



 Sign Out
Sign Out
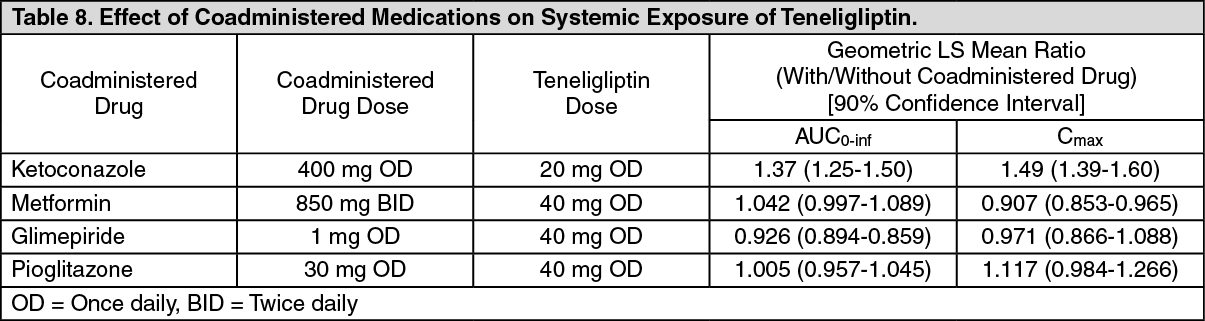
Ketoconazole (400 mg) a potent inhibitor of CYP3A4 increased Cmax and AUC of Teneligliptin by 1.37-fold and 1.49-fold, respectively which was less than 2-fold and not considered clinically significant (see Tables 8 and 9). The half-life (t1/2) of Teneligliptin was unchanged with ketoconazole coadministration. The combination of Teneligliptin with drugs and food that inhibit CYP3A4 are not expected to cause marked, clinically significant increases in the exposure to Teneligliptin. No dose adjustments are required.
The pharmacokinetics of Teneligliptin is not significantly affected by coadministration with pioglitazone or metformin. Teneligliptin does increase the exposure to metformin by a non-clinically relevant 20.5% (see Tables 8 and 9). No dosage adjustment is needed when Teneligliptin is combined with either pioglitazone or metformin.
When coadministered, neither Teneligliptin nor glimepiride affect each other's pharmacokinetic profile in any clinically meaningful way (see Tables 8 and 9). The risk of hypoglycemia may be increased when Teneligliptin is used concomitantly with insulin and insulin secretagogues such as sulfonylureas and glinides. The dosage of insulin or the insulin secretagogue should be adjusted.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image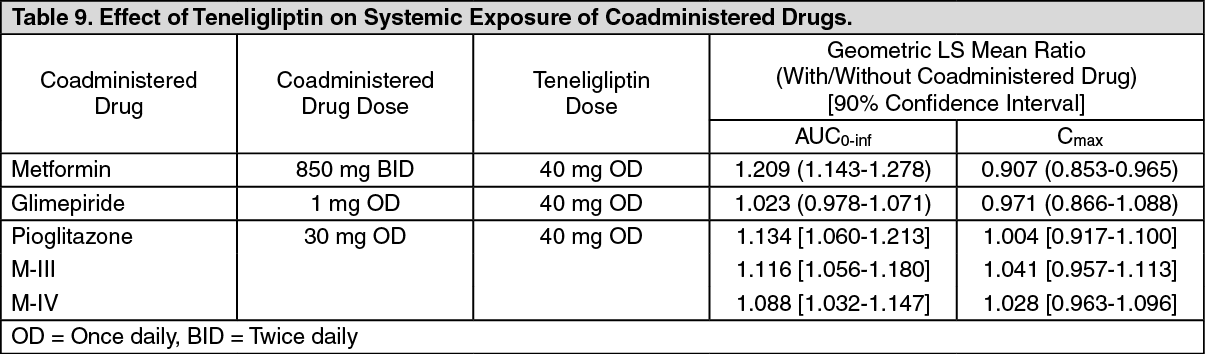 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image