Pharmacology: General: Adalimumab binds specifically to TNF and neutralizes the biological function of TNF by blocking its interaction with the p55 and p75 cell surface TNF receptors. TNF is a naturally occurring cytokine that is involved in normal inflammatory and immune responses. Elevated levels of TNF are found in the synovial fluid of rheumatoid arthritis, including juvenile idiopathic arthritis, psoriatic arthritis and ankylosing spondylitis patients and play an important role in both the pathologic inflammation and the joint destruction that are hallmarks of these diseases. Increased levels of TNF are also found in hidradenitis suppurativa (HS) lesions. The relationship between these pharmacodynamic activities and the mechanism(s) by which Humira exerts its clinical effects is unknown.
Adalimumab also modulates biological responses that are induced or regulated by TNF, including changes in the levels of adhesion molecules responsible for leukocyte migration (ELAM-1, VCAM-1, and ICAM-1 with an IC
50 of 1-2 X 10
-10M).
Pharmacodynamics: After treatment with Humira, a rapid decrease in levels of acute phase reactants of inflammation (C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR)) and serum cytokines (IL-6)) was observed compared to baseline in patients with RA. A decrease in CRP levels was also observed in patients with JIA, Crohn's disease, ulcerative colitis and hidradenitis suppurativa as well as a significant reduction in the expression of the TNF and inflammatory markers such as human leucocyte antigen (HLA-DR) and myeloperoxidase (MPO) in the colon of patients with Crohn's disease. Serum levels of matrix metalloproteinases (MMP-1 and MMP-3) that produce tissue remodeling responsible for cartilage destruction were also decreased after Humira administration. Patients with RA, PsA and AS often experience mild to moderate anemia and decreased lymphocyte counts, as well as elevated neutrophil and platelet counts. Patients treated with Humira usually experienced improvement in these hematological signs of chronic inflammation.
The serum adalimumab concentration-efficacy relationship as measured by the American College of Rheumatology response criteria (ACR 20) appears to follow the Hill E
max equation as shown as follows: See Figure 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
EC
50 estimates ranging from 0.8 to 1.4 mcg/mL were obtained through pharmacokinetic/pharmacodynamic modeling of swollen joint count, tender joint count and ACR 20 response from patients participating in Phase II and III trials.
Clinical Studies: Adults: Rheumatoid Arthritis Clinical Studies: Humira was evaluated in over 3000 patients in all rheumatoid arthritis clinical trials. The efficacy and safety of Humira were assessed in five randomized, double-blind and well-controlled studies. Some patients were treated for up to 120 months duration. Injection site pain of Humira 40 mg/0.4 mL compared to Humira 40 mg/0.8 mL was assessed in two randomized, active control, single-blind, two period crossover studies.
RA Study I (DE009) evaluated 271 patients with moderately to severely active RA who were ≥18 years old, had failed therapy with at least one but no more than four disease-modifying anti-rheumatic drugs (DMARDs) (e.g., hydroxychloroquine, oral or injectable gold, azathioprine, D-penicillamine, sulfasalazine), and had insufficient efficacy with MTX at doses of 12.5 to 25 mg (10 mg if MTX-intolerant) every week and whose MTX dose remained constant at 10 to 25 mg every week. Patients had ≥6 swollen joints and ≥9 tender joints and RA diagnosed according to ACR criteria. Doses of 20, 40 or 80 mg of Humira or placebo were given every other week for 24 weeks.
RA Study II (DE011) evaluated 544 patients with moderately to severely active RA who were ≥18 years old and had failed therapy with at least one DMARD (e.g., MTX, sulfasalazine, hydroxychloroquine, oral or injectable gold, D-penicillamine, azathioprine). Patients had ≥10 swollen joints and ≥12 tender joints and were also diagnosed according to ACR criteria. Doses of 20 or 40 mg of Humira were given by SC injection every other week with placebo on alternative weeks or every week for 26 weeks; placebo was given every week for the same duration.
RA Study III (DE019) evaluated 619 patients with moderately to severely active RA who were ≥18 years old, had insufficient efficacy to MTX at doses of 12.5 to 25 mg (10 mg if MTX-intolerant) every week and whose MTX dose remained constant at 12.5 to 25 mg every week. Unlike RA Study I, patients in RA Study III were not required to have failed therapy with any DMARDs other than MTX. Patients had ≥6 swollen joints and ≥9 tender joints and RA diagnosed according to ACR criteria. There were three groups in this study. The first received placebo injections every week for 52 weeks. The second received 20 mg of Humira every week for 52 weeks. The third group received 40 mg of Humira every other week with placebo injections on alternate weeks. Upon completion of the first 52 weeks, 457 patients enrolled in an open-label extension phase in which 40 mg of Humira/MTX was administered every other week up to 10 years.
RA Study IV (DE031) assessed 636 patients with moderately to severely active RA who were ≥18 years old. These patients met the ACR criteria for diagnosis of RA for at least three months and had at least 6 swollen joints and 9 tender joints. Patients were permitted to be either DMARD-naive or to remain on their pre-existing rheumatologic therapy provided that therapy was stable for a minimum of 28 days. Patients were randomized to 40 mg of Humira or placebo every other week for 24 weeks.
RA Study V (DE013) evaluated 799 methotrexate-naive, adult patients with moderately to severely active early rheumatoid arthritis (mean disease duration less than 9 months). This study evaluated the efficacy of Humira 40 mg every other week/methotrexate combination therapy, Humira 40 mg every other week monotherapy and methotrexate monotherapy in reducing the signs and symptoms and rate of progression of joint damage in rheumatoid arthritis for 104 weeks. Upon completion of the first 104 weeks, 497 patients enrolled in an open-label extension phase in which 40 mg of Humira was administered every other week up to 10 years.
RA Studies VI and VII each evaluated 60 patients with moderately to severely active rheumatoid arthritis who were ≥18 years old. Enrolled patients were either current users of Humira 40 mg/0.8 mL and rated their average injection site pain as at least 3 cm (on a 0-10 cm VAS) or were biologic-naïve subjects who were starting Humira 40 mg/0.8 mL. Patients were randomized to receive a single dose of Humira 40 mg/0.8 mL or Humira 40 mg/0.4 mL, followed by a single injection of the opposite treatment at their next dose.
Results of all RA Study I-V were expressed in percentage of patients with improvement in RA using ACR response criteria. The primary end point in RA Studies I, II and III and the secondary endpoint in RA Study IV was the percent of patients who achieved an ACR 20 response at Week 24 or 26. The primary endpoint in RA Study V was the percent of patients who achieved an ACR 50 response at Week 52. RA Study III and V had an additional primary endpoint at 52 weeks of retardation of disease progression (as detected by x-ray results). RA Study III also had a primary endpoint of changes in quality of life. The primary endpoint in RA studies VI and VII was injection site pain immediately after injection as measured by a 0-10 cm VAS.
Clinical Response: RA Studies I, II and III: The percent of Humira treated patients achieving ACR 20, 50 and 70 responses was consistent across all three trials. The results of the three trials are summarized in Table 1. (See Table 1.)
Click on icon to see table/diagram/image
Patients receiving Humira 40 mg every week in RA Study II also achieved statistically significant ACR 20, 50 and 70 response rates of 53.4%, 35.0% and 18.4%, respectively, at six months.
The results of the components of the ACR response criteria for RA Study III are shown in Table 2. The results depicted as follows are generally representative of each trial conducted.
In the open-label extension for RA Study III, most patients who were ACR responders maintained response when followed for up to 10 years. Of 207 patients who were randomized to Humira 40 mg every other week, 114 patients continued on Humira 40 mg every other week for 5 years. Among those, 86 patients (75.4%) had ACR 20 responses; 72 patients (63.2%) had ACR 50 responses; and 41 patients (36%) had ACR 70 responses. Of 207 patients, 81 patients continued on Humira 40 mg every other week for 10 years. Among those, 64 patients (79.0%) had ACR 20 responses; 56 patients (69.1%) had ACR 50 responses; and 43 patients (53.1%) had ACR 70 responses. (See Table 2.)
Click on icon to see table/diagram/image
In RA Study III, 84.7% of patients with ACR 20 responses at Week 24 maintained the response at 52 weeks. The following figures illustrate the durability of ACR 20 responses to Humira in RA Studies III and II. (See Figures 2 and 3.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
RA Study IV: The ACR 20 response of patients treated with Humira plus standard of care was statistically significantly better than patients treated with placebo plus standard of care (p<0.001). No unique adverse reactions related to the combination of Humira and other DMARDs were observed.
In RA Studies I-IV, Humira treated patients achieved ACR 20, 50 and 70 responses faster and more often than placebo-treated patients. In RA Study I, there was a statistically significant difference in ACR 20 responses at week one (first study visit) between patients treated with Humira (26.0%) and placebo (5.0%). Statistically significant differences in ACR 20 responses were also seen in RA Studies II, III and IV at week two (first study visit) between patients treated with Humira (36.4%, 29.1% and 33.7%, respectively) and placebo (7.3%, 13.0% and 8.6%, respectively). A similar pattern of the time to first ACR 50 and 70 responses was noted in all four studies.
Some patients not taking concomitant MTX may derive additional benefit from increasing the dosing frequency of Humira to 40 mg every week. This was confirmed in a long-term open label study where patients with an incomplete response increased their dosing frequency from 40 mg every other week to 40 mg weekly.
RA Study V: In RA Study V with early rheumatoid arthritis patients who were methotrexate naive, combination therapy with Humira and methotrexate led to faster and significantly greater ACR responses than methotrexate monotherapy and Humira monotherapy at Week 52 and responses were sustained through Week 104 (see Table 3).
At Week 52 all individual components of the ACR response criteria improved with Humira/methotrexate therapy and improvements were maintained to Week 104.
Over the two-year study, 48.5 % of patients who received Humira/methotrexate combination therapy achieved a major clinical response (ACR 70 for six continuous months) compared to 27.2% of patients who received methotrexate monotherapy (p<0.001) and 24.5% of patients who received Humira monotherapy (p<0.001). (See Table 3.)
Click on icon to see table/diagram/image
In the open-label extension for RA study V, ACR response rates were maintained when followed for up to 10 years. Of 542 patients who were randomized to Humira 40 mg every other week, 170 patients continued on Humira 40 mg every other week for 10 years. Among those, 154 patients (90.6%) had ACR 20 responses; 127 patients (74.7%) had ACR 50 responses; and 102 patients (60.0%) had ACR 70 responses.
At week 52, 42.9% of patients who received Humira/methotrexate combination therapy achieved clinical remission (Disease Activity Score (DAS28)-CRP <2.6) compared to 20.6% of patients receiving methotrexate monotherapy and 23.4% of patients receiving Humira monotherapy. Humira/methotrexate combination therapy was statistically and clinically superior to methotrexate (p<0.001) and Humira monotherapy (p<0.001) in achieving a low disease state in patients with recently diagnosed moderate to severe rheumatoid arthritis (see Table 4). Of 342 subjects originally randomized to Humira monotherapy or Humira/methotrexate combination therapy who entered the open-label extension study, 171 subjects completed 10 years of Humira treatment. Among those, 109 subjects (63.7%) were reported to be in remission at 10 years. (See Table 4.)
Click on icon to see table/diagram/image
Radiographic Response: In RA Study III, where Humira treated patients had a mean duration of rheumatoid arthritis of approximately 11 years, structural joint damage was assessed radiographically and expressed as change in modified total Sharp score and its components, the erosion score and joint space narrowing score (JSN). Radiographs of hands/wrists and forefeet were read at baseline, 6 months and 12 months. The 12-month results are shown in Table 5. A statistically significant difference for change in modified total Sharp score (TSS) and the erosion score was observed at 6 months and maintained at 12 months. Humira/MTX treated patients demonstrated less radiographic progression than patients receiving MTX alone at 52 weeks. The inhibition of progression of structural damage was maintained through 104 weeks. (See Table 5.)
Click on icon to see table/diagram/image
In the open-label extension of RA Study III, the reduction in rate of progression of structural damage is maintained for 8 and 10 years in a subset of patients. At 8 years, 81 of 207 patients originally treated with Humira 40 mg every other week were evaluated radiographically. Among those, 48 patients showed no progression of structural damage defined by a change from baseline in the mTSS of 0.5 or less. At 10 years, 79 of 207 patients originally treated with Humira 40 mg every other week were evaluated radiographically. Among those, 40 patients showed no progression of structural damage defined by a change from baseline in the mTSS of 0.5 or less.
In RA Study V, structural joint damage was assessed as in RA Study III. Greater inhibition of radiographic progression, as assessed by changes in TSS, erosion score and JSN was observed in the Humira/MTX combination group as compared to either the MTX or Humira monotherapy group at Week 52 as well as at Week 104 (see Table 6).
Click on icon to see table/diagram/image
Following 52 weeks and 104 weeks of treatment, the percentage of patients without progression (change from baseline in modified total Sharp score <0.5) was significantly higher with Humira/MTX combination therapy (63.8% and 61.2% respectively) compared to methotrexate monotherapy (37.4% and 33.5% respectively, p<0.001) and Humira monotherapy (50.7%, p<0.002 and 44.5%, p<0.001 respectively).
In the open-label extension of RA study V, the mean change from baseline at Year 10 in the modified Total Sharp Score was 10.8, 9.2 and 3.9 in patients originally randomized to methotrexate monotherapy, Humira monotherapy and Humira/methotrexate combination therapy, respectively. The corresponding proportions of patients with no radiographic progression were 31.3%, 23.7% and 36.7% respectively.
Quality of Life and Physical Function: Health-related quality of life was assessed using the disability index of the Health Assessment Questionnaire (HAQ) in the four original adequate and well-controlled trials, which was a pre-specified primary endpoint at Week 52 in RA Study III. All doses/schedules of Humira in all four studies showed statistically significantly greater improvement in the disability index of the HAQ from baseline to Month 6 compared to placebo. In RA Study III, the mean (CI) improvement in HAQ from baseline at week 52 was -0.60 (-0.65, -0.55) for the Humira/MTX patients and -0.25 (-0.33, -0.17) for placebo/MTX (p<0.001) patients. Sixty-three percent of Humira/MTX-treated patients achieved a 0.5 or greater improvement in HAQ at week 52 in the double-blind portion of the study. Most subjects who achieved improvement in physical function and continued treatment-maintained improvement through week 520 (10 years) of open-label treatment. Improvement in quality of life as measured by SF 36 was assessed up to Week 156 (36 months) and improvement was maintained through that time.
The Short Form Health Survey (SF 36) was also used to assess general health-related quality of life in all four adequate and well-controlled trials. All doses/schedules of Humira in all four studies showed statistically significantly greater improvement in SF 36 physical component summary scores from baseline to Month 6 compared to placebo, and this was maintained at Week 52 in RA Study III. Mean improvement in the SF 36 was also maintained through the end of measurement at week 156 (36 months). The SF 36 mental component summary scores in RA Studies II and IV were also statistically significantly greater at Month 6 for Humira vs. placebo. The pain and vitality domain scores of the SF 36 showed statistically significantly greater improvement from baseline to Month 6 in all four studies for the 40 mg every other week dose of Humira compared to placebo. These findings were supported by functional assessment of chronic illness therapy (FACIT) scores that showed a statistically significant decrease in fatigue at Month 6 in all three studies analyzed that was maintained at Week 52 in RA Study III.
In RA Study V the improvement in the HAQ disability index and the physical component of the SF 36 was greater for the Humira/methotrexate combination therapy group versus both methotrexate and Humira monotherapy groups (p<0.001) at Week 52; this improvement was maintained through Week 104. Among the 250 subjects who completed the open-label extension study, improvements in physical function were maintained through 10 years of treatment.
Injection Site Pain: For the pooled crossover RA studies VI and VII, a statistically significant difference for injection site pain immediately after dosing was observed between Humira 40 mg/0.8 mL and Humira 40 mg/0.4 mL (mean VAS of 3.7 cm versus 1.2 cm, scale of 0-10 cm, P <0.001). This represented an 84% median reduction in injection site pain.
Psoriatic Arthritis Clinical Studies: The safety and efficacy of Humira was assessed in two randomized, double-blind, placebo-controlled studies in 413 patients with psoriatic arthritis. PsA Study I (M02-518) enrolled 313 adult patients with moderately to severely active psoriatic arthritis (>3 swollen and >3 tender joints) who had an inadequate response to NSAID therapy in one of the following forms: (1) distal interphalangeal (DIP) involvement (N=23); (2) polyarticular arthritis (absence of rheumatoid nodules and presence of psoriasis) (N=210); (3) arthritis mutilans (N=1); (4) asymmetric psoriatic arthritis (N=77); or (5) ankylosing spondylitis-like (N=2). Patients on MTX therapy (158 of 313 patients) at enrollment (stable dose of <30 mg/week for >1 month) could continue MTX at the same dose. Doses of Humira 40 mg or placebo every other week were administered during the 24-week double-blind period of the study. PsA Study II (M02-570) with 12-week duration, treated 100 patients who had an inadequate response to DMARD therapy. Upon completion of both studies, 383 patients enrolled in an open-label extension study, in which 40 mg Humira was administered eow.
ACR and PASI Response: Compared to placebo, treatment with Humira resulted in improvements in the measures of disease activity (see Tables 7 and 8). Among patients with psoriatic arthritis who received Humira, the clinical responses were apparent in some patients at the time of the first visit (two weeks). Similar responses were seen in patients with each of the subtypes of psoriatic arthritis, although few patients were enrolled with the arthritis mutilans and ankylosing spondylitis-like subtypes. Responses were similar in patients who were or were not receiving concomitant MTX therapy at baseline.
Patients with psoriatic involvement of at least three percent body surface area (BSA) were evaluated for Psoriatic Area and Severity Index (PASI) responses. At 24 weeks, the proportions of patients achieving a 75% or 90% improvement in the PASI were 59% and 42% respectively, in the Humira group (N=69), compared to 1% and 0% respectively, in the placebo group (N=69) (p<0.001). PASI responses were apparent in some patients at the time of the first visit (two weeks). Responses were similar in patients who were or were not receiving concomitant MTX therapy at baseline. (See Tables 7 and 8.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Similar results were seen in an additional, 12-week study in 100 patients with moderate to severe psoriatic arthritis who had suboptimal response to DMARD therapy as manifested by >3 tender joints and >3 swollen joints at enrolment.
Radiographic Response: Radiographic changes were assessed in the psoriatic arthritis studies. Radiographs of hands, wrists and feet were obtained at baseline and Week 24 during the double-blind period when patients were on Humira or placebo and at Week 48 when all patients were on open-label Humira. A modified Total Sharp Score (mTSS), which included distal interphalangeal joints (i.e., not identical to the TSS used for rheumatoid arthritis), was used.
Humira treatment reduced the rate of progression of peripheral joint damage compared with placebo treatment as measured by change from baseline in mTSS score (mean ± SD) 0.8 ± 2.5 in the placebo group (at week 24) compared with 0.0 ± 1.9 in the Humira group (at week 48) (p <0.001).
In subjects treated with Humira with no radiographic progression from baseline to Week 48 (n=102), 84% continued to show no radiographic progression through 144 weeks of treatment.
Quality of Life and Physical Function: Humira treated patients demonstrated statistically significant improvement in physical function as assessed by HAQ and Short Form Health Survey (SF 36) compared to placebo at week 24. Improved physical function continued during the open label extension up to week 136.
Ankylosing Spondylitis Clinical Studies: The safety and efficacy of Humira 40 mg fortnightly was assessed in 393 adult patients in two randomized, 24-week double-blind, placebo-controlled studies in patients with active ankylosing spondylitis (AS). The larger study (AS Study I or M03-607) enrolled 315 adult patients with active AS (defined as fulfilling at least two of the following three criteria: (1) a Bath AS disease activity index (BASDAI) score ≥4 cm, (2) a visual analog score (VAS) for total back pain ≥40 mm, (3) morning stiffness ≥1 hour, who had an inadequate response to conventional therapy. Seventy-nine (20.1%) patients were treated concomitantly with disease modifying anti-rheumatic drugs, and 37 (9.4%) patients with glucocorticoids. The blinded period was followed by an open label period during which patients receive Humira every other week subcutaneously for up to an additional 236 weeks. Subjects (N=215, 54.7%) who failed to achieve ASAS 20 at Weeks 12, or 16 or 20 received early escape open-label adalimumab 40mg fortnightly SC and were subsequently treated as non-responders in double-blind statistical analyses.
Results showed statistically significant improvement of signs and symptoms of AS in patients treated with Humira compared to placebo. Significant improvement in measures of disease activity was first observed at Week 2 and maintained through 24 weeks as shown in Figure 4 and Table 9.
Patients with total spinal ankylosis were included in the larger study (n=11). Responses of these patients were similar to those without total ankylosis. (See Figure 4 and Table 9.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
A low level of disease activity (defined as a value <20 [on a scale of 0-100 mm] in each of the four ASAS response parameters) was achieved at 24 weeks in 22% of Humira-treated patients vs. 6% in placebo-treated patients (p<0.001). (See Table 10.)
Click on icon to see table/diagram/image
Similar trends (not all statistically significant) were seen in the smaller randomized, double-blind, placebo-controlled study (AS Study II or M03-606) of 82 patients with active ankylosing spondylitis.
Patient Reported Outcomes were assessed in both ankylosing spondylitis studies using the generic health status questionnaire SF-36 and the disease specific Ankylosing Spondylitis Quality of Life Questionnaire (ASQoL). The Humira-treated patients had significantly greater improvement in SF-36 Physical Component Score (mean change: 6.93) compared to placebo-treated patients (mean change: 1.55; p<0.001) at Week 12, which was maintained through Week 24 (mean change 7.44 vs 1.85).
Results from the ASQoL support these findings demonstrating improvement in overall quality of life. The Humira-treated patients had statistically significant improvement (mean change: -3.15) compared to placebo-treated patients (mean change: -0.95; p<0.001) at Week 12, which was maintained through Week 24 (mean change -3.58 vs -1.06).
Adult Crohn's Disease Clinical Studies: The safety and efficacy of multiple doses of Humira were assessed in over 1400 patients with moderately to severely active Crohn's disease (Crohn's Disease Activity Index (CDAI) ≥220 and ≤450) in randomized, double-blind, placebo controlled studies. Concomitant stable doses of aminosalicylates, corticosteroids, and/or immunomodulatory agents were permitted and 79% of patients continued to receive at least one of these medications.
Induction of clinical remission (defined as CDAI <150) was evaluated in two studies. In CD Study I (M02-403, CLASSIC I), 299 TNF-antagonist naïve patients were randomized to one of four treatment groups; the placebo group received placebo at weeks 0 to 2, the 160/80 group received 160mg Humira at Week 0 and 80mg at Week 2, the 80/40 group received 80mg at Week 0 and 40mg at Week 2, and the 40/20 group received 40mg at Week 0 and 20mg at Week 2. Clinical results were assessed at Week 4.
In the second induction study, CD Study II (M04-691, GAIN), 325 patients who had lost response or were intolerant to, previous infliximab were randomized to receive either 160mg Humira at Week 0 and 80mg at Week 2, or placebo at Weeks 0 and 2. Clinical results were assessed at Week 4.
Maintenance of clinical remission was evaluated in CD Study III (M02-404, CHARM). In this study, 854 patients with active disease received open-label 80 mg Humira at Week 0 and 40 mg at Week 2. Patients were then randomized at Week 4 to 40 mg Humira every other week, 40 mg Humira every week or placebo with a total study duration of 56 weeks. Patients in clinical response (CR-70 = decrease in CDAI ≥70) at Week 4 were stratified and analysed separately from those not in clinical response at Week 4. Corticosteroid taper was permitted after Week 8.
Clinical Results: Induction of Clinical Remission: A statistically significantly greater percentage of the patients treated with 160/80mg Humira achieved induction of clinical remission versus placebo at Week 4 regardless of whether the patients were TNF antagonist naïve (CD Study I), or had been previously exposed to infliximab (CD Study II) (see Table 11).
Click on icon to see table/diagram/image
Maintenance of Clinical Remission: In CD Study III, at Week 4, 58% (499/854) patients were in clinical response (decrease in CDAI ≥70 points) and were assessed in the primary analysis. Of those in clinical response at Week 4, 48% had been previously exposed to other anti-TNF therapy. At Weeks 26 and 56, statistically significantly greater proportions of patients who were in clinical response at Week 4 achieved clinical remission in the Humira maintenance group compared to patients in the placebo maintenance group. Additionally, statistically significantly greater proportions of patients receiving concomitant corticosteroids at baseline were in clinical remission and were able to discontinue corticosteroid use for at least 90 days in the Humira maintenance groups compared to patients in the placebo maintenance group at Weeks 26 and 56 (see Table 12). The group that received Humira every week did not show significantly higher remission rates than the group that received Humira every other week.
Clinical remission results presented in Table 12 remained relatively constant irrespective of previous TNF antagonist exposure. (See Table 12.)
Click on icon to see table/diagram/image
Of those in response at Week 4 who attained remission during the study, patients in Humira maintenance groups-maintained remission for a significantly longer time than patients in the placebo maintenance group. Disease-related hospitalizations and surgeries were statistically significantly reduced with Humira compared with placebo at Week 56.
Among patients who were not in response by Week 12, therapy continued beyond 12 weeks did not result in significantly more responses.
117/276 patients from CD study I and 272/777 patients from CD studies II and III were followed through at least 3 years of open-label Humira therapy. 88 (75.2%) and 189 (69.5%) patients, respectively, continued to be in clinical remission. Clinical response (CR-70) was maintained in 107 (91.5%) and 248 (91.2%) patients, respectively.
An endoscopy study (M05-769, EXTEND), which enrolled 135 patients, with moderate to severe Crohn's disease, indicated an effect of Humira on mucosal healing. 27.4% of patients treated with Humira had mucosal healing at Week 12 compared to 13.1% of patients given placebo (p=0.056), and 24.2% of patients treated with Humira had mucosal healing at Week 52 compared to 0% of patients given placebo (p<0.001).
Quality of Life: In CD Study I and CD Study II, statistically significant improvement in the disease-specific inflammatory bowel disease questionnaire (IBDQ) total score was achieved at week 4 in patients randomized to Humira 80/40 mg and 160/80 mg compared to placebo and was seen at weeks 26 and 56 in CD study III as well among the Humira treatment groups compared to the placebo group.
Ulcerative Colitis Clinical Studies: The safety and efficacy of multiple doses of Humira were assessed in adult patients with moderately to severely active ulcerative colitis (Mayo score 6 to 12 with endoscopy subscore of 2 to 3 points) in two randomized, double-blind, placebo-controlled studies. Concomitant stable doses of aminosalicylates, corticosteroids, and/or immunomodulatory agents were permitted.
Induction of clinical remission (defined as Mayo ≤2 with no subscore >1) was evaluated in Study UC-I. In Study UC-I, 390 TNF-antagonist naïve patients were randomized to receive either placebo at Weeks 0 and 2, 160 mg Humira at Week 0 followed by 80 mg at Week 2, or 80 mg Humira at Week 0 followed by 40 mg at Week 2. After Week 2, patients in both adalimumab arms received 40 mg every other week. Clinical remission was assessed at Week 8.
In study UC-II, 248 patients received 160 mg of Humira at Week 0, 80 mg at Week 2 and 40 mg eow thereafter, and 246 patients received placebo. Clinical results were assessed for induction of remission at Week 8 and for maintenance of remission at Week 52.
Subjects induced with 160/80 mg Humira achieved clinical remission versus placebo at Week 8 in statistically significantly greater percentages in study UC-I (18% vs. 9% respectively, p=0.031) and study UC-II (17% vs. 9% respectively, p=0.019). In study UC-II, among those treated with Humira who were in remission at Week 8, 21/41 (51%) were in remission at Week 52.
Results for both the overall UC-II study population and for patients who had responded at Week 8 of treatment per the full Mayo score are shown in Table 13. (See Table 13.)
Click on icon to see table/diagram/image
Approximately 40% of patients in study UC-II had failed prior anti-TNF treatment with infliximab. The efficacy of adalimumab in those patients was reduced compared to that in anti-TNF naïve patients. Among patients who had failed prior anti-TNF treatment, Week 52 remission was achieved by 3% on placebo and 10% on adalimumab.
The effectiveness of HUMIRA has not been established in patients who have lost response to or were intolerant to TNF blockers.
In the subgroup of patients in Study UC-II with prior TNF-blocker use, the treatment difference for induction of clinical remission appeared to be lower than that seen in the whole study population, and the treatment differences for sustained clinical remission and clinical remission at Week 52 appeared to be similar to those seen in the whole study population. The subgroup of patients with prior TNF-blocker use achieved induction of clinical remission at 9% (9/98) in the HUMIRA group versus 7% (7/101) in the placebo group, and sustained clinical remission at 5% (5/98) in the HUMIRA group versus 1% (1/101) in the placebo group. In the subgroup of patients with prior TNF-blocker use, 10% (10/98) were in clinical remission at Week 52 in the HUMIRA group versus 3% (3/101) in the placebo group.
Patients from UC studies I and II had the option to roll over into an open-label long-term extension study (UC-III). Following 3 years of HUMIRA therapy, 75% (301/402) continued to be in clinical remission per partial Mayo score, and of those who had received at least 4 years of HUMIRA therapy, 77% (245/320) were in clinical remission per partial Mayo score. Patients, who lost response after one year of treatment or beyond, could benefit from an increase of dosing frequency to 40 mg weekly.
Hospitalisation Rates: During 52 weeks of studies UC-I and UC-II, lower rates of all-cause hospitalisations and UC-related hospitalisations were observed for the adalimumab-treated arm compared to the placebo arm. The number of all cause hospitalisations in the adalimumab treatment group was 0.18 per patient year vs. 0.26 per patient year in the placebo group and the corresponding figures for UC-related hospitalisations were 0.12 per patient year vs. 0.22 per patient year.
Quality of Life: In UC Study II, improvement in the disease-specific inflammatory bowel disease questionnaire (IBDQ) total score was achieved at Week 52 in patients randomized to Humira 160/80 mg compared to placebo (p=0.007).
Plaque Psoriasis Clinical Studies: The safety and efficacy of Humira were assessed in over 1,600 patients 18 years of age or older with moderate to severe chronic plaque psoriasis who were candidates for systemic therapy or phototherapy in randomized, double-blind, well-controlled studies.
The safety and efficacy of Humira were also studied in adult patients with moderate to severe chronic plaque psoriasis with concomitant hand and/or foot psoriasis who were candidates for systemic therapy in a randomized double-blind study (Ps Study IV).
Ps Study I (M03-656, REVEAL) evaluated 1212 patients with chronic plaque psoriasis with ≥10% BSA involvement and Psoriasis Area and Severity Index (PASI) ≥12 within three treatment periods. In period A, patients received placebo or Humira subcutaneously at an initial dose of 80 mg at Week 0 followed by a dose of 40 mg every other week starting at Week 1. After 16 weeks of therapy, patients who achieved at least a PASI 75 response at Week 16, defined as a PASI score improvement of at least 75% relative to baseline, entered period B and received open label 40 mg Humira every other week. After 17 weeks of open label therapy, patients who maintained at least a PASI 75 response at Week 33 and were originally randomized to active therapy in Period A were re-randomized in period C to receive 40 mg Humira every other week or placebo for an additional 19 weeks. Across all treatment groups the mean baseline PASI score was 18.9 and the baseline Physician's Global Assessment (PGA) score ranged from "moderate" (52.6%) to "severe" (41.3%) to "very severe" (6.1%).
Ps Study II (M04-716, CHAMPION) compared the efficacy and safety of Humira versus methotrexate and placebo in 271 patients with 10% BSA involvement and PASI ≥10. Patients received placebo, an initial dose of MTX 7.5 mg and thereafter dose increases up to Week 12, with a maximum dose of 25 mg or an initial dose of 80 mg Humira followed by 40 mg every other week (starting one week after the initial dose) for 16 weeks. There are no data available comparing Humira and MTX beyond 16 weeks of therapy. Patients receiving MTX who achieved a ≥PASI 50 response at Week 8 and/or 12 did not receive further dose increases. Across all treatment groups, the mean baseline PASI score was 19.7 and the baseline PGA score ranged from "mild" (<1%) to "moderate" (48%) to "severe" (46%) to "very severe" (6%).
Ps Study III (M02-528) evaluated 148 patients with chronic plaque psoriasis with ≥5% BSA involvement for at least 1 year. Patients received placebo or Humira subcutaneously at a dose of 40 mg every other week starting at Week 1 after an initial dose of 80 mg at Week 0 or Humira at an initial dose of 80 mg at Week 0 followed by a dose of 40 mg weekly.
Patients participating in all Phase 2 and Phase 3 psoriasis studies were eligible to enroll into an open-label extension trial (M03-658), where Humira was given for at least an additional 108 weeks.
Clinical Results: In Ps Studies I, II and III, the primary endpoint was the proportion of patients who achieved a reduction in PASI score of at least 75% (PASI 75) from baseline at Week 16 for studies I and II and Week 12 for Study III. Other evaluated outcomes in Ps Studies I, II, and III included the PGA and other PASI measures. Ps Study I had an additional primary endpoint of loss of adequate response after Week 33 and on or before Week 52. Loss of adequate response is defined as a PASI score after Week 33 and on or before Week 52 that resulted in a <PASI 50 response relative to baseline with a minimum of a 6-point increase in PASI score relative to Week 33.
In Ps Studies I and II, more patients randomized to Humira than to placebo achieved at least a 75% reduction from baseline of PASI score at Week 16. Other relevant clinical parameters including PASI 100 (i.e. complete clearance of psoriasis skin signs) and PGA of "clear or minimal" were also improved over placebo. In Ps Study II, superior results were achieved for PASI 75, PASI 100 and PGA of "clear or minimal" in patients randomized to the Humira treatment group versus those randomized to receive methotrexate (see Tables 14 and 15).
Improvements in signs and symptoms in patients with moderate to severe psoriasis were maintained for up to 1 year (pivotal study M03-656) and for up to 3 years. (See Tables 14 and 15.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In Psoriasis Study I, 28% of patients who were PASI 75 responders and were re-randomized to placebo at week 33 compared to 5% continuing on Humira, p<0.001, experienced "loss of adequate response" (PASI score after week 33 and on or before week 52 that resulted in a <PASI 50 response relative to baseline with a minimum of a 6-point increase in PASI score relative to week 33). Of the patients who lost adequate response after re-randomization to placebo who then enrolled into the open-label extension trial, 38% (25/66) and 55% (36/66) regained PASI 75 response after 12 and 24 weeks of re-treatment, respectively.
A total of 233 PASI 75 responders at Week 16 and Week 33 received continuous Humira therapy for 52 weeks in Psoriasis Study I, and continued Humira in the open-label extension trial. PASI 75 and PGA of clear or minimal response rates in these patients were 74.7% and 59.0%, respectively, after an additional 108 weeks of open-label therapy (total of 160 weeks).
A total of 94 patients were randomized to Humira therapy in Psoriasis Study II, and continued Humira in the open label extension trial. PASI 75 and PGA clear or minimal response rates in these patients were 58.1% and 46.2%, respectively, after an additional 108 weeks of open-label therapy (total of 124 weeks).
A total of 347 stable responders participated in a withdrawal and retreatment evaluation in an open-label extension study. Median time to relapse (decline to PGA "moderate" or worse) was approximately 5 months. None of these patients experienced rebound during the withdrawal period. A total of 76.5% (218/285) of patients who entered the retreatment period had a response of PGA "clear" or "minimal" after 16 weeks of retreatment, irrespective of whether they relapsed during withdrawal (69.1% [123/178] and 88.8% [95/107] for patients who relapsed and who did not relapse during the withdrawal period, respectively).
Significant improvements at Week 16 from baseline compared to placebo (Studies I and II) and MTX (Study II) were demonstrated in the DLQI (Dermatology Life Quality Index). In Study I, improvements in the physical and mental component summary scores of the SF-36 were also significant compared to placebo.
In an open-label extension study, for patients whose dose escalated from 40 mg every other week to 40 mg weekly due to a PASI response below 50%, 26.4% (92/349) and 37.8% (132/349) of patients achieved PASI 75 response at Week 12 and 24, respectively.
Psoriasis Study III (REACH) compared the efficacy and safety of Humira versus placebo in 72 patients with moderate to severe chronic plaque psoriasis and hand and/or foot psoriasis. Patients received an initial dose of 80 mg Humira followed by 40 mg every other week (starting one week after the initial dose) or placebo for 16 weeks. At Week 16, a statistically significantly greater proportion of patients who received Humira achieved PGA of 'clear' or 'almost clear' for the hands and/or feet compared to patients who received placebo (30.6% versus 4.3%, respectively [P=0.014]).
Psoriasis Study IV compared the efficacy and safety of Humira versus placebo in 217 adult patients with moderate to severe nail psoriasis. Patients received an initial dose of 80 mg Humira followed by 40 mg every other week (starting one week after the initial dose) or placebo for 26 weeks followed by open-label Humira treatment for an additional 26 weeks. Nail psoriasis was assessed using the Modified Nail Psoriasis Severity Index (mNAPSI) and the Physician's Global Assessment of Fingernail Psoriasis (PGA-F). A statistically significantly higher proportion of patients randomized to Humira achieved at least a 75% improvement in mNAPSI (mNAPSI 75) at Week 26, as compared with patients randomized to placebo (see Table 16). The percent improvement in NAPSI was statistically significantly greater in Humira patients compared with placebo at Week 16 (44.2% vs 7.8%) and at Week 26 (56.2% vs 11.5%).
A statistically significant higher proportion of patients in the Humira group achieved a PGA-F of "clear" or "minimal" with at least a 2-grade improvement from Baseline at Week 26 compared with placebo. In this study, Humira demonstrated a treatment benefit in nail psoriasis patients with different extents of skin involvement (BSA ≥10% and BSA <10% and ≥5%) and a statistically significant improvement in scalp psoriasis compared with placebo. (See Table 16.)
Click on icon to see table/diagram/image
Of those who continued to receive Humira treatment until Week 52, 65.0% achieved mNAPSI 75 response and 61.3% achieved PGA-F response. Humira treated patients showed statistically significant improvements at Week 26 from baseline compared with placebo in the DLQI (Dermatology Life Quality Index). The mean decrease (improvement) from baseline at Week 26 was 8.0 in the Humira group (N=94) and 1.9 in the placebo group (N=93).
Results from Ps Study III supported the efficacy demonstrated in Ps Studies I and II: In Ps Study I, patients who were PASI 75 responders and were re-randomized to continue Humira therapy at Week 33 were less likely to experience a loss of adequate response on or before Week 52 than the PASI 75 responders who were re-randomized to placebo at Week 33 (4.9% versus 28.4%, p<0.001).
Quality of Life: Patient Reported Outcomes (PRO) were evaluated by several measures. Quality of Life was assessed using the disease-specific Dermatology Life Quality Index (DLQI) in Ps Study I and Ps Study II. In Ps Study I, patients receiving Humira demonstrated clinically meaningful improvement in the DLQI total score, disease severity, pain, and pruritus compared to the placebo group at both Weeks 4 & 16. The DLQI result was maintained at Week 52. In Ps Study II, patients receiving Humira demonstrated clinically meaningful improvement in the DLQI total score, disease severity, and pruritus compared to the placebo and methotrexate groups at Week 16, and clinically meaningful improvement in pain compared to the placebo group at Week 16.
The Short Form Health Survey (SF-36) was used to assess general health-related quality of life in Ps Study I. The Humira-treated patients had significantly greater improvement in the SF-36 Physical Component Summary (PCS) and Mental Component Summary (MCS) scores.
Hidradenitis Suppurativa Clinical Studies: The safety and efficacy of Humira were assessed in randomized, double-blind, placebo-controlled studies and an open-label extension study in adult patients with moderate to severe hidradenitis suppurativa (HS) who were intolerant, had a contraindication or an inadequate response to systemic antibiotic therapy. The patients in Studies HS-I and HS-II had Hurley Stage II or III disease with at least 3 abscesses or inflammatory nodules.
Study HS-I (M11-313) evaluated 307 patients with 2 treatment periods. In Period A, patients received placebo or HUMIRA at an initial dose of 160 mg at Week 0, 80 mg at Week 2, and 40 mg every week starting at Week 4 to Week 11. Concomitant antibiotic use was not allowed during the study. After 12 weeks of therapy, patients who had received HUMIRA in Period A were re-randomized in Period B to 1 of 3 treatment groups (HUMIRA 40 mg every week, HUMIRA 40 mg every other week, or placebo from Week 12 to Week 35). Patients who had been randomized to placebo in Period A were assigned to receive Humira 40 mg every week in Period B.
Study HS-II (M11-810) evaluated 326 patients with 2 treatment periods. In Period A, patients received placebo or HUMIRA at an initial dose of 160 mg at Week 0 and 80 mg at Week 2 and 40 mg every week starting at Week 4 to Week 11. 19.3% of patients had continued baseline oral antibiotic therapy during the study. After 12 weeks of therapy, patients who had received HUMIRA in Period A were re-randomized in Period B to 1 of 3 treatment groups (HUMIRA 40 mg every week, HUMIRA 40 mg every other week, or placebo from Week 12 to Week 35). Patients who had been randomized to placebo in Period A were assigned to receive placebo in Period B.
Patients participating in Studies HS-I and HS-II were eligible to enroll into an open-label extension study in which Humira 40mg was administered every week. Mean exposure in all adalimumab population was 762 days. Throughout all 3 studies patients used topical antiseptic wash daily.
Clinical Response: Reduction of inflammatory lesions and prevention of worsening of abscesses and draining fistulas was assessed using Hidradenitis Suppurativa Clinical Response (HiSCR; at least a 50% reduction in total abscess and inflammatory nodule count with no increase in abscess count and no increase in draining fistula count relative to Baseline). Reduction in HS-related skin pain was assessed using a Numeric Rating Scale in patients who entered the study with an initial baseline score of 3 or greater on a 11 point scale.
At Week 12, a significantly higher proportion of patients treated with Humira versus placebo achieved HiSCR. At Week 12, a significantly higher proportion of patients in Study HS-II experienced a clinically relevant decrease in HS-related skin pain (see Table 17). Patients treated with Humira had significantly reduced risk of disease flare during the initial 12 weeks of treatment. (See Table 17.)
Click on icon to see table/diagram/image
Among patients who were randomized to Humira continuous weekly dosing, the overall HiSCR rate at Week 12 was maintained through Week 96. Longer term treatment with Humira 40 mg weekly for 96 weeks identified no new safety findings.
Greater improvements at Week 12 from baseline compared to placebo were demonstrated in skin-specific health-related quality of life, as measured by the Dermatology Life Quality Index (DLQI; Studies HS-I and HS-II), patient global satisfaction with medication treatment as measured by the Treatment Satisfaction Questionnaire - medication (TSQM; Studies HS-I and HS-II) and physical health as measured by the physical component summary score of the SF-36 (Study HS-I).
Uveitis Clinical Studies: The safety and efficacy of Humira were assessed in adult patients with non-infectious intermediate, posterior, and panuveitis (also known as "non-infectious uveitis affecting the posterior segment"), excluding patients with isolated anterior uveitis, in two randomized, double-masked, placebo-controlled studies (UV Study I (M10-877) and UV Study II (M10-880)). Patients received placebo or Humira at an initial dose of 80 mg followed by 40 mg every other week starting one week after the initial dose. Concomitant stable doses of non-biologic immunosuppressants were permitted. The primary efficacy endpoint in both studies was 'time to treatment failure'. Following initial control of disease, a prolongation in time to treatment failure will result in reduced risk of disease flares, inflammation and vision loss.
Treatment failure was defined by a multi-component outcome based on inflammatory chorioretinal and/or inflammatory retinal vascular lesions, anterior chamber (AC) cell grade, vitreous haze (VH) grade and best corrected visual acuity (BCVA).
UV Study I evaluated 217 patients with active uveitis despite treatment with corticosteroids (oral prednisone at a dose of 10 to 60 mg/day). All patients received a standardized dose of prednisone 60 mg/day at study entry followed by a mandatory taper schedule, with complete corticosteroid discontinuation by Week 15.
UV Study II evaluated 226 patients with inactive uveitis requiring chronic corticosteroid treatment (oral prednisone 10 to 35 mg/day) at baseline to control their disease. Patients subsequently underwent a mandatory taper schedule, with complete corticosteroid discontinuation by Week 19.
Clinical Response: Results from both studies demonstrated statistically significant reduction of the risk of treatment failure in patients treated with HUMIRA versus patients receiving placebo (See Table 18). Both studies demonstrated an early and sustained effect of HUMIRA on the treatment failure rate versus placebo (see Figure 5). (See Figure 5 and Tables 18 and 19).
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Additionally, in UV Study I, statistically significant differences in favor of adalimumab versus placebo were observed for changes in AC cell grade, vitreous haze grade, and logMAR BCVA (mean change from best state prior to Week 6 to the final visit; P Values: 0.011, <0.001 and 0.003, respectively).
Of the 417 subjects included in the uncontrolled long-term extension of Studies UV I and UV II, 46 subjects were regarded ineligible (e.g. developed complications secondary to diabetic retinopathy, due to cataract surgery or vitrectomy) and were excluded from the primary analysis of efficacy. Of the 371 remaining patients, 276 evaluable patients reached 78 weeks of open-label adalimumab treatment. Based on the observed data approach, 222 (80.4%) were in quiescence (no active inflammatory lesions, AC cell grade ≤0.5+, VH grade ≤0.5+) with a concomitant steroid dose ≤7.5 mg per day, and 184 (66.7 %) were in steroid-free quiescence. BCVA was either improved or maintained (<5 letters deterioration) in 88.4% of the eyes at week 78. Among the patients who discontinued the study prior to week 78, 11% discontinued due to adverse events, and 5% due to insufficient response to adalimumab treatment.
Quality of Life: In UV Study 1, treatment with Humira resulted in maintenance of vision-related functioning and health-related quality of life, as measured by the NEI VFQ-25.
Pediatrics: Juvenile Idiopathic Arthritis Clinical Studies: Polyarticular Juvenile Idiopathic Arthritis (pJIA): The safety and efficacy of Humira was assessed in two studies (pJIA I and II) in children with active polyarticular or polyarticular course juvenile idiopathic arthritis, who had a variety of JIA onset types (most frequently rheumatoid-factor negative or positive polyarthritis and extended oligoarthritis).
pJIA I: The safety and efficacy of Humira were assessed in a multicenter, randomized, double-blind, parallel-group study in 171 children (4 to 17 years old) with polyarticular juvenile idiopathic arthritis (JIA). In the open-label lead in phase (OL LI), patients were stratified into two groups, MTX (methotrexate)-treated or non-MTX-treated. Patients who were in the non-MTX stratum were either naïve or had been withdrawn from MTX at least two weeks prior to study drug administration. Patients remained on stable doses of NSAIDs and or prednisone (≤0.2 mg/kg/day or 10 mg/day maximum). In the OL LI phase, all patients received 24 mg/m
2 up to a maximum of 40 mg of Humira every other week for 16 weeks. The distribution of patients by age and minimum, median and maximum dose received during the OL LI phase is presented in Table 20. (See Table 20.)
Click on icon to see table/diagram/image
Patients demonstrating a Pediatric ACR 30 response at week 16 were eligible to be randomized into the double blind (DB) phase and received either Humira 24 mg/m
2 up to a maximum of 40 mg, or placebo every other week for an additional 32 weeks or until disease flare. Disease flare criteria was defined as a worsening of ≥30% from baseline in ≥3 of 6 Pediatric ACR core criteria, ≥2 active joints, and improvement of >30% in no more than 1 of the 6 criteria. After 32 weeks or at disease flare, patients were eligible to enroll into the open label extension phase. (See Table 21.)
Click on icon to see table/diagram/image
Among those who responded at week 16 (n=144), the Pediatric ACR 30/50/90 responses were maintained for up to two years in the OLE phase in patients who received Humira throughout the study.
Overall responses were generally better and fewer patients developed antibodies when treated with the combination of Humira and MTX compared to Humira alone. Taking these results into consideration, Humira is recommended for use in combination with MTX and for use as monotherapy in patients for who MTX use is not appropriate.
pJIA II: The safety and efficacy of Humira was assessed in an open-label, multicenter study in 32 children (2 to <4 years old or aged 4 and above weighing <15 kg) with moderately to severely active polyarticular JIA. The patients received 24 mg/m
2 body surface area (BSA) of Humira up to a maximum of 20 mg every other week as a single dose via SC injection for at least 24 weeks. During the study, most subjects used concomitant MTX, with fewer reporting use of corticosteroids or NSAIDs.
At Week 12 and Week 24, Pediatric ACR 30 response was 93.5% and 90.0%, respectively, using the observed data approach. The proportions of subjects with Pediatric ACR 50/70/90 at Week 12 and Week 24 were 90.3%/61.3%/38.7% and 83.3%/73.3%/36.7%, respectively. Amongst those who responded (Pediatric ACR 30) at Week 24 (n=27 out of 30 patients), the Pediatric ACR 30 responses were maintained for up to 60 weeks in the OLE phase in patients who received Humira throughout this time period. Overall, 20 subjects were treated for 60 weeks or longer.
Enthesitis-Related Arthritis: The safety and efficacy of Humira were assessed in a multicenter, randomized, double-blind study in 46 pediatric patients (6 to 17 years old) with enthesitis-related arthritis. Patients were randomized to receive either 24 mg/m
2 body surface area (BSA) of Humira up to a maximum of 40 mg, or placebo every other week for 12 weeks. The double-blind period is followed by an open-label (OL) period during which patients received 24 mg/m
2 BSA of Humira up to a maximum of 40 mg every other week subcutaneously for up to an additional 192 weeks. The primary endpoint was the percent change from Baseline to Week 12 in the number of active joints with arthritis (swelling not due to deformity or joints with loss of motion plus pain and/or tenderness), which was achieved (p=0.039) with mean percent decrease of -62.6% in patients in the Humira group compared to -11.6% in patients in the placebo group. Improvement in number of active joints with arthritis was maintained during the open label period through Week 156. The majority of patients demonstrated clinical improvement in secondary endpoints such as number of sites of enthesitis, tender joint count (TJC), swollen joint count (SJC), Pediatric ACR 30 response, Pediatric ACR 50 response, and Pediatric ACR 70 response and maintained these improvements during the open label period through Week 156 of the study.
Pediatric Crohn's Disease Clinical Study: Humira was assessed in a multicenter, randomized, double-blind clinical trial designed to evaluate the efficacy and safety of induction and maintenance treatment with doses dependent on body weight (<40 kg or ≥40 kg) in 192 pediatric subjects between the ages of 6 and 17 (inclusive) years, with moderate to severe Crohn's disease (CD) defined as Pediatric Crohn's Disease Activity Index (PCDAI) score >30. Subjects had to have failed conventional therapy (including a corticosteroid and/or an immunomodulator) for CD. Subjects may also have previously lost response or been intolerant to infliximab.
All subjects received open-label induction therapy at a dose based on their Baseline body weight: 160 mg at Week 0 and 80 mg at Week 2 for subjects ≥40 kg, and 80 mg and 40 mg, respectively, for subjects <40 kg.
At Week 4, subjects were randomized 1:1 based on their body weight at the time to either the Low Dose or Standard Dose maintenance regimens as shown in Table 22. (See Table 22.)
Click on icon to see table/diagram/image
Efficacy Results: The primary endpoint of the study was clinical remission at Week 26, defined as PCDAI score ≤10.
Clinical remission and clinical response (defined as reduction in PCDAI score of at least 15 points from Baseline) rates are presented in Table 23. Rates of discontinuation of corticosteroids or immunomodulators are presented in Table 24. (See Tables 23 and 24.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Statistically significant increases (improvement) from Baseline to Week 26 and 52 in Body Mass Index and height velocity were observed for both treatment groups. Statistically and clinically significant improvements from Baseline were also observed in both treatment groups for quality of life parameters (including IMPACT III).
Pediatric Plaque Psoriasis Clinical Study: The efficacy of Humira was assessed in a randomized, double-blind, controlled study of 114 pediatric patients from 4 years of age with severe chronic plaque psoriasis (as defined by a PGA ≥4 or >20% BSA involvement or >10% BSA involvement with very thick lesions or PASI ≥20 or ≥10 with clinically relevant facial, genital, or hand/foot involvement) who were inadequately controlled with topical therapy and heliotherapy or phototherapy.
Patients received Humira 0.8mg/kg eow (up to 40 mg), 0.4 mg/kg eow (up to 20 mg), or methotrexate 0.1-0.4 mg/kg weekly (up to 25 mg). At week 16, more patients randomized to Humira 0.8 mg/kg had positive efficacy responses (e.g., PASI 75) than those randomized to MTX. (See Table 25.)
Click on icon to see table/diagram/image
Patients who achieved PASI 75 and PGA clear or minimal were withdrawn from treatment for up to 36 weeks and monitored for loss of disease control (loss of PGA response). Patients were then re-treated with adalimumab 0.8 mg/kg eow for an additional 16 weeks and responses observed during retreatment were similar to the previous double-blind period: PASI 75 response of 78.9% (15 of 19 subjects) and PGA clear or minimal of 52.6% (10 of 19 subjects).
In the open label period of the study, PASI 75 and PGA clear or minimal responses were maintained for up to an additional 52 weeks with no new safety findings.
Adolescent Hidradenitis Suppurativa: There are no clinical trials with Humira in adolescent patients with hidradenitis suppurativa (HS). Efficacy of Humira for the treatment of adolescent patients with HS is predicted based on the demonstrated efficacy and exposure-response relationship in adult HS patients and the likelihood that the disease course, pathophysiology, and drug effects are substantially similar to that of adults at the same exposure levels. The recommended adolescent HS dosing schedule of 40 mg every other week is predicted to provide similar efficacy to that observed in adult HS patients receiving the recommended adult dose of 40 mg every week. Safety of the recommended Humira dose in the adolescent HS population is based on cross-indication safety profile of Humira in both adults and pediatric patients at similar or more frequent doses.
Pediatric Uveitis Clinical Study: The safety and efficacy of Humira was assessed in a randomized, double-masked, controlled study of 90 pediatric patients from 2 to <18 years of age with active JIA-associated noninfectious anterior uveitis who were refractory to at least 12 weeks of methotrexate treatment. Patients received either placebo or 20 mg adalimumab (if <30 kg) or 40 mg adalimumab (if ≥30 kg) every other week in combination with their baseline dose of methotrexate.
The primary endpoint was 'time to treatment failure.' The criteria determining treatment failure were worsening, or sustained non-improvement in ocular inflammation, or partial improvement with development of sustained ocular co-morbidities, or worsening of ocular co-morbidities, non-permitted use of concomitant medications, and suspension of treatment for an extended period of time.
Clinical Response: Adalimumab significantly delayed the time to treatment failure, as compared to placebo (See Figure 6, P <0.0001 from log rank test). The median time to treatment failure was 24.1 weeks for subjects treated with placebo, whereas the median time to treatment failure was not estimable for subjects treated with adalimumab because less than one-half of these subjects experienced treatment failure. Adalimumab significantly decreased the risk of treatment failure by 75% relative to placebo, as shown by the hazard ratio (HR=0.25 [95% CI: 0.12, 0.49]). (See Figure 6.)
Click on icon to see table/diagram/image
Pediatric Ulcerative Colitis: The safety and efficacy of Humira was assessed in a multicenter, randomized, double-blind, trial in 93 pediatric patients from 5 to 17 years of age with moderate to severe ulcerative colitis (Mayo score 6 to 12 with endoscopy subscore of 2 to 3 points, confirmed by centrally read endoscopy) who had an inadequate response or intolerance to conventional therapy. Approximately 16% of patients in the study had failed prior anti-TNF treatment. Patients who received corticosteroids at enrollment were allowed to taper their corticosteroid therapy after Week 4.
In the induction period of the study, 77 patients were randomized 3:2 to receive double-blind treatment with adalimumab at an induction dose of 2.4 mg/kg (maximum of 160 mg) at Week 0 and Week 1, and 1.2 mg/kg (maximum of 80 mg) at Week 2; or an induction dose of 2.4 mg/kg (maximum of 160 mg) at Week 0, placebo at Week 1, and 1.2 mg/kg (maximum of 80 mg) at Week 2. Both groups received 0.6 mg/kg (maximum of 40 mg) at Week 4 and Week 6. Following an amendment to the study design, the remaining 16 patients who enrolled in the induction period received open-label treatment with adalimumab at the induction dose of 2.4 mg/kg (maximum of 160 mg) at Week 0 and Week 1, and 1.2 mg/kg (maximum of 80 mg) at Week 2.
At Week 8, 62 patients who demonstrated clinical response per Partial Mayo Score (PMS; defined as a decrease in PMS ≥2 points and ≥30% from Baseline) were randomized equally to receive double-blind maintenance treatment at a dose of 0.6 mg/kg (maximum of 40 mg) every week (ew), or a maintenance dose of 0.6 mg/kg (maximum of 40 mg) every other week (eow). Prior to an amendment to the study design, 12 additional patients who demonstrated clinical response per PMS were randomized to receive placebo but were not included in the confirmatory analysis of efficacy.
Disease flare was defined as an increase in Partial Mayo Score (PMS) of at least 3 points (for patients with PMS of 0 to 2 at Week 8), at least 2 points (for patients with PMS of 3 to 4 at Week 8), or at least 1 point (for patients with PMS of 5 to 6 at Week 8).
Patients who met criteria for disease flare at or after Week 12 were randomized to receive a re-induction dose of 2.4 mg/kg (maximum of 160 mg) or a dose of 0.6 mg/kg (maximum of 40 mg) and continued to receive their respective maintenance dose regimen afterwards.
Efficacy Results: The co-primary endpoints of the study were clinical remission per PMS (defined as PMS ≤2 and no individual subscore >1) at Week 8, and clinical remission per FMS (Full Mayo Score) (defined as a Mayo Score ≤2 and no individual subscore >1) at Week 52 in patients who achieved clinical response per PMS at Week 8. Clinical remission rates per PMS at Week 8 for patients in each of the Humira double-blind induction groups are presented in Table 26. (See Table 26.)
Click on icon to see table/diagram/image
At Week 52, clinical remission per FMS in Week 8 responders, clinical response per FMS (defined as a decrease in Mayo Score ≥3 points and ≥30% from Baseline) in Week 8 responders, mucosal healing (defined as Mayo endoscopy subscore ≤1) in Week 8 responders, clinical remission per FMS in Week 8 remitters, and the proportion of subjects in corticosteroid-free remission per FMS in Week 8 responders were assessed in patients who received Humira at the double-blind maximum 40 mg eow (0.6 mg/kg) and maximum 40 mg ew (0.6 mg/kg) maintenance doses (Table 27). (See Table 27.)
Click on icon to see table/diagram/image
Additional exploratory efficacy endpoints included clinical response per the Pediatric Ulcerative Colitis Activity Index (PUCAI) (defined as a decrease in PUCAI ≥20 points from Baseline) and clinical remission per PUCAI (defined as PUCAI <10) at Week 8 and Week 52 (Table 28). (See Table 28.)
Click on icon to see table/diagram/image
Of the adalimumab-treated patients who received re-induction treatment during the maintenance period, 2/6 (33%) achieved clinical response per FMS at Week 52.
Quality of Life: Improvements from Baseline were observed in IMPACT III and the caregiver Work Productivity and Activity Impairment (WPAI) scores for the groups treated with adalimumab.
Increases (improvement) from Baseline in height velocity were observed for the groups treated with adalimumab, and increases (improvement) from Baseline in Body Mass Index were observed for subjects on the Humira maintenance dose of maximum 40 mg (0.6 mg/kg) ew.
Immunogenicity: Formation of anti-adalimumab antibodies is associated with increased clearance and reduced efficacy of adalimumab. There is no apparent correlation between the presence of anti-adalimumab antibodies and adverse events.
Because immunogenicity analyses are product-specific, comparison of antibody rates with those from other products is not appropriate.
Adults: Patients in rheumatoid arthritis studies I, II and III were tested at multiple time points for anti-adalimumab antibodies during the 6 to 12 month period. In the pivotal trials, anti-adalimumab antibodies were identified in 5.5% (58/1053) of patients treated with adalimumab, compared to 0.5% (2/370) on placebo. In patients not given concomitant methotrexate, the incidence was 12.4%, compared to 0.6% when adalimumab was used as add-on to methotrexate.
In patients with psoriatic arthritis, anti-adalimumab antibodies were identified in 10% (38/376) of patients treated with adalimumab. In patients not given concomitant methotrexate, the incidence was 13.5% (24/178), compared to 7% (14/198) when adalimumab was used as add-on to methotrexate.
In patients with ankylosing spondylitis anti-adalimumab antibodies were identified in 8.3% (17/204) of patients treated with adalimumab. In patients not given concomitant methotrexate, the incidence was 8.6% (16/185), compared to 5.3% (1/19) when adalimumab was used as add-on to methotrexate.
In patients with Crohn's disease, anti-adalimumab antibodies were identified in 2.6% (7/269) of patients treated with adalimumab.
In patients with moderately to severely active ulcerative colitis, the rate of anti-adalimumab antibody development in patients treated with adalimumab was 5.0%. In patients with psoriasis, anti-adalimumab antibodies were identified in 8.4% (77/920) of patients treated with adalimumab without concomitant methotrexate.
In plaque psoriasis patients on long term adalimumab without concomitant methotrexate who participated in a withdrawal and retreatment study, the rate of anti-adalimumab antibodies after retreatment was 2.3%, and was similar to the rate observed prior to withdrawal 1.9%.
In patients with moderate to severe hidradenitis suppurativa, anti-adalimumab antibodies were identified in 10.1% (10/99) of patients treated with adalimumab.
In patients with non-infectious uveitis, anti-adalimumab antibodies were identified in 4.8% (12/249) of patients treated with adalimumab.
Pediatrics: In patients with polyarticular juvenile idiopathic arthritis who were 4 to 17 years, anti-adalimumab antibodies were identified in 16.0% (27/171) of patients treated with adalimumab. In patients not given concomitant methotrexate, the incidence was 26.0% (22/86), compared to 6.0% (5/85) when adalimumab was used as add-on to methotrexate. In patients with polyarticular juvenile idiopathic arthritis who were 2 to <4 years old or aged 4 and above weighing <15 kg, anti-adalimumab antibodies were identified in 7.0% (1/15) of patients, and the one patient was receiving concomitant methotrexate.
In patients with enthesitis-related arthritis, anti-adalimumab antibodies were identified in 11% (5/46) of patients treated with adalimumab. In patients not given concomitant methotrexate, the incidence was 14% (3/22), compared to 8% (2/24) when adalimumab was used as add-on to methotrexate.
In patients with moderately to severely active pediatrics Crohn's disease, the rate of anti-adalimumab antibody development in patients receiving adalimumab was 3.3% (6/182).
In patients with pediatric psoriasis, anti-adalimumab antibodies were identified in 13% (5/38) of subjects treated with 0.8 mg/kg adalimumab monotherapy.
In patients with moderately to severely active pediatric ulcerative colitis, the rate of anti-adalimumab antibody development in patients receiving adalimumab was 3%.
Pharmacokinetics: Absorption: Following a single 40 mg subcutaneous (SC) administration of adalimumab to 59 healthy adult subjects, absorption and distribution of adalimumab was slow, with mean peak serum concentration being reached about five days after administration. The average absolute bioavailability of adalimumab estimated from three studies following a single 40 mg subcutaneous dose was 64%.
Distribution and Elimination: The single dose pharmacokinetics of adalimumab were determined in several studies with intravenous doses ranging from 0.25 to 10 mg/kg. The distribution volume (V
ss) ranged from 4.7 to 6.0 L, indicating that adalimumab distributes approximately equally between the vascular and extravascular fluids. Adalimumab is slowly eliminated, with clearances typically under 12 mL/h. The mean terminal phase half-life was approximately two weeks, ranging from 10 to 20 days across studies. The clearance and half-life were relatively unchanged over the studied dose range, and the terminal half-life was similar after IV and SC administration. Adalimumab concentrations in the synovial fluid from several RA patients ranged from 31 to 96% of those in serum.
Steady-state pharmacokinetics: Accumulation of adalimumab was predictable based on the half-life following SC administration of 40 mg of adalimumab every other week to patients with RA, with mean steady-state trough concentrations of approximately 5 mcg/mL (without concomitant methotrexate (MTX) and 8 to 9 mcg/mL (with concomitant MTX)), respectively. The serum adalimumab trough levels at steady state increased approximately proportionally with dose following 20, 40 and 80 mg every other week and every week SC dosing. In long-term studies with dosing more than two years, there was no evidence of changes in clearance over time.
In patients with psoriasis, the mean steady-state trough concentration was 5 mcg/mL during adalimumab 40 mg eow without concomitant MTX treatment.
In patients with hidradenitis suppurativa, a dose of 160 mg adalimumab on Week 0 followed by 80 mg on Week 2 achieved serum adalimumab trough concentrations of approximately 7 to 8 mcg/mL at Week 2 and Week 4. The mean steady-state trough concentration at Week 12 through Week 36 were approximately 8 to 10 mcg/mL during adalimumab 40 mg every week treatment.
In patients with uveitis, a loading dose of 80 mg adalimumab on Week 0 followed by 40 mg adalimumab every other week starting at Week 1, resulted in mean steady-state concentrations of approximately 8 to 10 mcg/mL.
Population pharmacokinetic and pharmacokinetic/pharmacodynamic modelling and simulation predicted comparable adalimumab exposure and efficacy in patients treated with 80 mg every other week when compared with 40 mg every week (including adult patients with RA, HS, UC, CD or Ps, adolescent patients with HS, and pediatric patients ≥40 kg with CD and UC).
Population pharmacokinetic analyses with data from over 1200 patients revealed that co-administration of MTX had an intrinsic effect on adalimumab apparent clearance (CL/F) (see Interactions). As expected, there was a trend toward higher apparent clearance of adalimumab with increasing body weight and in the presence of anti-adalimumab antibodies.
Other more minor factors were also identified; higher apparent clearance was predicted in patients receiving doses lower than the recommended dose, and in patients with high rheumatoid factor or CRP concentrations. These factors are not likely to be clinically important.
In patients with Crohn's disease, the loading dose of 80 mg adalimumab on Week 0 followed by 40 mg Humira on Week 2 achieves serum adalimumab trough levels of approximately 5.5 mcg/mL during the induction period. A loading dose of 160 mg adalimumab on Week 0 followed by 80 mg Humira on Week 2 achieves serum adalimumab trough levels of approximately 12 mcg/mL during the induction period. Mean steady-state trough levels of approximately 7 mcg/mL were observed at Week 24 and Week 56 in Crohn's disease patients after receiving a maintenance dose of 40 mg adalimumab every other week.
In patients with ulcerative colitis, a loading dose of 160 mg adalimumab on Week 0 followed by 80 mg adalimumab on Week 2 achieves serum adalimumab trough concentrations of approximately 12 mcg/mL during the induction period. Mean steady-state trough levels of approximately 8 mcg/mL were observed in ulcerative colitis patients who received a maintenance dose of 40 mg adalimumab every other week.
Special Populations: Pharmacokinetics in special populations were investigated using population pharmacokinetic analyses.
Geriatrics: Age appeared to have a minimal effect on adalimumab apparent clearance. From the population analyses, the mean weight-adjusted clearances in patients 40 to 65 years (n=850) and ≥65 years (n=287) were 0.33 and 0.30 mL/h/kg, respectively.
Pediatrics: Following the administration of 24 mg/m
2 (up to a maximum of 40 mg) subcutaneously every other week to patients with polyarticular juvenile idiopathic arthritis (JIA) who were 4 to 17 years, the mean trough steady-state (values measured from Week 20 to 48) serum adalimumab concentration was 5.6 ± 5.6 μg/mL (102% CV) for adalimumab without concomitant MTX and 10.9 ± 5.2 μg/mL (47.7% CV) with concomitant MTX. The mean steady-state trough serum adalimumab concentrations for patients weighing <30 kg receiving 20 mg adalimumab subcutaneously every other week without concomitant MTX or with concomitant MTX were 6.8 μg/mL and 10.9 μg/mL, respectively. The mean steady-state trough serum adalimumab concentrations for patients weighing ≥30 kg receiving 40 mg adalimumab subcutaneously every other week without concomitant MTX or with concomitant MTX were 6.6 μg/mL and 8.1 μg/mL, respectively. In patients with polyarticular JIA who were 2 to <4 years old or aged 4 and above weighing <15 kg dosed with adalimumab 24 mg/m
2, the mean trough steady-state serum adalimumab concentrations was 6.0 ± 6.1 μg/mL (101% CV) for adalimumab without concomitant MTX and 7.9 ± 5.6 μg/mL (71.2% CV) with concomitant MTX.
Following the administration of 24 mg/m
2 (up to a maximum of 40 mg) subcutaneously every other week to patients with enthesitis-related arthritis, the mean trough steady-state (values measured at Week 24) serum adalimumab concentrations were 8.8 ± 6.6 μg/mL for adalimumab without concomitant methotrexate and 11.8 ± 4.3 μg/mL with concomitant methotrexate.
In pediatric patients with moderately to severely active Crohn's disease, the open-label adalimumab induction dose was 160/80 mg or 80/40 mg at Weeks 0 and 2, respectively, dependent on a body weight cut-off of 40 kg. At Week 4, patients were randomized 1:1 to either the Standard Dose (40/20 mg eow) or Low Dose (20/10 mg eow) maintenance treatment groups based on their body weight. The mean (±SD) serum adalimumab trough concentrations achieved at Week 4 were 15.7±6.6 μg/mL for patients ≥40 kg (160/80 mg) and 10.6±6.1 μg/mL for patients <40 kg (80/40 mg).
For patients who stayed on their randomized therapy, the mean (±SD) adalimumab trough concentrations at Week 52 were 9.5±5.6 μg/mL for the Standard Dose group and 3.5±2.2 μg/mL for the Low Dose group. The mean trough concentrations were maintained in patients who continued to receive adalimumab treatment eow for 52 weeks. For patients who dose escalated from eow to weekly regimen, the mean (±SD) serum concentrations of adalimumab at Week 52 were 15.3±11.4 μg/mL (40/20 mg, weekly) and 6.7±3.5 μg/mL (20/10 mg, weekly).
Following the administration of 0.8 mg/kg (up to a maximum of 40 mg) subcutaneously every other week to pediatric patients with chronic plaque psoriasis, the mean ± SD steady-state adalimumab trough concentration was approximately 7.4 ± 5.8 μg/mL (79% CV).
Adalimumab exposure in adolescent hidradenitis suppurativa (HS) patients was predicted using population pharmacokinetic modeling and simulation based on cross-indication pharmacokinetics in other pediatric patients (pediatric psoriasis, juvenile idiopathic arthritis, pediatric Crohn's disease, and enthesitis-related arthritis). The recommended adolescent HS dosing schedule of 40 mg every other week is predicted to provide serum adalimumab exposure similar to that observed in adult HS patients receiving the recommended adult dose of 40 mg every week.
Adalimumab exposure in paediatric uveitis patients was predicted using population pharmacokinetic modelling and simulation based on cross-indication pharmacokinetics in other paediatric patients (paediatric psoriasis, juvenile idiopathic arthritis, paediatric Crohn's disease, and enthesitis-related arthritis). No clinical exposure data are available on the use of a loading dose in children <6 years. The predicted exposures indicate that in the absence of methotrexate, a loading dose may lead to an initial increase in systemic exposure.
Following the subcutaneous administration of body weight-based dosing of 0.6 mg/kg (maximum of 40 mg) every other week to pediatric patients with ulcerative colitis, the mean trough steady-state serum adalimumab concentration was 5.01±3.28 μg/mL at Week 52. For patients who received 0.6 mg/kg (maximum of 40 mg) every week, the mean (±SD) trough steady-state serum adalimumab concentration was 15.7±5.60 μg/mL at Week 52.
Gender: No gender-related pharmacokinetic differences were observed after correction for a patient's body weight.
Race: No differences in immunoglobulin clearance would be expected among races. From limited data in non-Caucasians, no important kinetic differences were observed for adalimumab.
Hepatic and Renal Insufficiency: No pharmacokinetic data are available in patients with hepatic or renal impairment.
Disease States: Healthy volunteers and patients with RA displayed similar adalimumab pharmacokinetics.
Toxicology: Pre-Clinical Safety Data: Preclinical data reveal no special hazard for humans based on studies of single dose toxicity, repeated dose toxicity, and genotoxicity.
Carcinogenesis, Mutagenesis, and Impairment of Fertility: Long-term animal studies of adalimumab have not been conducted to evaluate the carcinogenic potential or its effect on fertility.
No clastogenic or mutagenic effects of adalimumab were observed in the
in vivo mouse micronucleus test or the
Salmonella-
Escherichia coli (Ames) assay, respectively.



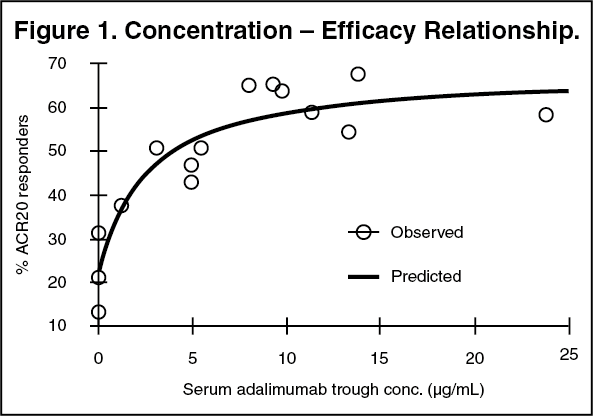 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image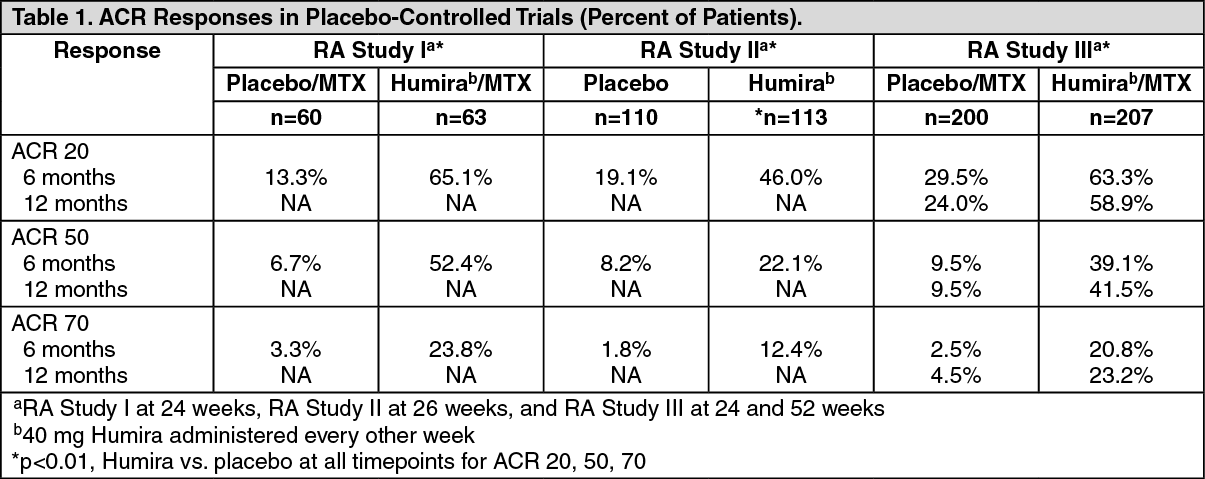 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image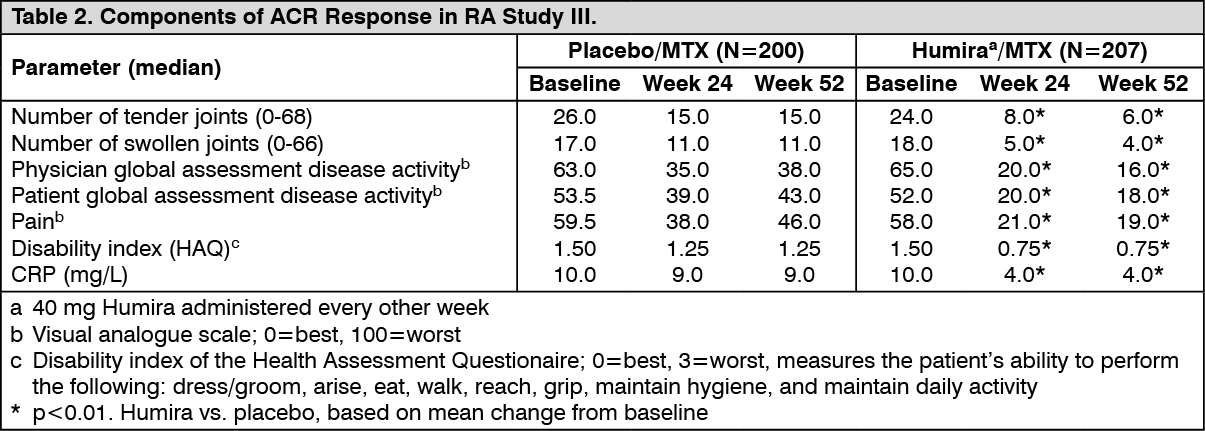 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image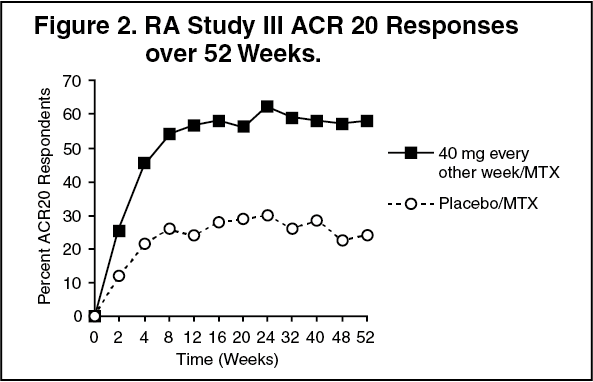 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image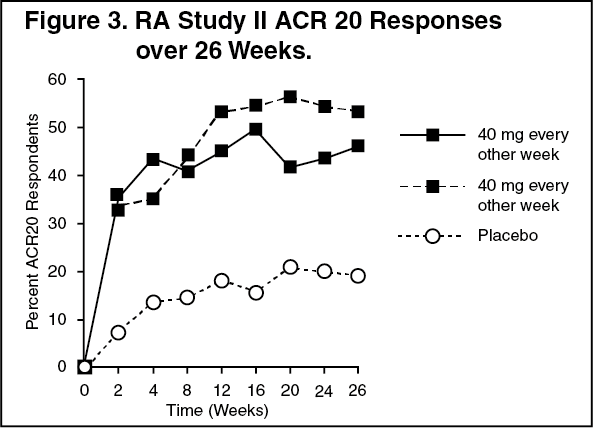 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image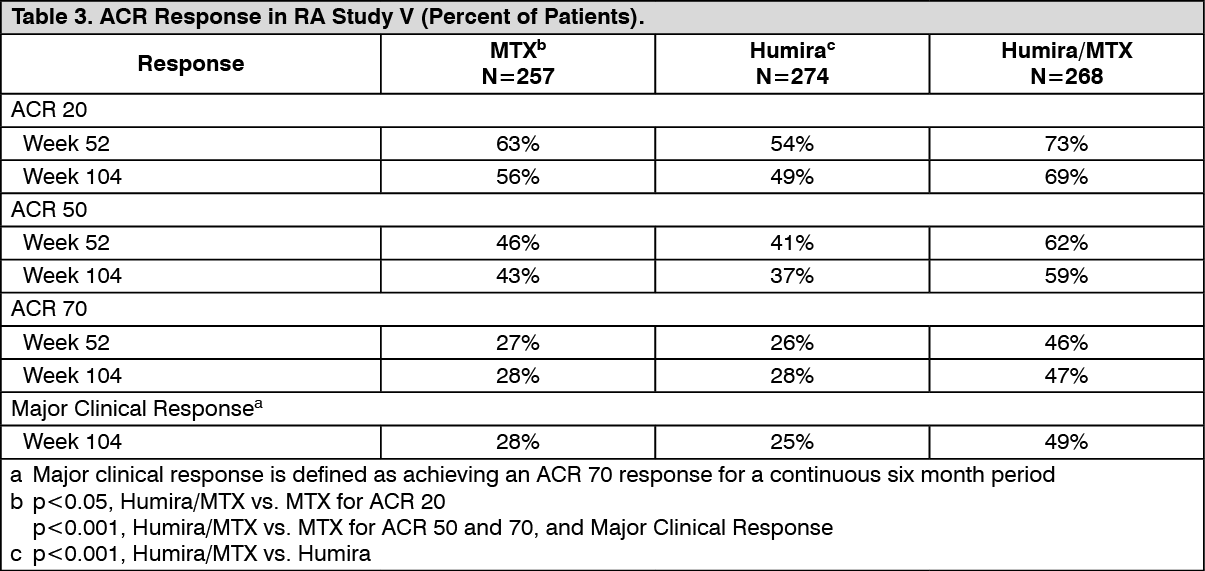 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image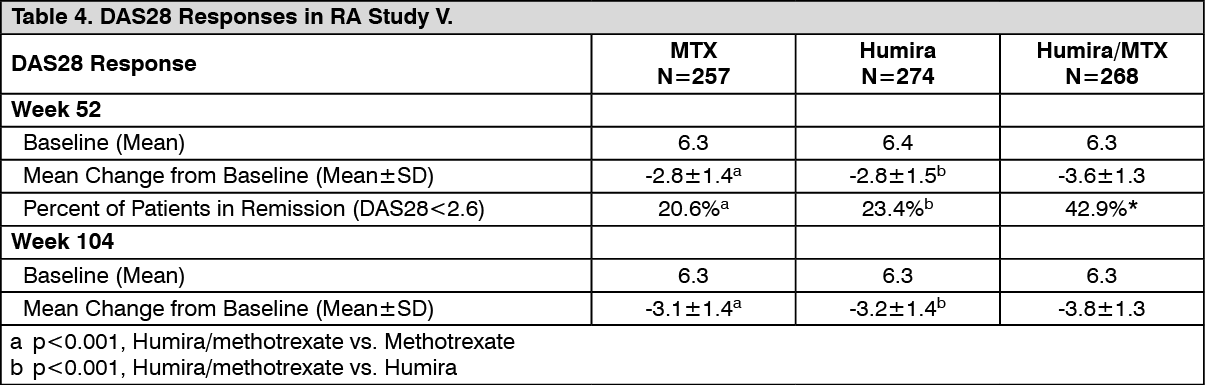 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image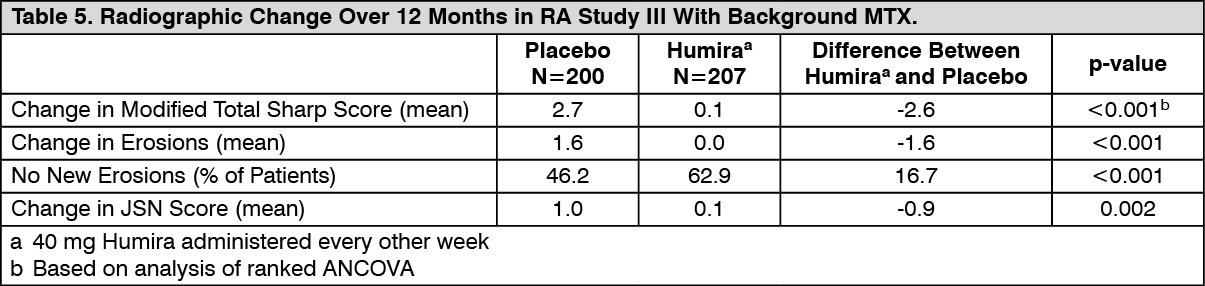 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image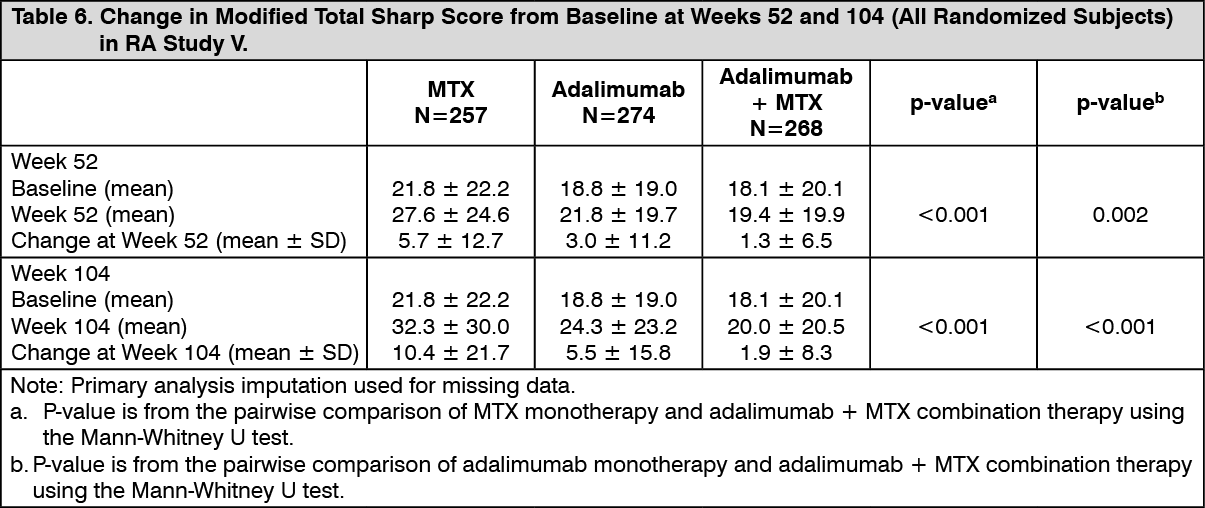 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image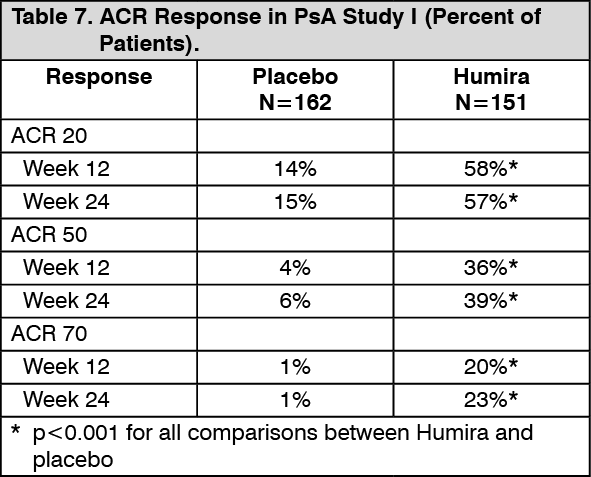 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image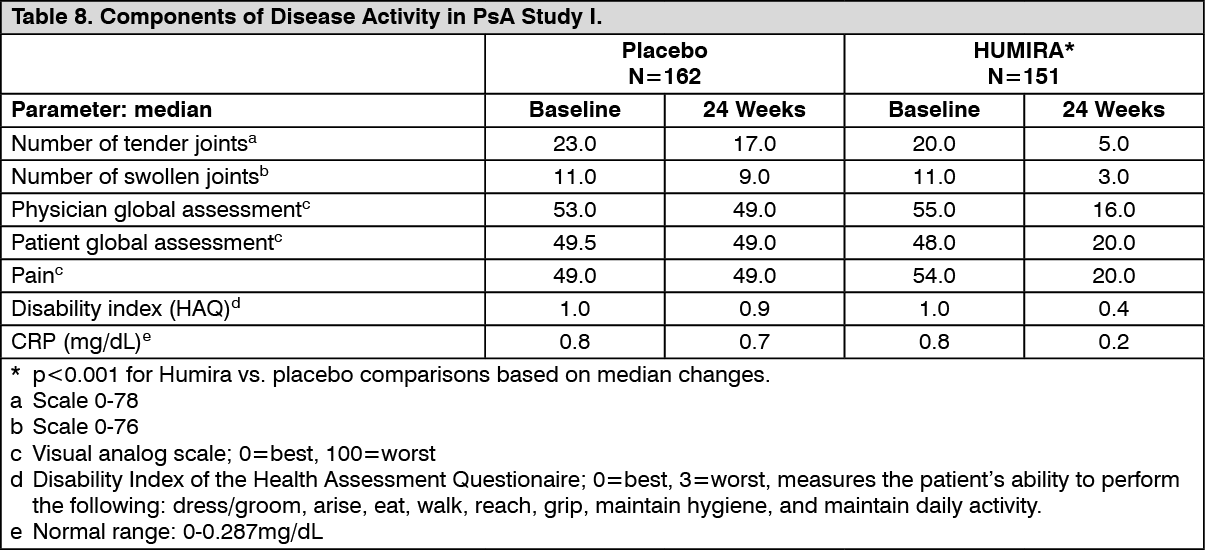 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image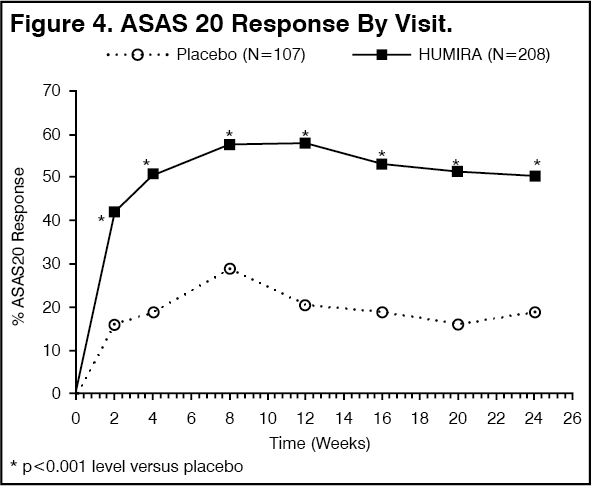 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image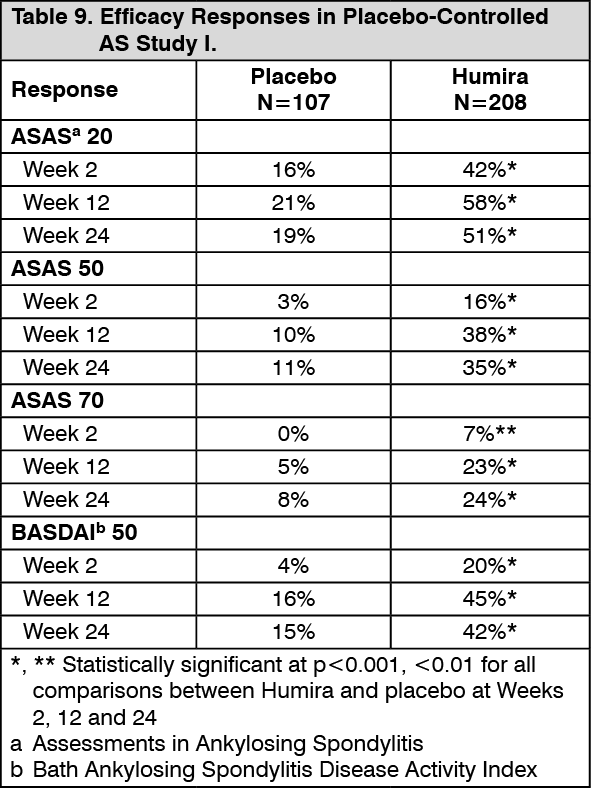 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image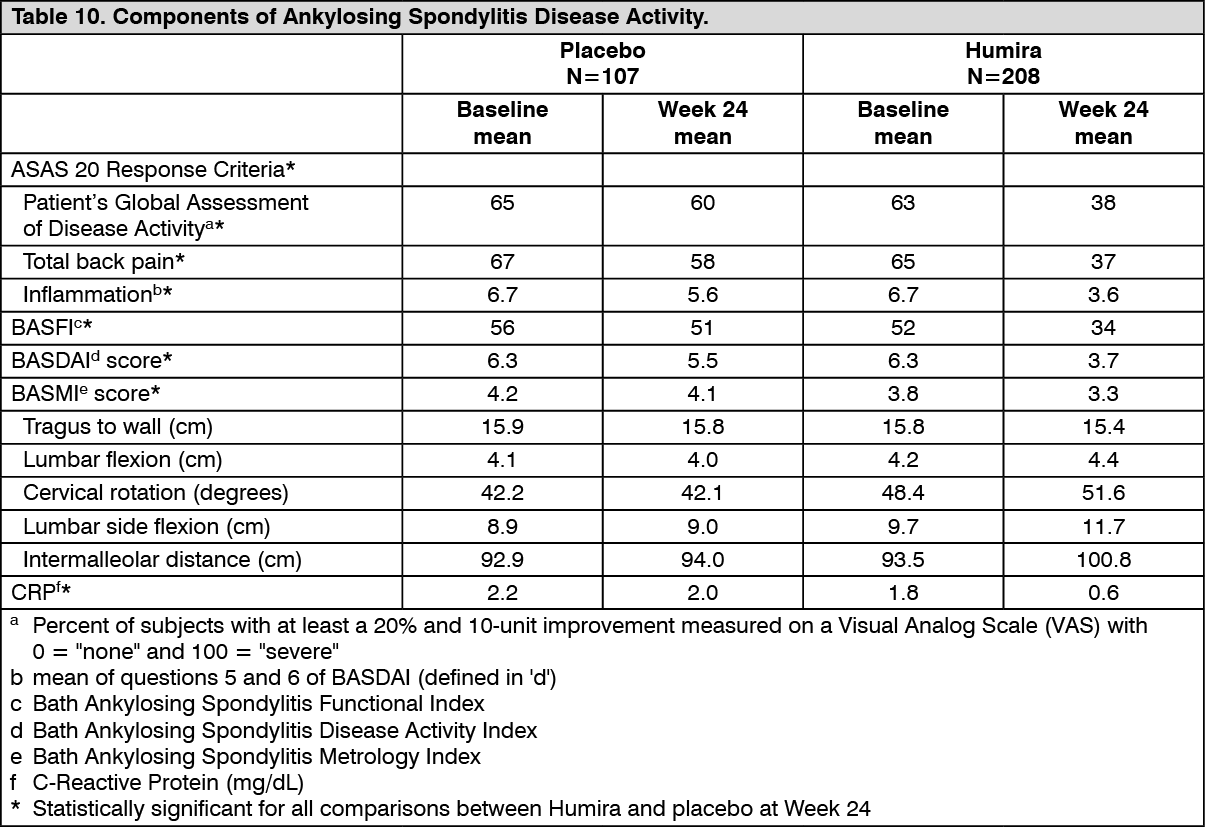 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image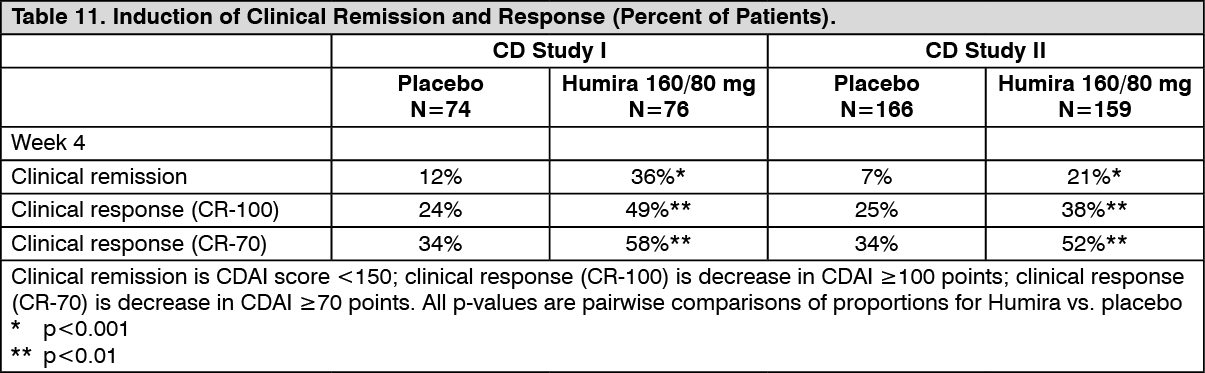 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image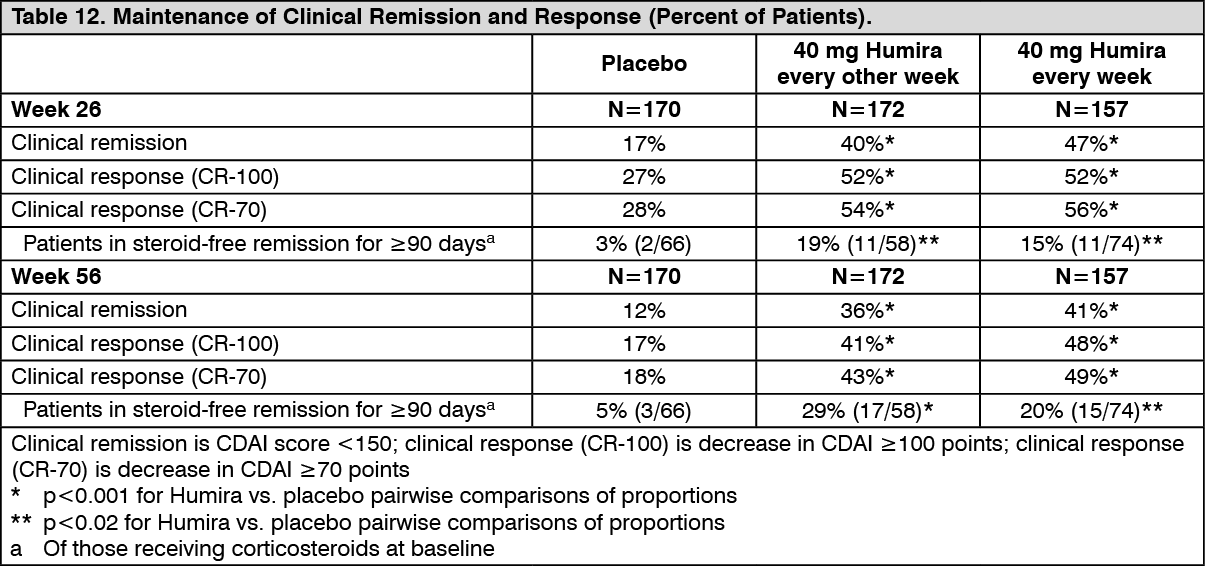 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image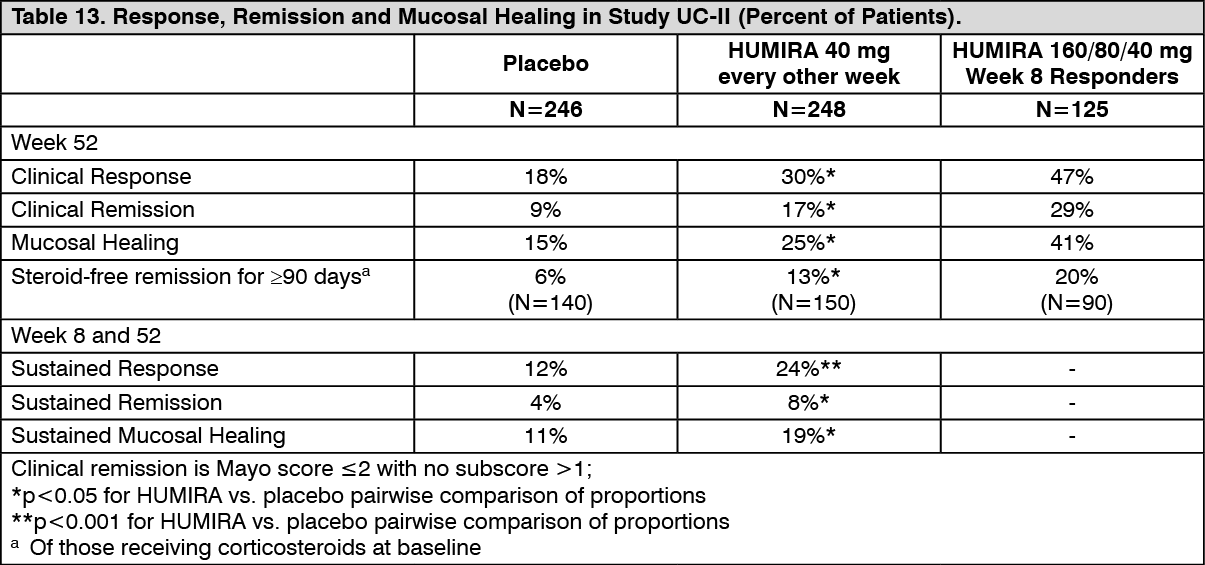 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image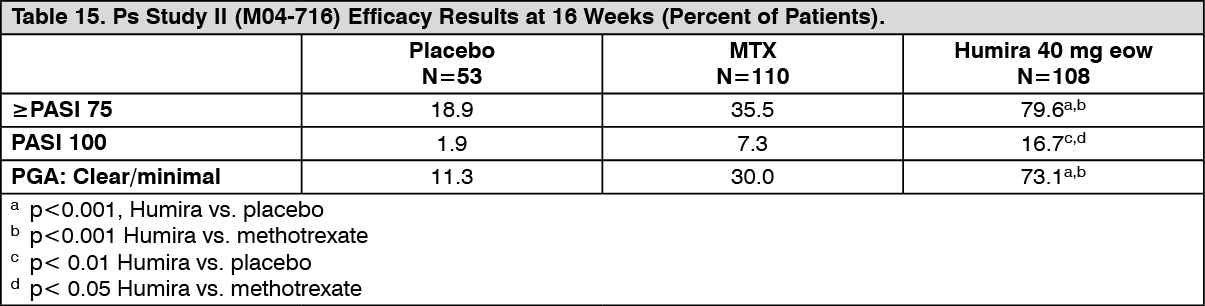 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image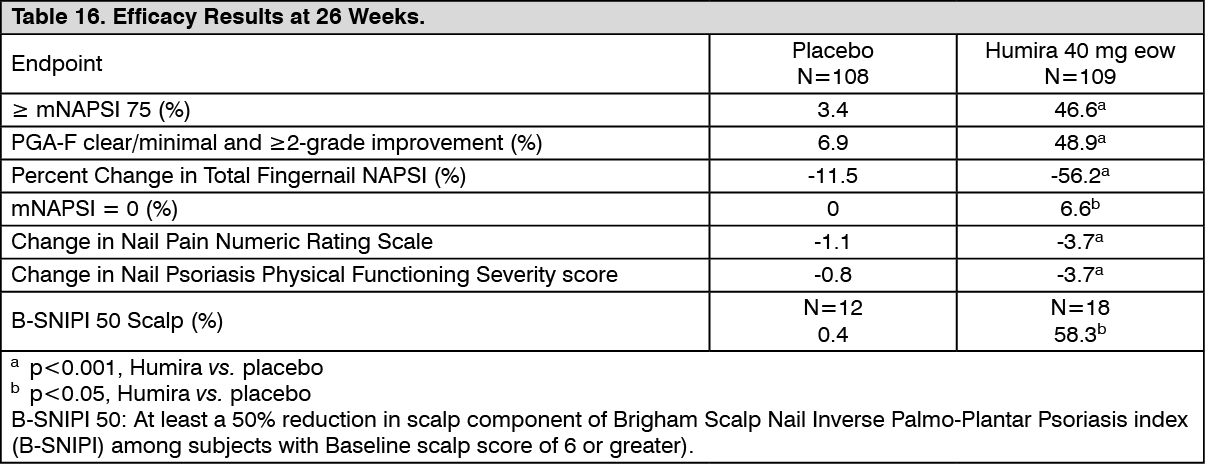 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image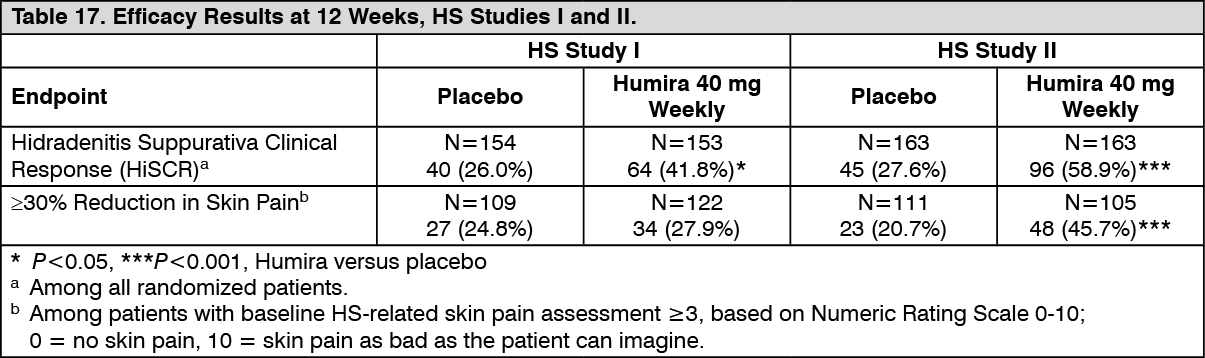 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image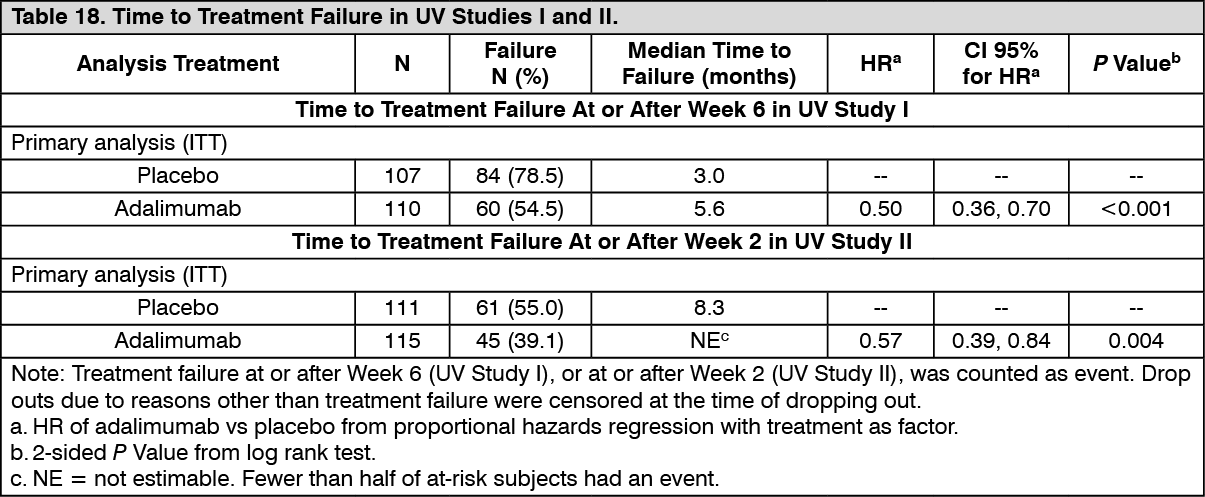 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image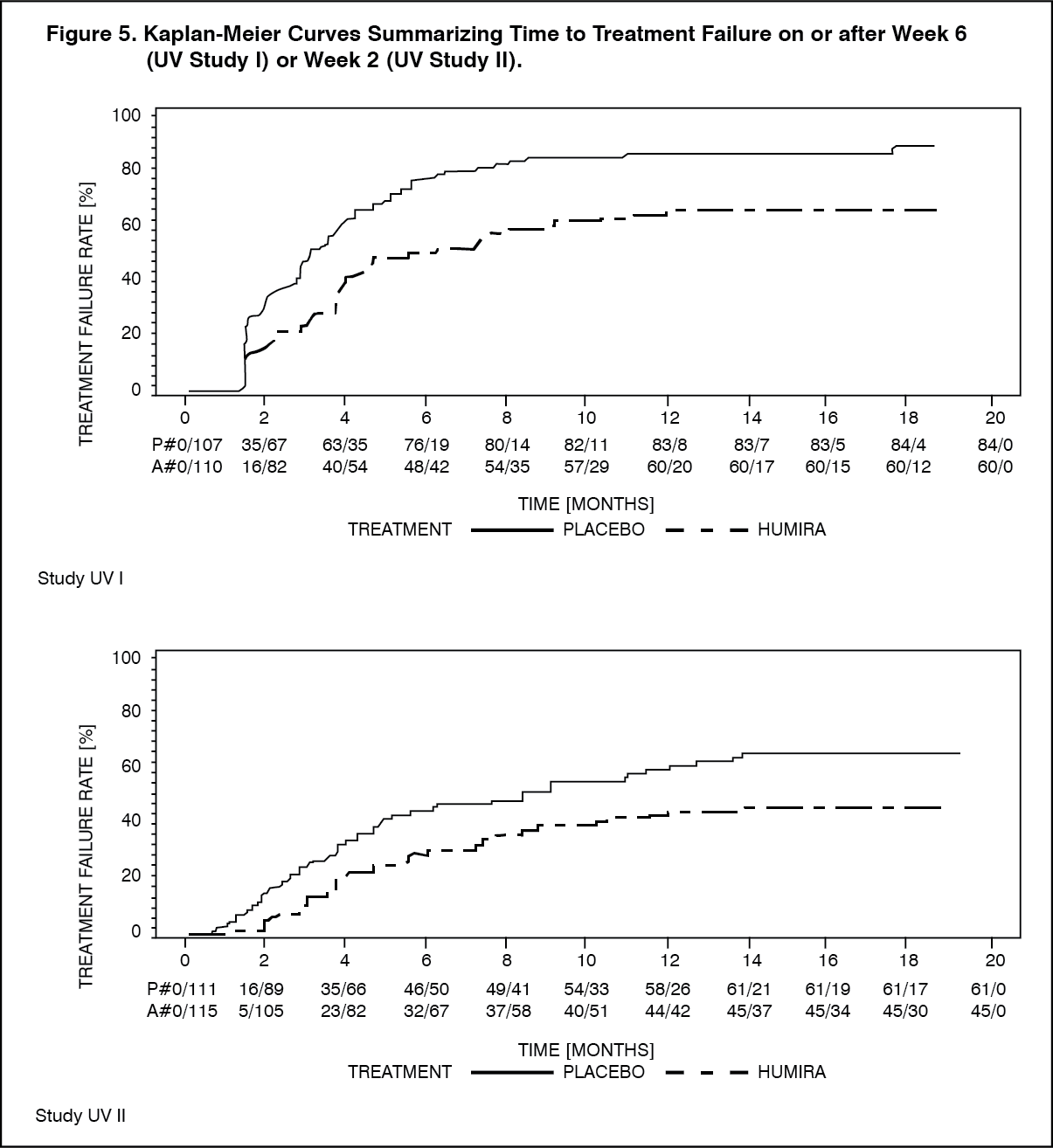 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image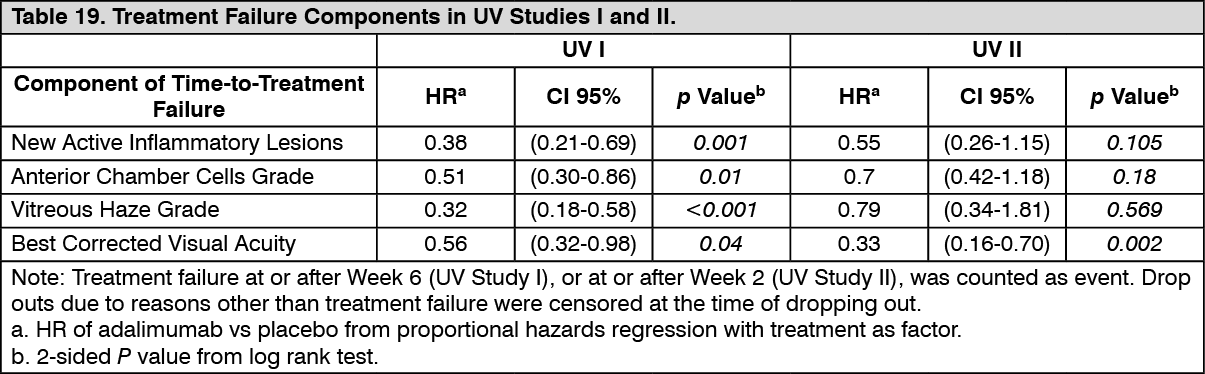 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image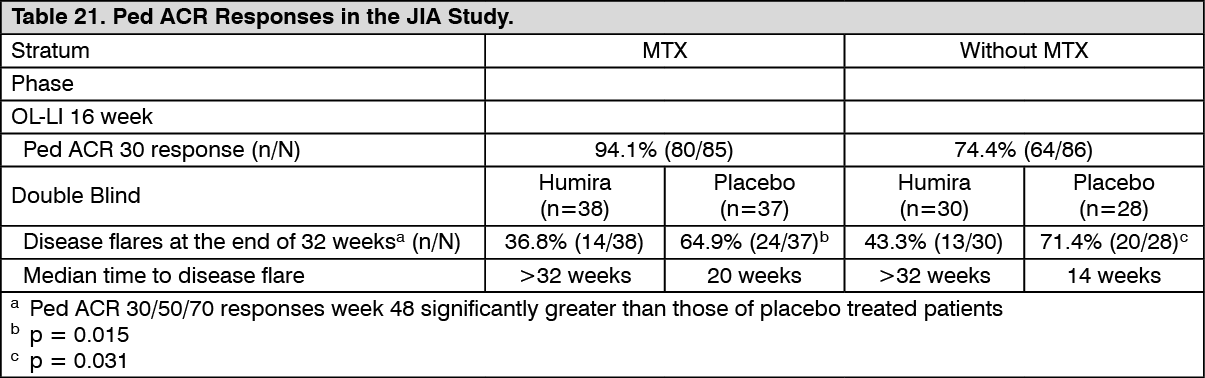 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image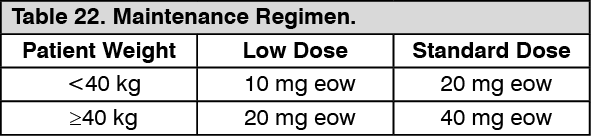 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image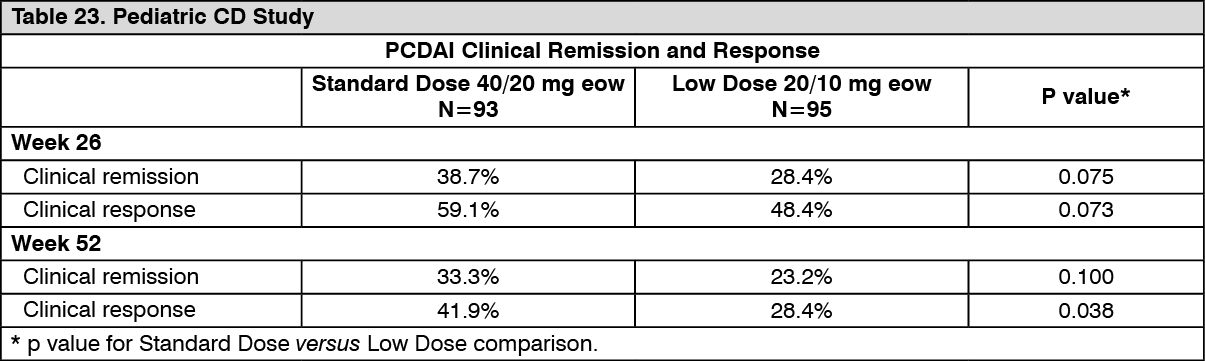 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image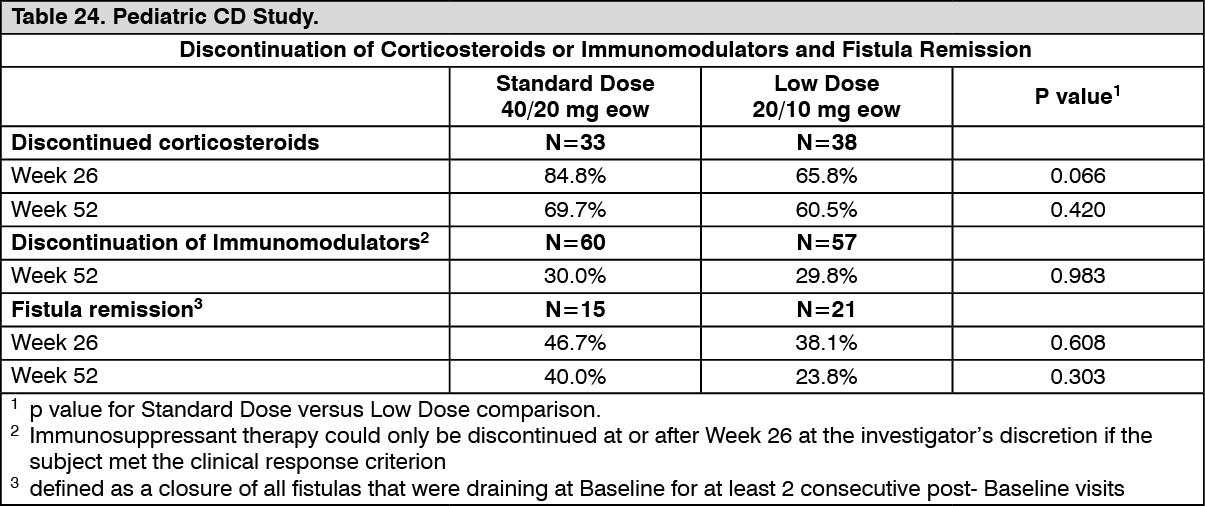 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image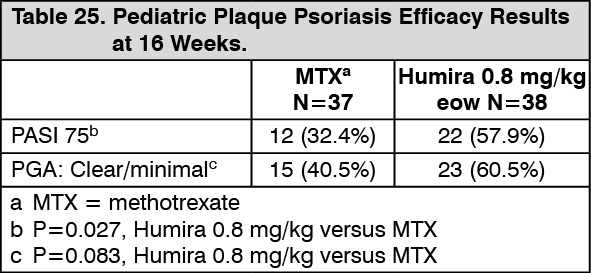 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image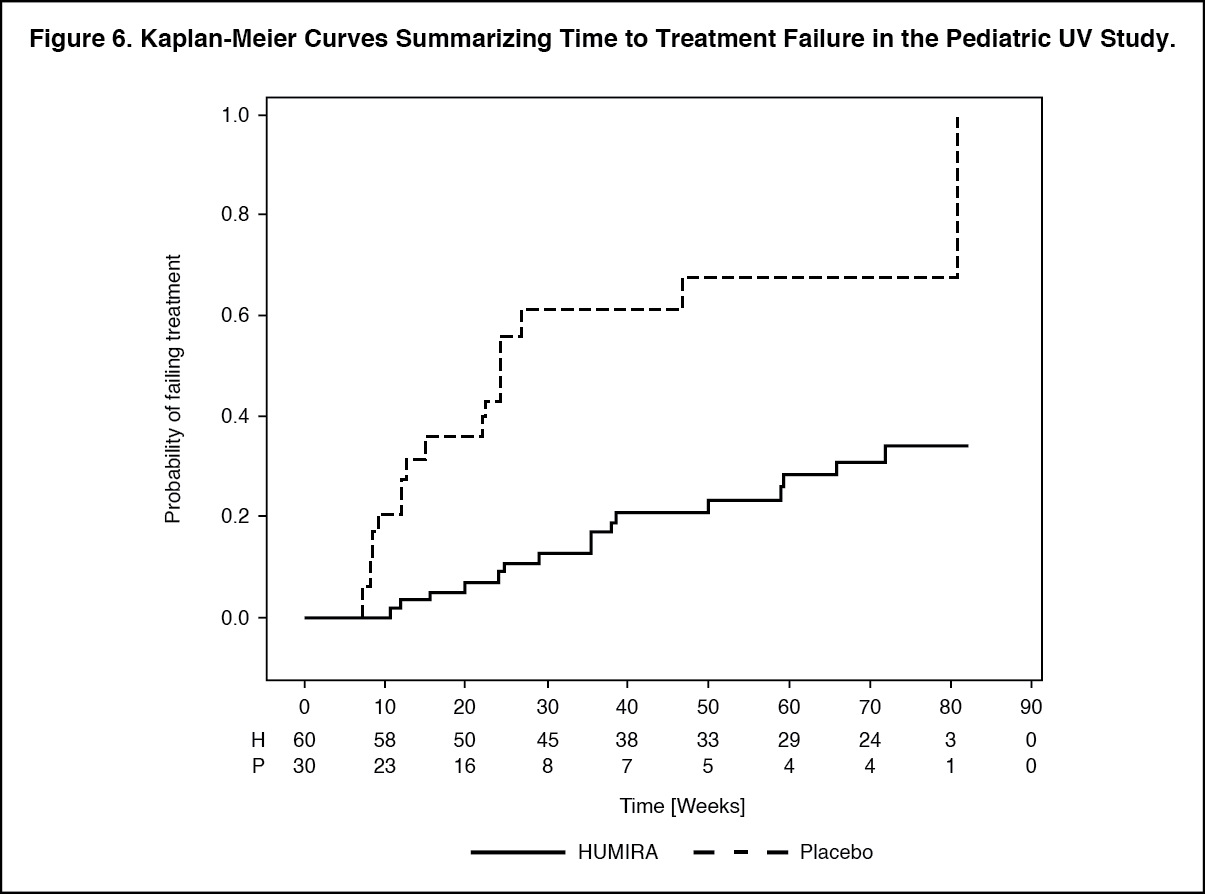 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image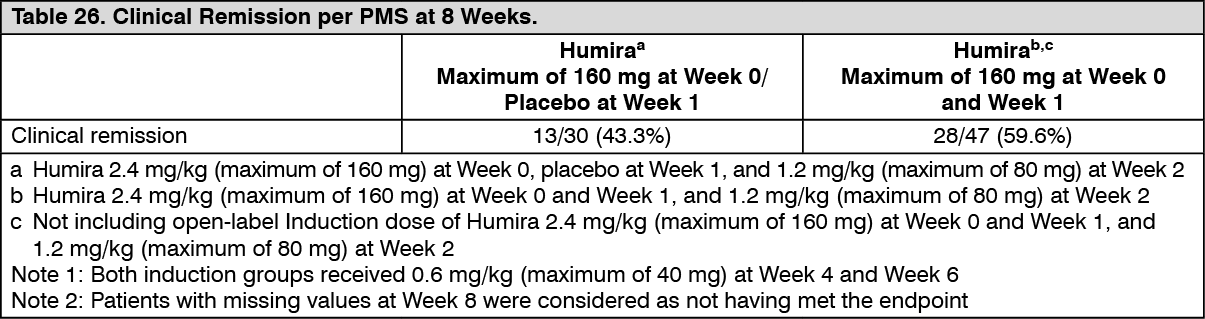 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image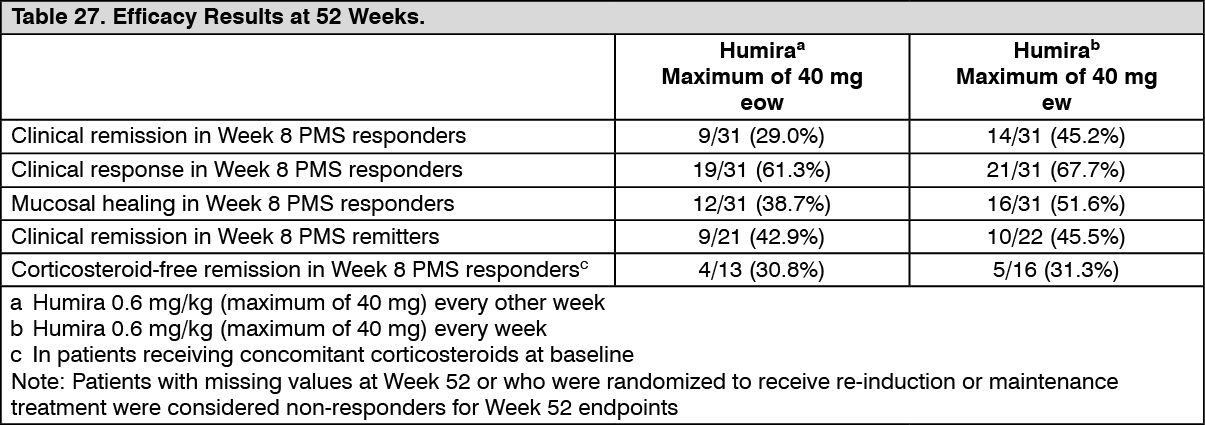 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image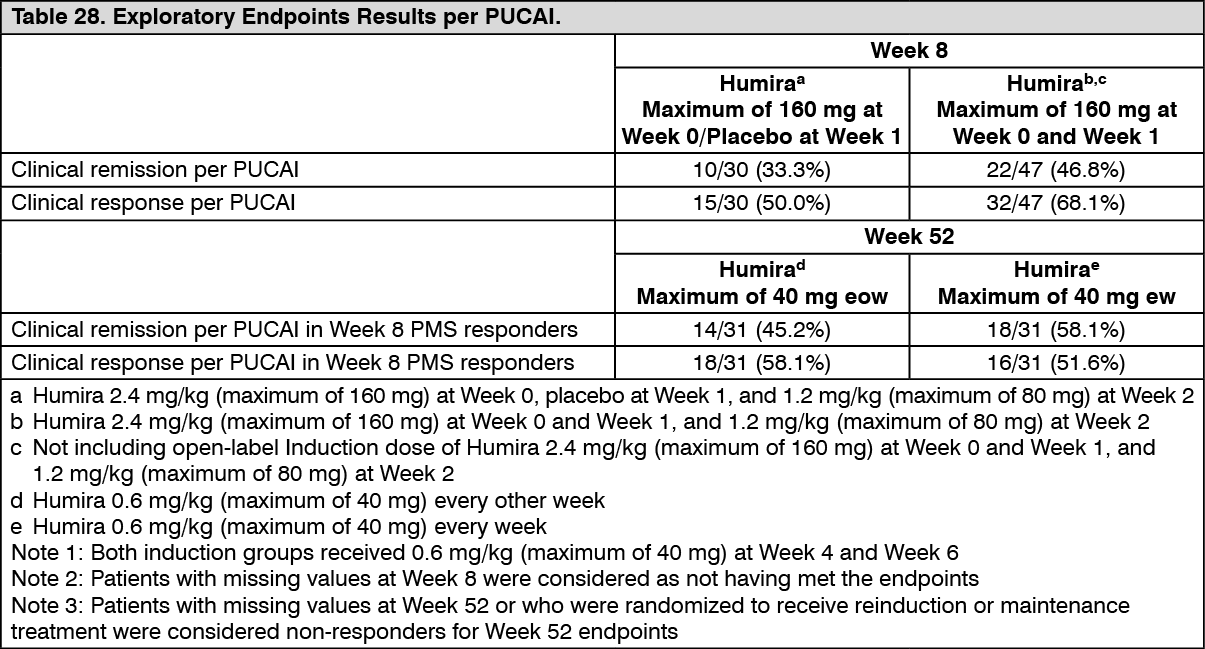 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image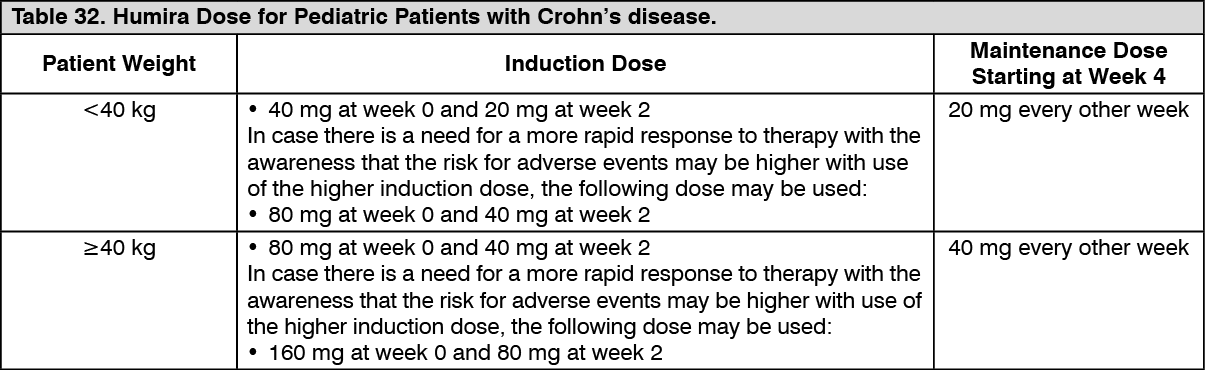 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image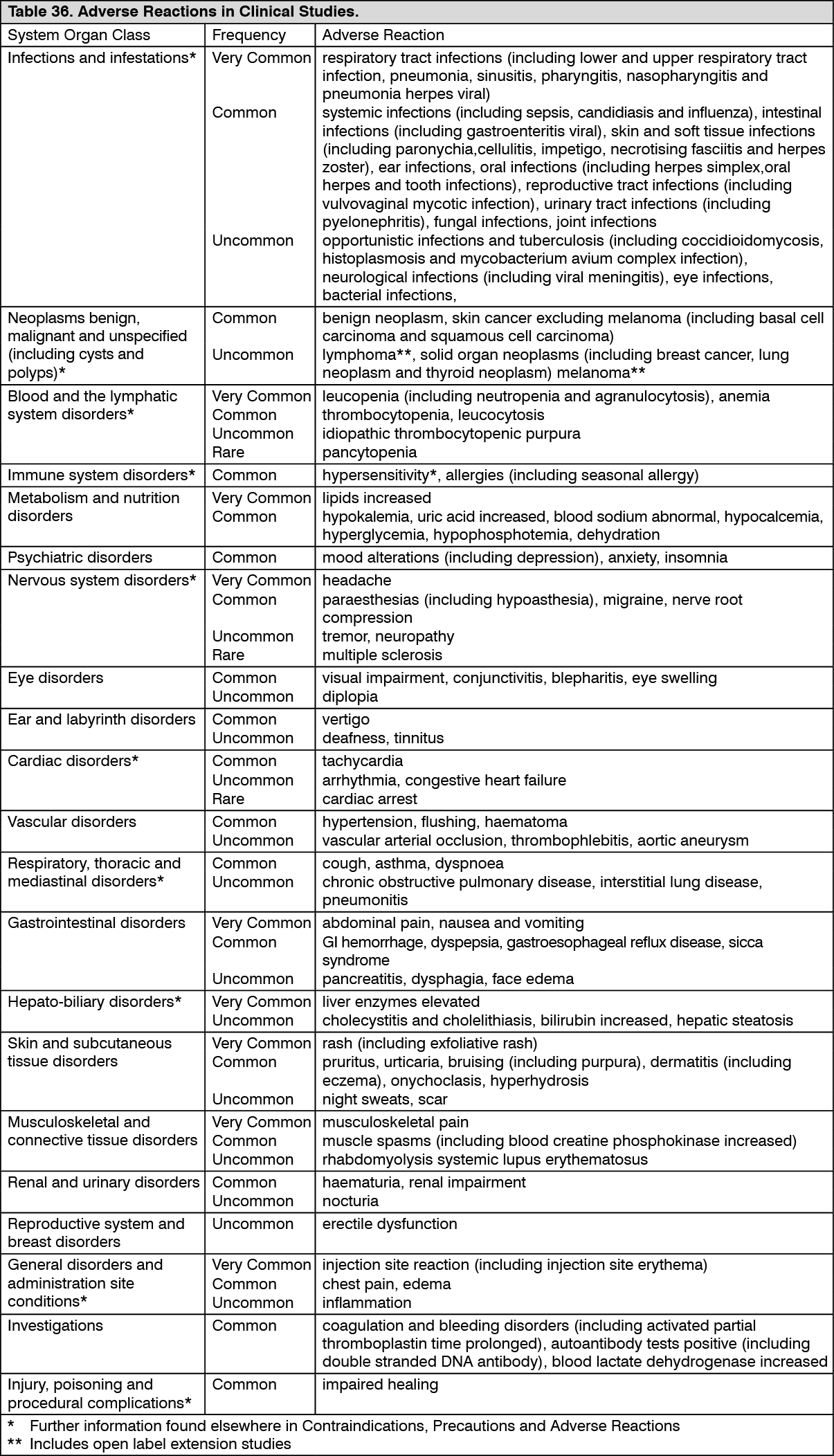 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image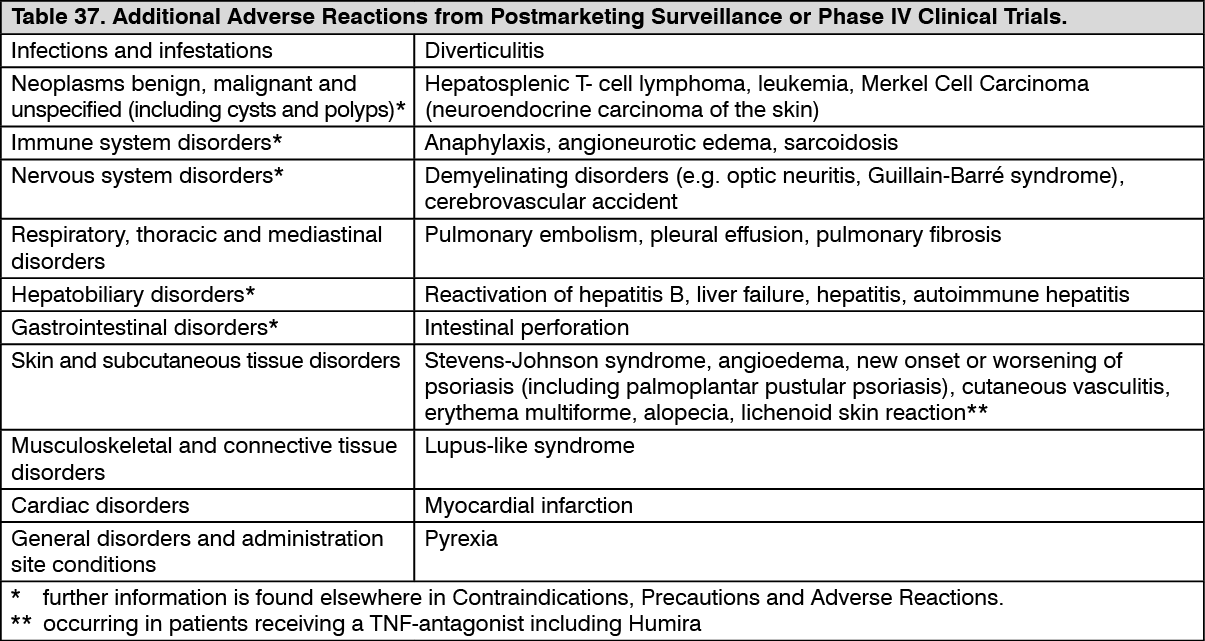 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out