Summary of the safety profile: The safety and tolerability of vildagliptin (50 mg qd, 50 mg bid and 100 mg qd) have been assessed by pooling data from more than 11,000 patients from 36 Phase II and III studies (including 3 open label studies) ranging in duration from 12 to more than 104 weeks. The studies used in this pooled analysis have assessed vildagliptin as monotherapy, add-on therapy to other oral anti-diabetic agents (metformin, TZD, SU, and insulin) and as an initial combination therapy with metformin or pioglitazone. Patients not receiving vildagliptin (all comparators group) were taking only placebo or metformin, TZD, SU, acarbose, or insulin. For the calculation of frequency of adverse drug reactions for the individual indications, safety data from a subset of pivotal controlled trials of at least 12 week's duration was considered. Safety data were obtained from patients exposed to vildagliptin at a daily dose of 50 mg (once daily) or 100 mg (50 mg twice daily or 100 mg once daily) who received vildagliptin as monotherapy or in combination with another agent.
The majority of adverse reactions in these trials were mild and transient, not requiring treatment discontinuations. No association was found between adverse reactions and age, ethnicity, duration of exposure or daily dose.
Rare cases of angioedema have been reported on vildagliptin at a similar rate to controls. A greater proportion of cases were reported when vildagliptin was administered in combination with an angiotensin converting enzyme inhibitor (ACE-inhibitor). The majority of events were mild in severity and resolved with ongoing vildagliptin treatment. In data from controlled monotherapy and add-on therapy trials up to 24 weeks in duration, the incidence of ALT or AST elevations >=3x ULN (classified as present on at least 2 consecutive measurements or at the final on-treatment visit) was 0.2%, 0.3% and 0.2% for vildagliptin 50 mg daily, vildagliptin 50 mg twice a day and all comparators, respectively. These elevations in transaminases were generally asymptomatic, nonprogressive in nature and not associated with cholestasis or jaundice.
Monotherapy: The overall incidence of withdrawal from monotherapy trials due to adverse reactions was no greater for patients treated with vildagliptin at a dose of 50 mg once daily (0.2%) or vildagliptin at a dose of 50 mg twice daily (0.1%) than for placebo (0.6%) or comparators (0.5%).
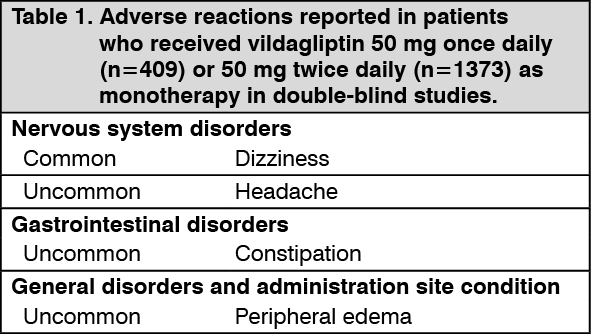
In monotherapy studies, hypoglycemia was uncommon, reported in 0.5% (2 of 409) of patients treated with vildagliptin 50 mg once daily and 0.3% (4 of 1,373) of patients treated with vildagliptin 50 mg twice daily compared to 0.2% (2 of 1,082) of patients in the groups treated with an active comparator or placebo, with no serious or severe events reported.
Vildagliptin is weight neutral when administered as monotherapy. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Long term clinical trials of up to 2 years did not show any additional safety signals or unforeseen risks with vildagliptin monotherapy.
Combination with metformin: In clinical trials with the combination of vildagliptin + metformin, 0.4% of patients withdrew due to adverse reactions in the vildagliptin 50 mg once daily + metformin treatment group, and no withdrawal due to adverse reactions was reported in either the vildagliptin 50 mg twice daily + metformin or the placebo + metformin treatment groups. (See Table 2.)
Click on icon to see table/diagram/image
Long term clinical trials of up to more than 2 years did not show any additional safety signal or unforeseen risks when vildagliptin was added on to metformin.
When vildagliptin was studies as an initial combination therapy with metformin, no additional safety signal or unforeseen risk was observed.
Combination with a sulfonylurea: In clinical trials with the combination of vildagliptin 50 mg + glimepiride, the overall incidence of withdrawals due to adverse reactions was 0.6% in the vildagliptin 50 mg + glimepiride treatment group versus 0% in the placebo + glimepiride treatment group.
In clinical trials, the incidence of hypoglycaemia when vildagliptin 50 mg once daily was added to glimepiride was 1.2% versus 0.6% placebo + glimepiride. No severe hypoglycemic events were reported in the vildagliptin arms.
At the recommended dose of 50 mg, vildagliptin is weight neutral when administered in combination with glimepiride. (See Table 3.)
Click on icon to see table/diagram/image
Combination with a thiazolidinedione: In clinical trials with the combination of vildagliptin and a thiazolidinedione, 0.7% of patients withdrew for adverse reactions in the vildagliptin 50 mg once daily + pioglitazone group, and there were no withdrawals due to adverse reactions reported in either the vildagliptin 50 mg twice daily + pioglitazone or the placebo + pioglitazone treatment groups.
In clinical trials, no hypoglycaemia events were reported in patients receiving vildagliptin 50 mg once daily + pioglitazone 45 mg, hypoglycaemia was uncommon in patients receiving vildagliptin 50 mg twice daily + pioglitazone 45 mg (0.6%) but common in patients receiving placebo + pioglitazone 45 mg (1.9%). No severe hypoglycemic events were reported in the vildagliptin arms.
In pioglitazone add-on study, the change in body weight compared to placebo was + 0.1 kg and +1.3 kg for vildagliptin 50 mg daily and vildagliptin 50 mg twice daily, respectively.
The incidence of peripheral edema when vildagliptin was added to a maximum dose of background pioglitazone (45 mg once daily) was 8.2% as 50 mg once daily and 7.0% as 50 mg twice daily compared to 2.5% for background pioglitazone alone. The incidence of edema when vildagliptin was added to pioglitazone as dual initial therapy in drug naïve patients was, however, less than for pioglitazone alone (50 mg once daily 3.5%, 50 mg twice daily 6.1% vs. pioglitazone 30 mg 9.3%). (See Table 4.)
Click on icon to see table/diagram/image
Combination with insulin: In controlled clinical trials using vildagliptin 50 mg twice daily in combination with insulin, with or without concomitant metformin, the overall incidence or withdrawal due to adverse reactions was 0.3% in the vildagliptin treatment group and there were no cases of withdrawal in the placebo group.
The incidence of hypoglycemia was similar in both treatment groups (14.0% in the vildagliptin group versus 16.4% in the placebo group). Two patients reported severe hypoglycemic events in the vildagliptin group, and 6 patients - in the placebo group.
At the end of the study, the effect on mean body weight was neutral (+0.6 kg change from baseline in the vildagliptin group and no weight change in the placebo group). (See Table 5.)
Click on icon to see table/diagram/image
Combination with metformin and SU: There were no cases of withdrawal reported due to adverse reactions in the vildagliptin + metformin + glimepiride treatment group versus. 0.6% in the placebo + metformin + glimepiride treatment group.
The incidence of hypoglycaemia was common in both treatment groups (5.1% for the vildagliptin + metformin + glimepiride vs. 1.9% for the placebo + metformin + glimepiride). One severe hypoglycemic event was reported in the vildagliptin group.
At the end of the study, the effect on mean body weight was neutral (+ 0.6 kg in the vildagliptin group and -0.1 kg in the placebo group). (See Table 6.)
Click on icon to see table/diagram/image
Adverse drug reactions from spontaneous reports and literature cases - Post-marketing Experience (frequency not known): The following adverse drug reactions have been derived from postmarketing experience via spontaneous case reports and literature cases. Because these reactions are reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency, which is therefore categorized as not known.
Hepatitis reversible upon drug discontinuation; Urticaria, bullous and exfoliative skin lesions, including bullous pemphigoid; Pancreatitis; Arthralgia, sometimes severe.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image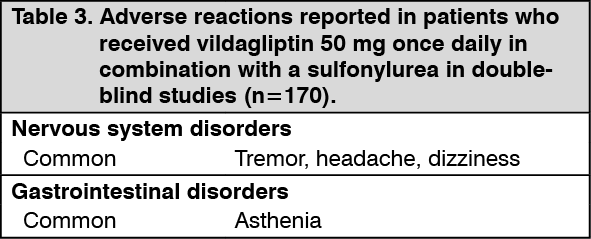 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image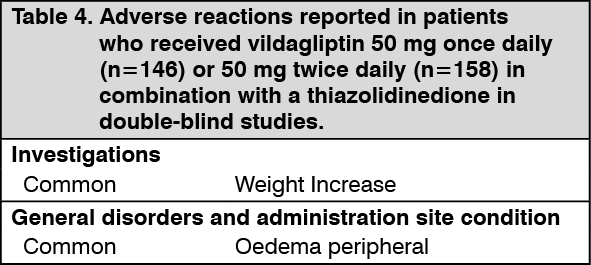 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image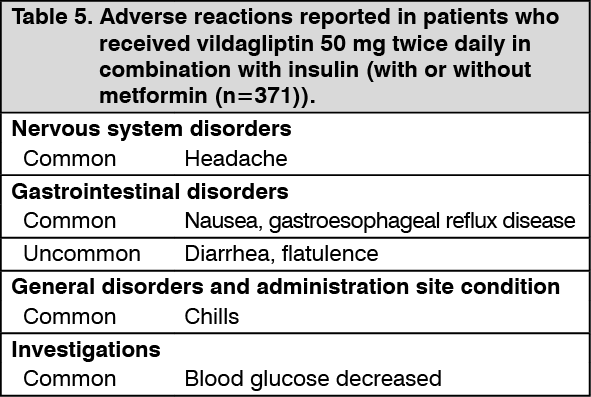 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image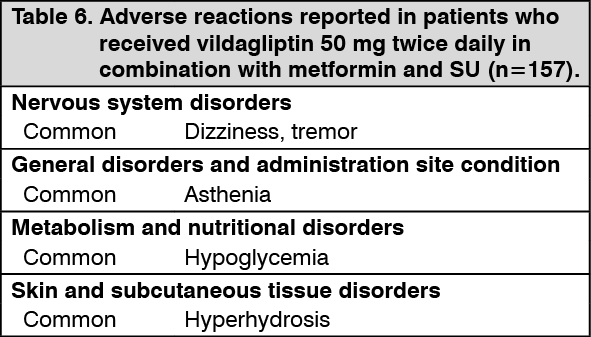 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out