%), aspartate aminotransferase increased/alanine aminotransferase increased (2.4%), fatigue (2.4%), lipase increased (2.4%), colitis (2.1%), hepatitis (2.1%) and rash (2.1%).
Tabulated list of adverse reactions: Tables 5a and 5b, unless otherwise stated, lists the incidence of adverse reactions (ADRs) in patients treated with tremelimumab 300 mg in combination with durvalumab in the HCC pool of 462 patients, and Tremelimumab (IMJUDO) in combination with durvalumab and platinum-based chemotherapy in the POSEIDON Study, in which 330 patients received tremelimumab. In the POSEIDON study, patients were exposed to tremelimumab during a median of 20 weeks.
Adverse reactions are listed according to system organ class in MedDRA. Within each system organ class, the ADRs are presented in decreasing frequency. The corresponding frequency category for each ADR is defined as: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1000); very rare (<1/10,000); not known (cannot be estimated from available data). Within each frequency grouping, ADRs are presented in order of decreasing seriousness. (See Tables 5a and 5b.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Description of selected adverse reactions:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Description of selected adverse reactions: Tremelimumab is associated with immune-mediated adverse reactions. Most of these, including severe reactions, resolved following initiation of appropriate medical therapy or withdrawal of tremelimumab. The data for the following immune-mediated adverse reactions are based on 2280 patients from nine studies across multiple tumour types who received tremelimumab 75 mg every 4 weeks or 1 mg/kg every 4 weeks in combination with durvalumab 1500 mg every 4 weeks, 20 mg/kg every 4 weeks or 10 mg/kg every 2 weeks. This combined safety dataset excludes the POSEIDON Study (and patients treated with tremelimumab in combination with durvalumab and platinum-based chemotherapy). Details for the significant adverse reactions for tremelimumab when given in combination with durvalumab and platinum-based chemotherapy are presented if clinically relevant differences were noted in comparison to tremelimumab in combination with durvalumab.
The data as follows also reflects information for significant adverse reactions for tremelimumab 300 mg in combination with durvalumab in the HCC pool (n=462).
The management guidelines for these adverse reactions are described in Precautions.
Immune-mediated pneumonitis: In the combined safety database with tremelimumab in combination with durvalumab (n=2280), immune-mediated pneumonitis occurred in 86 (3.8%) patients, including Grade 3 in 30 (1.3%) patients, Grade 4 in 1 (<0.1%) patient, and Grade 5 (fatal) in 7 (0.3%) patients. The median time to onset was 57 days (range: 8-912 days). All patients received systemic corticosteroids and 79 of the 86 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Seven patients also received other immunosuppressants. Treatment was discontinued in 39 patients. Resolution occurred in 51 patients.
In the HCC pool (n=462), immune-mediated pneumonitis occurred in 6 (1.3%) patients, including Grade 3 in 1 (0.2%) patient and Grade 5 (fatal) in 1 (0.2%) patient. The median time to onset was 29 days (range: 5-774 days). All patients received systemic corticosteroids, and 5 of the 6 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). One patient also received other immunosuppressants. Treatment was discontinued in 2 patients. Resolution occurred in 3 patients.
Immune-mediated hepatitis: In the combined safety database with tremelimumab in combination with durvalumab (n=2280), immune-mediated hepatitis occurred in 80 (3.5%) patients, including Grade 3 in 48 (2.1%) patients, Grade 4 in 8 (0.4%) patients and Grade 5 (fatal) in 2 (<0.1%) patients. The median time to onset was 36 days (range: 1-533 days). All patients received systemic corticosteroids and 68 of the 80 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Eight patients also received other immunosuppressants. Treatment was discontinued in 27 patients. Resolution occurred in 47 patients.
In the HCC pool (n=462), immune-mediated hepatitis occurred in 34 (7.4%) patients, including Grade 3 in 20 (4.3%) patients, Grade 4 in 1 (0.2%) patient and Grade 5 (fatal) in 3 (0.6%) patients. The median time to onset was 29 days (range: 13-313 days). All patients received systemic corticosteroids, and 32 of the 34 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Nine patients also received other immunosuppressants. Treatment was discontinued in 10 patients. Resolution occurred in 13 patients.
Immune-mediated colitis: In the combined safety database with tremelimumab in combination with durvalumab (n=2280), immune-mediated colitis or diarrhoea occurred in 167 (7.3%) patients, including Grade 3 in 76 (3.3%) patients and Grade 4 in 3 (0.1%) patients. The median time to onset was 57 days (range: 3-906 days). All patients received systemic corticosteroids and 151 of the 167 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Twenty-two patients also received other immunosuppressants. Treatment was discontinued in 54 patients. Resolution occurred in 141 patients.
In the HCC pool (n=462), immune-mediated colitis or diarrhoea occurred in 31 (6.7%) patients, including Grade 3 in 17 (3.7%) patients. The median time to onset was 23 days (range: 2-479 days). All patients received systemic corticosteroids, and 28 of the 31 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Four patients also received other immunosuppressants. Treatment was discontinued in 5 patients. Resolution occurred in 29 patients.
Intestinal perforation was observed in patients receiving tremelimumab in combination with durvalumab (rare) in studies outside of the HCC pool.
Immune-mediated endocrinopathies: Immune-mediated hypothyroidism: In the combined safety database with tremelimumab in combination with durvalumab (n=2280), immune-mediated hypothyroidism occurred in 209 (9.2%) patients, including Grade 3 in 6 (0.3%) patients. The median time to onset was 85 days (range: 1-624 days). Thirteen patients received systemic corticosteroids and 8 of the 13 received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Treatment discontinued in 3 patients. Resolution occurred in 52 patients. Immune-mediated hypothyroidism was preceded by immune-mediated hyperthyroidism in 25 patients or immune-mediated thyroiditis in 2 patients.
In the HCC pool (n=462), immune-mediated hypothyroidism occurred in 46 (10.0%) patients. The median time to onset was 85 days (range: 26-763 days). One patient received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). All patients required other therapy including hormone replacement therapy. Resolution occurred in 6 patients. Immune-mediated hypothyroidism was preceded by immune-mediated hyperthyroidism in 4 patients.
Immune-mediated hyperthyroidism: In the combined safety database with tremelimumab in combination with durvalumab (n=2280), immune-mediated hyperthyroidism occurred in 62 (2.7%) patients, including Grade 3 in 5 (0.2%) patients. The median time to onset was 33 days (range: 4-176 days). Eighteen patients received systemic corticosteroids, and 11 of the 18 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Fifty-three patients required other therapy (thiamazole, carbimazole, propylthiouracil, perchlorate, calcium channel blocker or beta-blocker). One patient discontinued treatment due to hyperthyroidism. Resolution occurred in 47 patients.
In the HCC pool (n=462), immune-mediated hyperthyroidism occurred in 21 (4.5%) patients, including Grade 3 in 1 (0.2%) patient. The median time to onset was 30 days (range: 13-60 days). Four patients received systemic corticosteroids, and all of the four patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Twenty patients required other therapy (thiamazole, carbimazole, propylthiouracil, perchlorate, calcium channel blocker, or beta-blocker). One patient discontinued treatment due to hyperthyroidism. Resolution occurred in 17 patients.
Immune-mediated thyroiditis: In the combined safety database with tremelimumab in combination with durvalumab (n=2280), immune-mediated thyroiditis occurred in 15 (0.7%) patients, including Grade 3 in 1 (<0.1%) patient. The median time to onset was 57 days (range: 22-141 days). Five patients received systemic corticosteroids and 2 of the 5 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Thirteen patients required other therapy including, hormone replacement therapy, thiamazole, carbimazole, propylthiouracil, perchlorate, calcium channel blocker, or beta-blocker. No patients discontinued treatment due to immune-mediated thyroiditis. Resolution occurred in 5 patients.
In the HCC pool (n=462), immune-mediated thyroiditis occurred in 6 (1.3%) patients. The median time to onset was 56 days (range: 7-84 days). Two patients received systemic corticosteroids, and 1 of the 2 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). All patients required other therapy including hormone replacement therapy. Resolution occurred in 2 patients.
Immune-mediated adrenal insufficiency: In the combined safety database with tremelimumab in combination with durvalumab (n=2280), immune-mediated adrenal insufficiency occurred in 33 (1.4%) patients, including Grade 3 in 16 (0.7%) patients and Grade 4 in 1 (<0.1%) patient. The median time to onset was 105 days (range: 20-428 days). Thirty-two patients received systemic corticosteroids, and 10 of the 32 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Treatment was discontinued in one patient. Resolution occurred in 11 patients.
In the HCC pool (n=462), immune-mediated adrenal insufficiency occurred in 6 (1.3%) patients, including Grade 3 in 1 (0.2%) patient. The median time to onset was 64 days (range: 43-504 days). All patients received systemic corticosteroids, and 1 of the 6 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Resolution occurred in 2 patients.
Immune-mediated type 1 diabetes mellitus: In the combined safety database with tremelimumab in combination with durvalumab (n=2280), immune-mediated type 1 diabetes mellitus occurred in 6 (0.3%) patients, including Grade 3 in 1 (<0.1%) patient and Grade 4 in 2 (<0.1%) patients. The median time to onset was 58 days (range: 7-220 days). All patients required insulin. Treatment was discontinued for 1 patient. Resolution occurred in 1 patient.
Immune-mediated type 1 diabetes mellitus was observed in patients receiving tremelimumab in combination with durvalumab (uncommon) in studies outside of the HCC pool.
Immune-mediated hypophysitis/hypopituitarism: In the combined safety database with tremelimumab in combination with durvalumab (n=2280), immune-mediated hypophysitis/hypopituitarism occurred in 16 (0.7%) patients, including Grade 3 in 8 (0.4%) patients. The median time to onset for the events was 123 days (range: 63-388 days). All patients received systemic corticosteroids and 8 of the 16 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Four patients also required endocrine therapy. Treatment was discontinued in 2 patients. Resolution occurred in 7 patients.
In the HCC pool (n=462), immune-mediated hypophysitis/hypopituitarism occurred in 5 (1.1%) patients. The median time to onset for the events was 149 days (range: 27-242 days). Four patients received systemic corticosteroids, and 1 of the 4 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Three patients also required endocrine therapy. Resolution occurred in 2 patients.
Immune-mediated nephritis: In the combined safety database with tremelimumab in combination with durvalumab (n=2280), immune-mediated nephritis occurred in 9 (0.4%) patients, including Grade 3 in 1 (<0.1%) patient. The median time to onset was 79 days (range: 39-183 days). All patients received systemic corticosteroids and 7 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Treatment was discontinued in 3 patients. Resolution occurred in 5 patients.
In the HCC pool (n=462), immune-mediated nephritis occurred in 4 (0.9%) patients, including Grade 3 in 2 (0.4%) patients. The median time to onset was 53 days (range: 26-242 days). All patients received systemic corticosteroids, and 3 of the 4 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Treatment was discontinued in 2 patients. Resolution occurred in 3 patients.
Immune-mediated rash: In the combined safety database with tremelimumab in combination with durvalumab (n=2280), immune-mediated rash or dermatitis (including pemphigoid) occurred in 112 (4.9%) patients, including Grade 3 in 17 (0.7%) patients. The median time to onset was 35 days (range: 1-778 days). All patients received systemic corticosteroids, and 57 of the 112 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). Treatment was discontinued in 10 patients. Resolution occurred in 65 patients.
In the HCC pool (n=462), immune-mediated rash or dermatitis (including pemphigoid) occurred in 26 (5.6%) patients, including Grade 3 in 9 (1.9%) patients and Grade 4 in 1 (0.2%) patient. The median time to onset was 25 days (range: 2-933 days). All patients received systemic corticosteroids and 14 of the 26 patients received high-dose corticosteroid treatment (at least 40 mg prednisone or equivalent per day). One patient received other immunosuppressants. Treatment was discontinued in 3 patients. Resolution occurred in 19 patients.
Infusion-related reactions: In the combined safety database with tremelimumab in combination with durvalumab (n=2280), infusion-related reactions occurred in 45 (2.0%) patients, including Grade 3 in 2 (<0.1%) patients. There were no Grade 4 or 5 events.
Laboratory abnormalities: In patients treated with tremelimumab in combination with durvalumab and platinum-based chemotherapy in the POSEIDON study (n=330), the proportion of patients who experienced a shift from baseline to a Grade 3 or 4 laboratory abnormality was as follows: 6.2% for alanine aminotransferase increased, 5.2% for aspartate aminotransferase increased, 4.0% for blood creatinine increased, 9.4% for amylase increased and 13.6% for lipase increased. The proportion of patients who experienced a TSH shift from baseline that was ≤ ULN to > ULN was 24.8% and a TSH shift from baseline that was ≥ LLN to < LLN was 32.9%.
Immunogenicity: As with all therapeutic proteins, there is a potential for immunogenicity. Immunogenicity of tremelimumab is based on pooled data in 2075 patients who were treated with tremelimumab 75 mg or 1 mg/kg and evaluable for the presence of anti-drug antibodies (ADAs). Two-hundred fifty-two patients (12.1%) tested positive for treatment-emergent ADAs. Neutralising antibodies against tremelimumab were detected in 10.0% (208/2075) patients. The presence of ADAs did not impact tremelimumab pharmacokinetics, and there was no apparent effect safety.
In the HIMALAYA study, of the 182 patients who were treated with tremelimumab 300 mg as a single dose in combination with durvalumab and evaluable for the presence of ADAs against tremelimumab, 20 (11.0%) patients tested positive for treatment-emergent ADAs. Neutralising antibodies against tremelimumab were detected in 4.4% (8/182) patients. The presence of ADAs did not have an apparent effect on pharmacokinetics or safety.
In the POSEIDON study, of the 278 patients who were treated with tremelimumab 75 mg in combination with durvalumab 1500 mg every 3 weeks and platinum-based chemotherapy and evaluable for the presence of ADAs, 38 (13.7%) patients tested positive for treatment-emergent ADAs. Neutralising antibodies against tremelimumab were detected in 11.2% (31/278) of patients. The presence of ADAs did not have an apparent effect on pharmacokinetics or safety.
Elderly: Data from HCC patients 75 years of age or older are limited.
In the POSEIDON study in patients treated with tremelimumab in combination with durvalumab and platinum-based chemotherapy, some differences in safety were reported between elderly (≥65 years) and younger patients. The safety data from patients 75 years of age or older are limited to a total of 74 patients. There was a higher frequency of serious adverse reactions and discontinuation of any study treatment due to adverse reactions in 35 patients aged 75 years of age or older treated with tremelimumab in combination with durvalumab and platinum-based chemotherapy (45.7% and 28.6%, respectively) relative to 39 patients aged 75 years of age or older who received platinum-based chemotherapy only (35.9% and 20.5%, respectively).
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image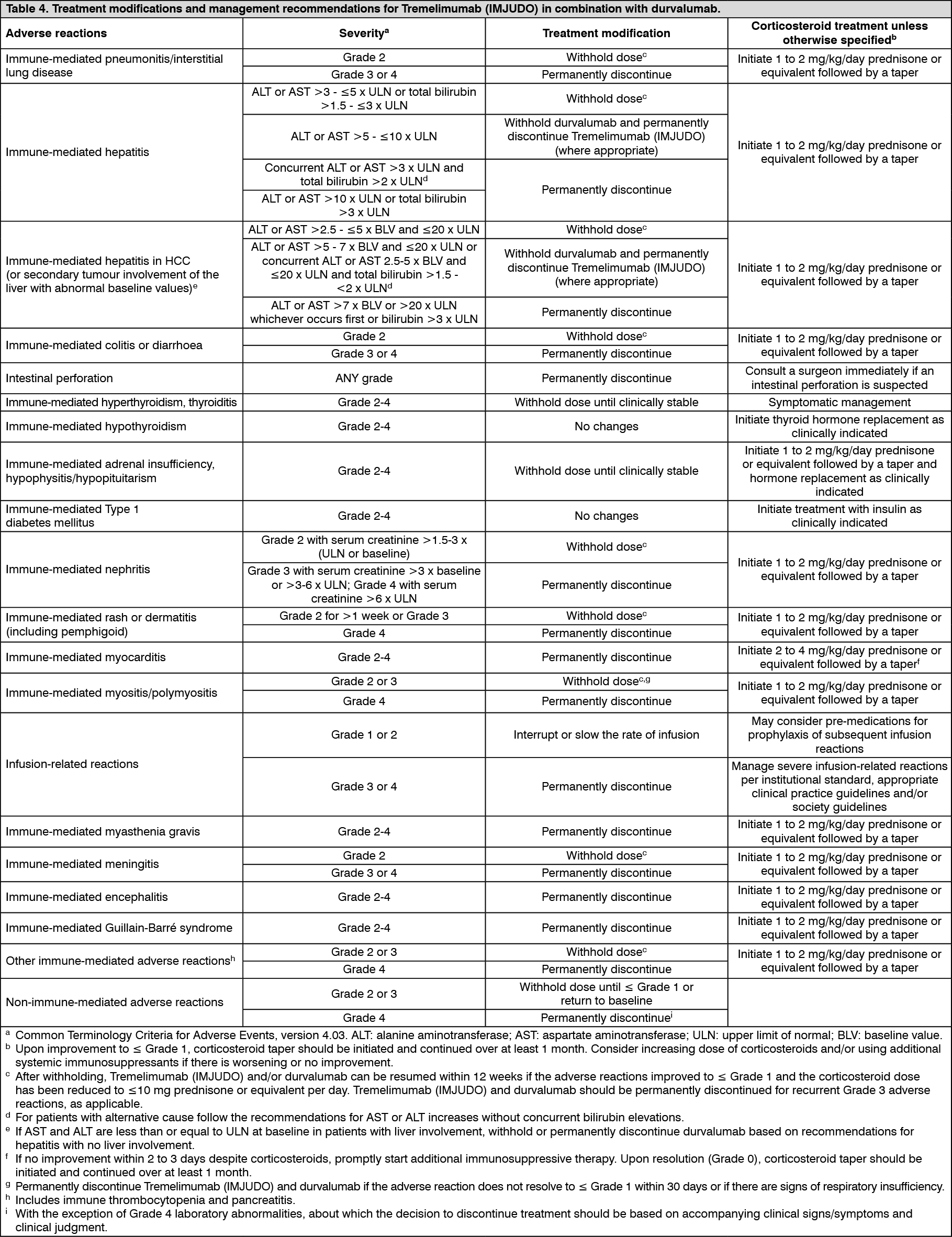 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image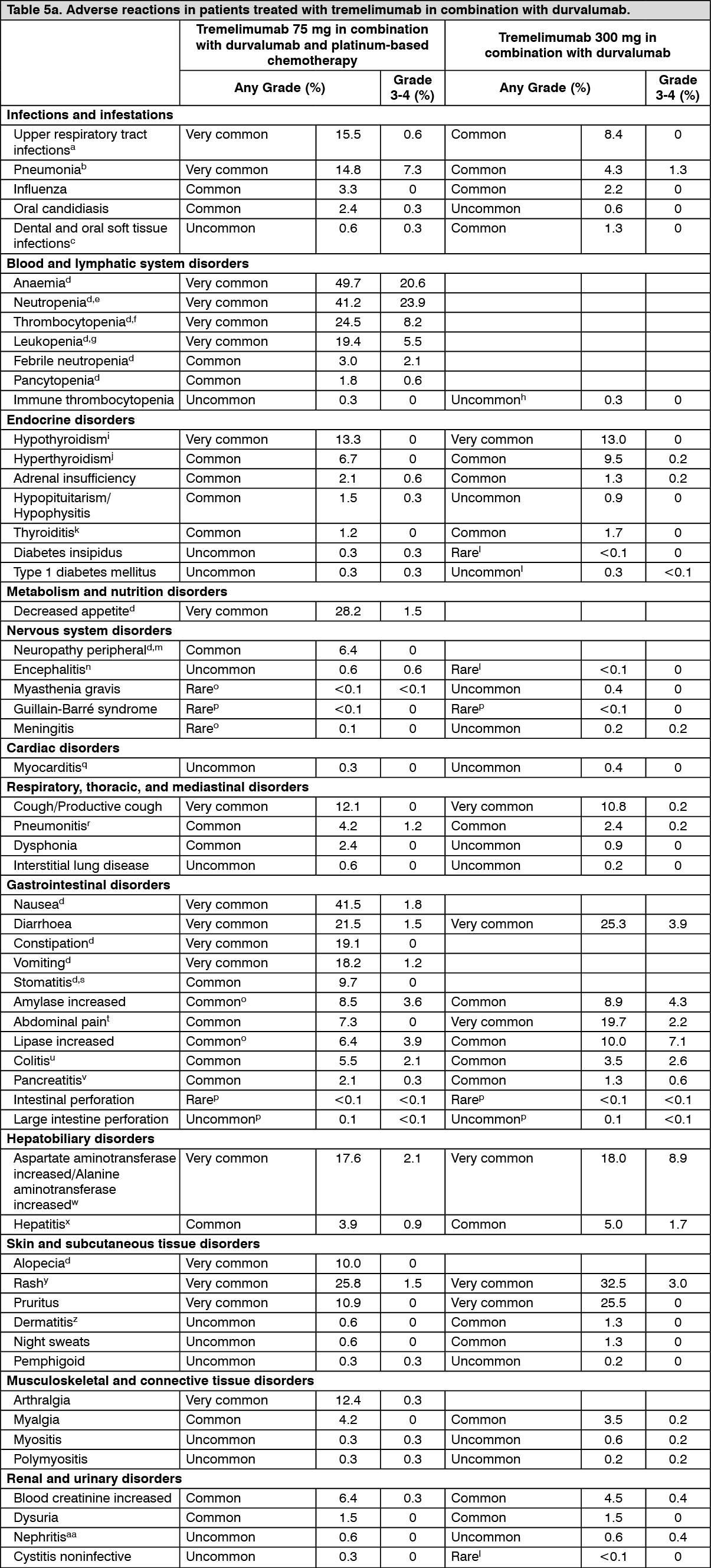 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image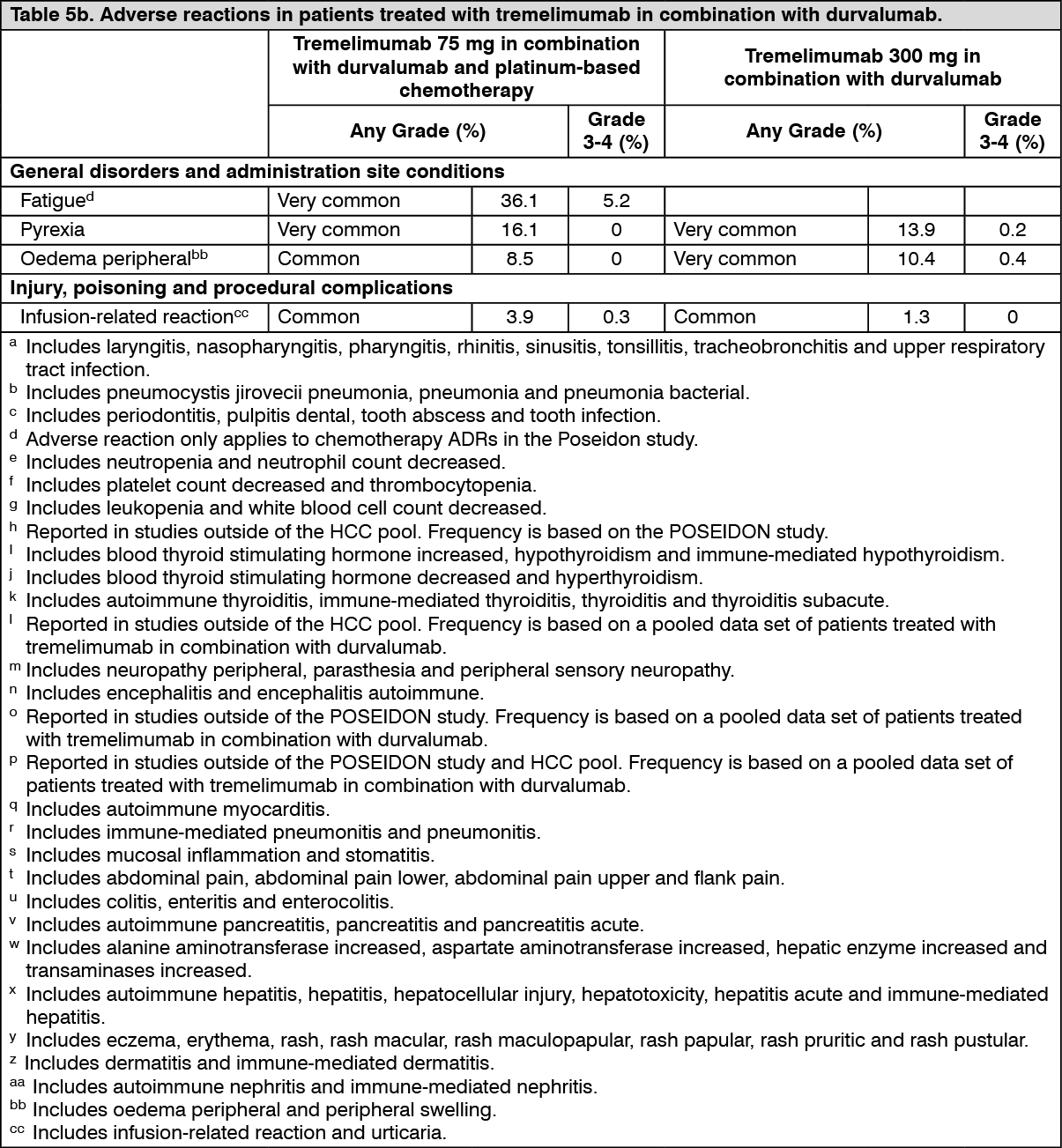 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out