Most common adverse reactions (incidence >28%) are application site reactions or local skin reactions: itching, burning, erythema, flaking/scaling/dryness, scabbing/crusting, edema, induration, excoriation, erosion, ulceration. Other reported reactions (≥1%) include fatigue, fever, and headache.
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Clinical Trials Experience: Actinic Keratosis: The data described as follows reflect exposure to Imiquimod Cream or vehicle in 436 subjects enrolled in two double-blind, vehicle-controlled studies. Subjects applied Imiquimod Cream or vehicle to a 25 cm
2 contiguous treatment area on the face or scalp 2 times per week for 16 weeks (See Tables 3 and 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Local skin reactions were collected independently of the adverse reaction "application site reaction" in an effort to provide a better picture of the specific types of local reactions that might be seen. The most frequently reported local skin reactions were erythema, flaking/scaling/dryness, and scabbing/crusting. The prevalence and severity of local skin reactions that occurred during controlled studies are shown in the following table. (See Table 5.)
Click on icon to see table/diagram/image
The adverse reactions that most frequently resulted in clinical intervention (e.g., rest periods, withdrawal from study) were local and skin application site reactions. Overall, in the clinical studies, 2% (5/215) of subjects discontinued for local skin/application site reactions. Of the 215 subjects treated, 35 subjects (16%) on Imiquimod Cream and 3 of 220 subjects (1%) on vehicle cream had at least one period. Of these Imiquimod Cream subjects, 32 (91%) resumed therapy after a rest period.
In the AK studies, 22 of 678 (3.2%) of Imiquimod-treated subjects developed treatment site infections that required a rest period off Imiquimod Cream and were treated with antibiotics (19 with oral and 3 with topical).
Of the 206 Imiquimod Cream subjects with both baseline and 8-week post-treatment scarring assessments, 6 (2.9%) had a greater degree of scarring scores at 8-weeks post-treatment than at baseline.
Clinical Trials Experience: Superficial Basal Cell Carcinoma: The data described as follows reflect exposure to Imiquimod Cream or vehicle in 364 subjects enrolled in two double-blind, vehicle-controlled studies. Subjects applied Imiquimod Cream or vehicle 5 times per week for 6 weeks. The incidence of adverse reactions reported by > 1% of subjects during the studies is summarized as follows. (See Table 6.)
Click on icon to see table/diagram/image
The most frequently reported adverse reactions were local skin and application site reactions including erythema, edema, induration, erosion, flaking/scaling, scabbing/crusting, itching and burning at the application site. The incidence of application site reactions reported by > 1% of the subject during the 6 week treatment period is summarized in the following table. (See Table 7.)
Click on icon to see table/diagram/image
Local skin reactions were collected independently of the adverse reaction "application site reaction" in an effort to provide a better picture of the specific types of local reactions that might be seen. The prevalence and severity of local skin reactions that occurred during controlled studies are shown in the following table. (See Table 8.)
Click on icon to see table/diagram/image
The adverse reactions that most frequently resulted in clinical interventions (e.g., rest periods, withdrawal from study) were local skin and application site reactions; 10% (19/185) of subjects received rest periods. The average number of doses not received per subject due to rest periods was 7 doses with a range of 2 to 22 doses; 79% of subjects (15/19) resumed therapy after a rest period. Overall, in the clinical studies, 2% (4/185) of subjects discontinued for local skin/application site reactions.
In the sBCC studies, 17 of 1266 (1.3%) Imiquimod-treated subjects developed treatment site infections that required a rest period and treatment with antibiotics.
Clinical Trials Experience: External Genital Warts: In controlled clinical trials for genital warts, the most frequently reported adverse reactions were local skin and application site reactions.
Some subjects also reported systemic reactions. Overall, 1.2% (4/327) of the subjects discontinued due to local skin/application site reactions. The incidence and severity of local skin reactions during controlled clinical trials are shown in the following table. (See Table 9.)
Click on icon to see table/diagram/image
Remote site skin reactions were also reported. The severe remote site skin reactions reported for females were erythema (3%), ulceration (2%), and edema (1%); and for males, erosion (2%), and erythema, edema, induration, and excoriation/flaking (each 1%). Selected adverse reactions judged to be probably or possibly related to Imiquimod Cream are listed as follows. (See Table 10.)
Click on icon to see table/diagram/image
Adverse reactions judged to be possibly or probably related to Imiquimod Cream and reported by more than 1% of subjects included:
Application Site Disorders: burning, hypopigmentation, irritation, itching, pain, rash, sensitivity, soreness, stinging, tenderness.
Remote Site Reactions: bleeding, burning, itching, pain, tenderness, tinea cruris.
Body as a Whole: fatigue, fever, influenza-like symptoms.
Central and Peripheral Nervous System Disorders: headache.
Gastro-Intestinal System Disorders: diarrhea.
Musculo-Skeletal System Disorders: myalgia.
Clinical Trials Experience: Dermal Safety Studies: Provocative repeat insult patch test studies involving induction and challenge phases produced no evidence that Imiquimod Cream causes photoallergenicity or contact sensitization in healthy skin; however, cumulative irritancy testing revealed the potential for Imiquimod Cream to cause irritation, and application site reactions were reported in the clinical studies.
Post-marketing Experience: The following adverse reactions have been identified during post-approval use of Imiquimod Cream. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. (See Table 11.)
Click on icon to see table/diagram/image



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image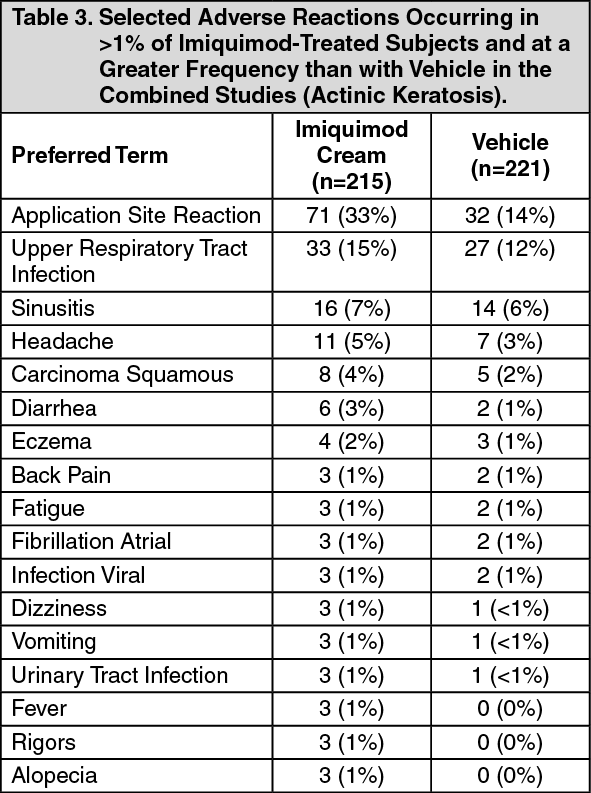 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image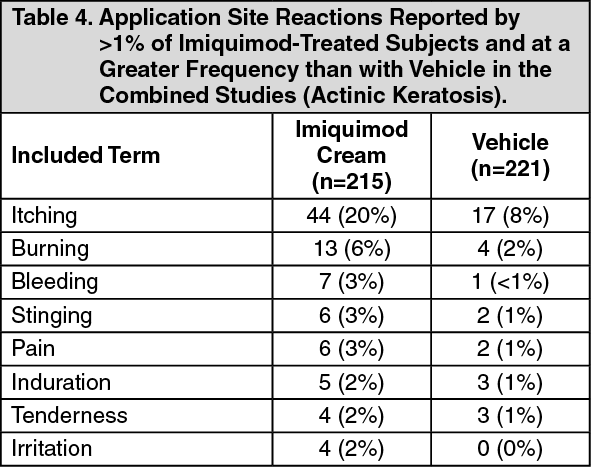 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image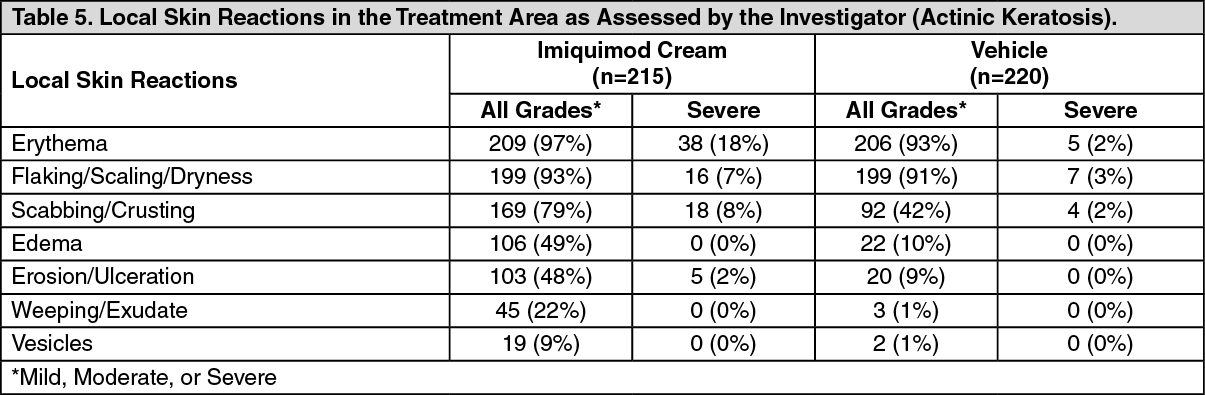 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image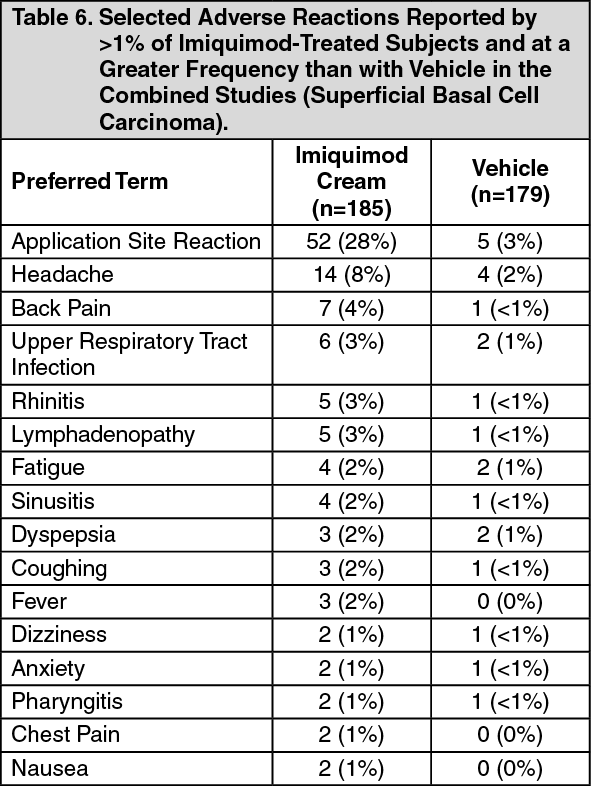 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image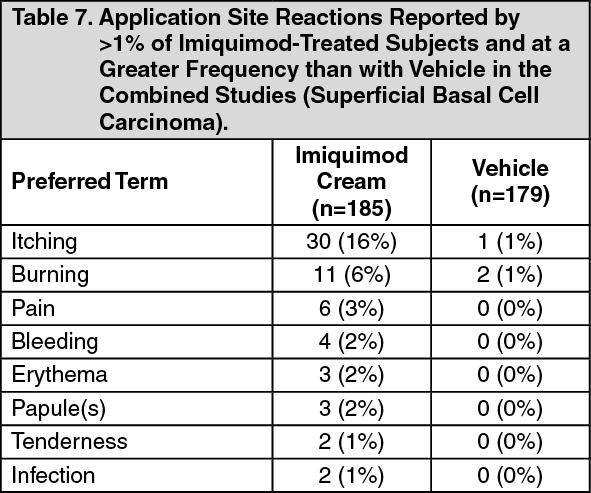 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image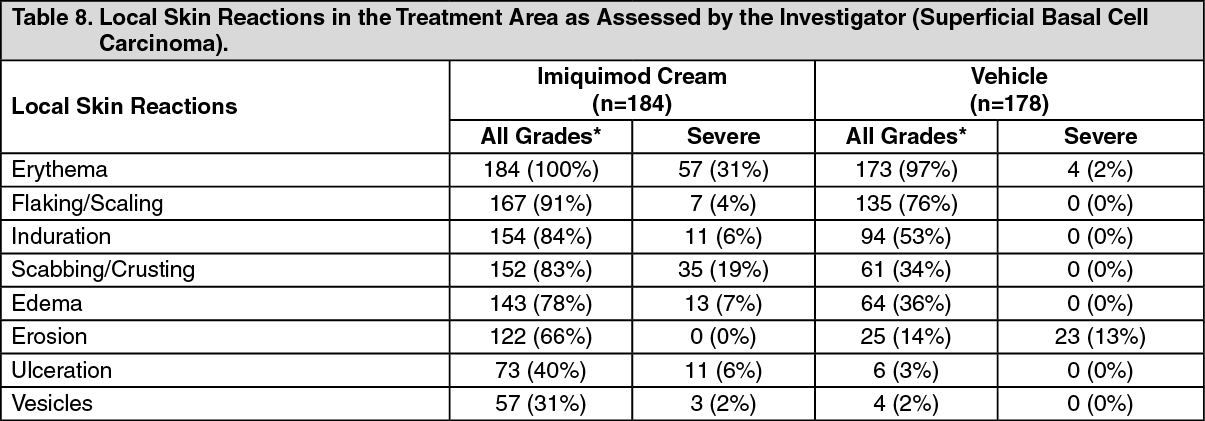 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image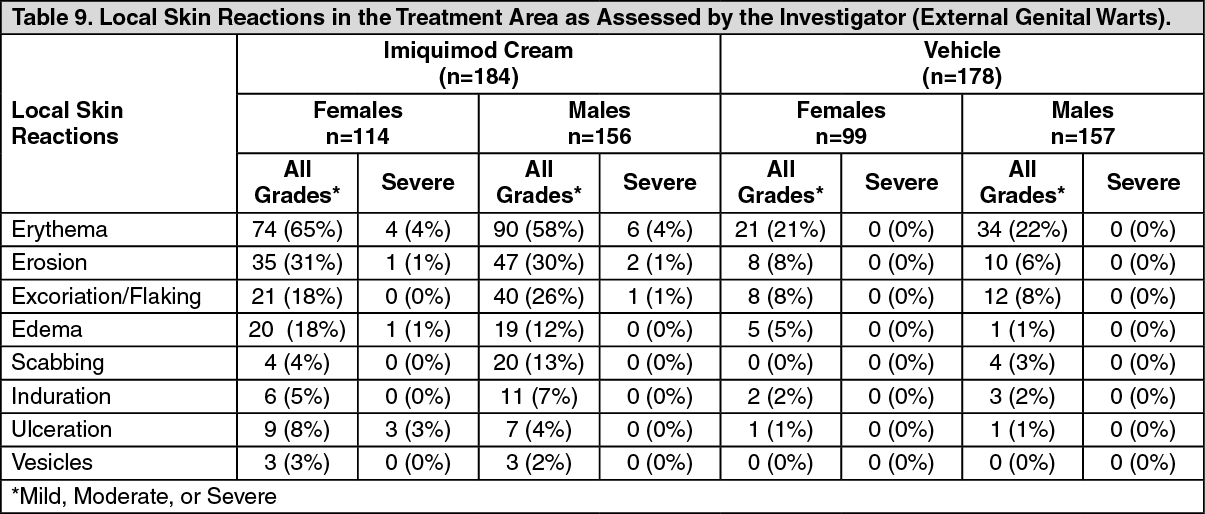 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image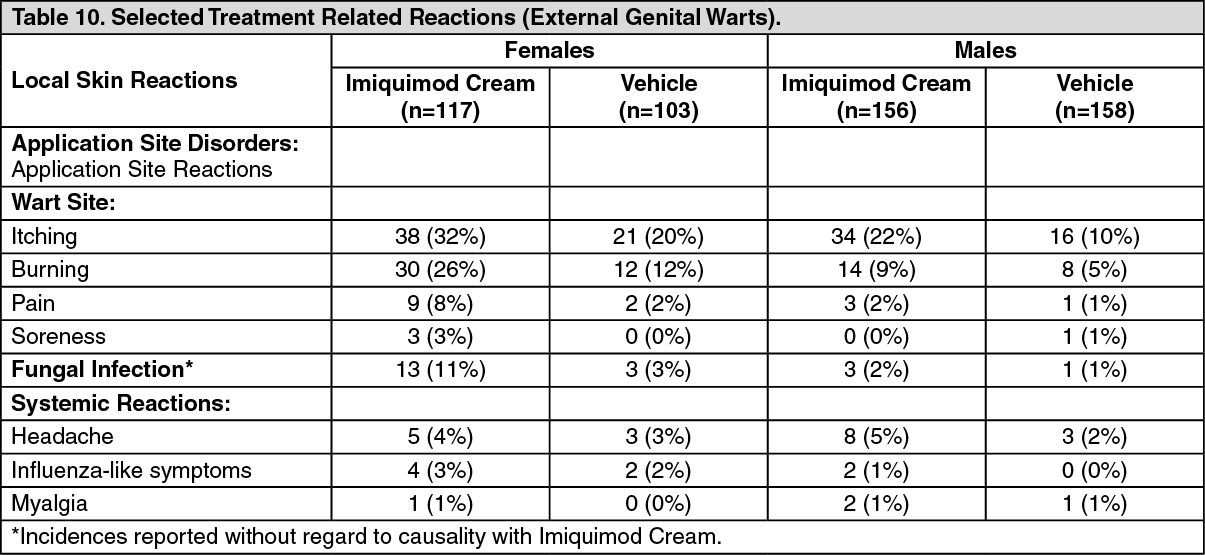 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image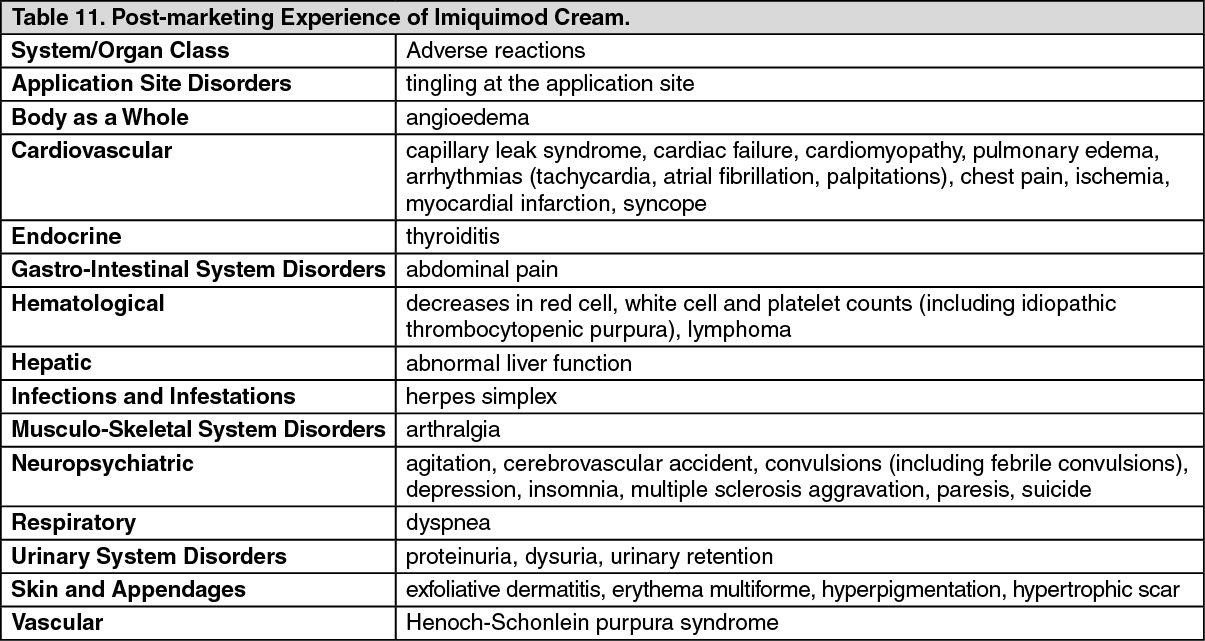 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out